
Abstract
Patients with neurocysticercosis, a common infection of the central nervous system caused by Taenia solium, have been reported to develop neuropsychiatric complications. We report a unique case of recurrent psychosis caused by neurocysticercosis in a 37-year-old El Salvador immigrant woman and discuss the underlying pathophysiological mechanisms of the complications. We reviewed published case reports of neurocysticercosis that presented with psychotic features and compared their diagnostic evaluation, the underlying pathophysiology of complications and treatment regimen with our case. This review concludes that neurocysticercosis should be considered in the differential diagnosis of patients presenting with psychosis with a history of residence in an endemic area.
Introduction
Neurocysticercosis (NCC) is the most severe form of cysticercosis to cause infection of the central nervous system (CNS) and is the leading cause of acquired epilepsy in humans globally. 1 The total number of individuals suffering from NCC is about 2.56–8.30 million worldwide, while it is estimated that the total symptomatic cases in endemic regions are roughly 400,000. 1 NCC is endemic in Latin America, Asia, Africa and Central Europe, where 30% of all epilepsy cases are caused by it. 2 Recently, it is being diagnosed more often in the United States due to increased migration. 3 However, very little attention has been paid to its surveillance, prevention and treatment. 4
NCC is caused by the feco-oral transmission of Taenia solium eggs. Humans ingest these parasite eggs, and their embryos invade the mucosa of the small intestine, from where they enter the circulation and subsequently into the CNS. 5 NCC is classified into six clinical syndromes: asymptomatic, parenchymal, intraventricular, subarachnoid, spinal and ocular forms. 5 Clinical manifestations of NCC depend on the location of the lesions and the number of cysts; however, commonly associated neurological symptoms are chronic headache, increased intracranial hypertension (ICH) with symptoms of vomiting, nausea, dizziness and changes in vision and focal neurological deficits. 3 NCC may also cause psychiatric manifestations like depression and psychosis. 6 In psychosis, a person loses contact with reality; symptoms include delusions, hallucinations, bizarre behavior and incoherent speech. 7
Psychosis is a rare presenting complaint in NCC. One in twenty NCC patients present with psychosis, and only 5% of NCC patients present with psychosis in the emergency department (ED) 6 (2004). NCC remains underdiagnosed in most patients as it is asymptomatic in approximately 50% of cases. 8 The variability in its clinical presentation and neuropathology makes it challenging to diagnose, highlighting the importance of thorough history taking, early detection and treatment. In this literature review, we present a rare case of recurrent psychosis, along with a detailed review of previous case reports of psychotic presentation with NCC, along with associated features, diagnostic evaluation and treatment options. This review will help clinicians recognize and treat NCC presenting with psychotic symptoms.
Case presentation
A 37-year-old female immigrant from El Salvador presented with a headache, strange behavior, auditory hallucinations and paranoid delusions to the ED. She admitted to being depressed, having a decreased appetite, sleep deprivation and forgetfulness. She was admitted to the medical floor to rule out delirium, and the consultation–liaison (CL) team was contacted. When the CL team saw the patient, she was still paranoid, delusional and experiencing auditory hallucinations. A review of systems revealed no evidence of a focal neurological deficit. The general physical examination revealed no abnormalities. On mental status examination, her appearance was unkempt; the behavior was strange with poor eye contact. She described her mood as “depressed,” and her affect was constricted. Her thought process was concrete with circumstantiality at times; thought content was positive for paranoid delusions, “her husband making plans with his girlfriend to murder his wife and daughters.” On perceptions disturbances, she was positive for auditory hallucinations. She lacked insight/judgment, but her orientation and memory were intact. The Mini Mental State Examination (MMSE)9,10 score was 27. The CL team began her on risperidone 1 mg two times a day (BID) targeting psychotic symptoms. Collateral history revealed that the patient had a history of generalized tonic–clonic seizures (GTCSs), for which an antiepileptic medication was started. During the same period, she was diagnosed with NCC and was prescribed albendazole 400 mg BID for 28 days, but she did not take the medication due to a lack of insurance. During the current hospitalization, the medical team obtained a computed tomography (CT) scan and a magnetic resonance imaging (MRI) of the brain. The CT brain indicated hypodense regions in the right frontal and parietal lobes, as well as abnormal and irregular calcifications (Figure 1). The MRI revealed encephalomalacia in the upper right frontal and parietal lobes, as well as a rim of adjacent gliosis. On the following day of her admission, she was cleared by the medical team and transferred to psychiatry for psychosis. Risperidone was increased to 6 mg/day in two divided doses of 3 mg BID due to the patient’s persistent psychotic symptoms. After her psychosis had resolved, she was discharged with an aftercare follow-up appointment at a nearby facility.

Computed tomography scan of the brain showing areas of calcified lesions; inactive parenchymal neurocysticercosis.
Discussion
This article aims to highlight the difficulties in diagnosing and treating NCC in patients with psychosis in the United States or other NCC-prevalent countries. In addition to the case, presented here, we conducted a literature review of 21 similar cases (Table 1). Thirteen case reports came from India, the remaining instances came from Nepal, Brazil, Haiti, Portugal and Africa. Thirteen were male, and eight were female. Fifteen cases were between the ages of 21 and 50 years, four were between the ages of 10 and 20 years, and two were elderly (>51 years). The current case was diagnosed with NCC and presented to the ED with psychosis in 2017. However, due to non-compliance, she explained to the ED again after 3 years with psychosis. This demonstrates a high probability of recurrence of NCC if the disease is not treated optimally or if patients do not adhere to their recommended medication. Cases were reported in the literature where patients were non-compliant and presented with psychosis, most likely due to reinfection.16,28,29 In NCC, psychiatric symptoms may be triggered by inflammatory injury to the brain caused by degenerating cysts and mechanical alterations in cerebrospinal fluid (CSF) pressure. 6 The classification of psychiatric manifestations is based on the location of the lesion 6 (Table 2). The parietal lobe is involved in many neuropsychological functions, including its engagement with the frontal lobe to store and retrieve verbal information. Both the parietal and frontal lobes have solid anatomical connections and are activated simultaneously in performing cognitive tasks. 14 In addition to changes in the cortical areas responsible for the normal physiological function of hearing and vision, the limbic system is also involved in developing psychotic phenomena such as auditory and visual hallucinations. However, limbic structures play a central role in the psychopathology of psychosis, involving frontal and parietal structures. 26
Case reports of neurocysticercosis causing psychosis.

OD: once a day; BID: two times a day; TID: three times a day; QID: four times a day; IV: intravenous; IM: intramuscular; MMSE: Mini-Mental State Examination; GTCS: generalized tonic–clonic seizure; QHS: every night at bedtime; CT: computed tomography.
Psychiatric manifestations based on site of lesion.
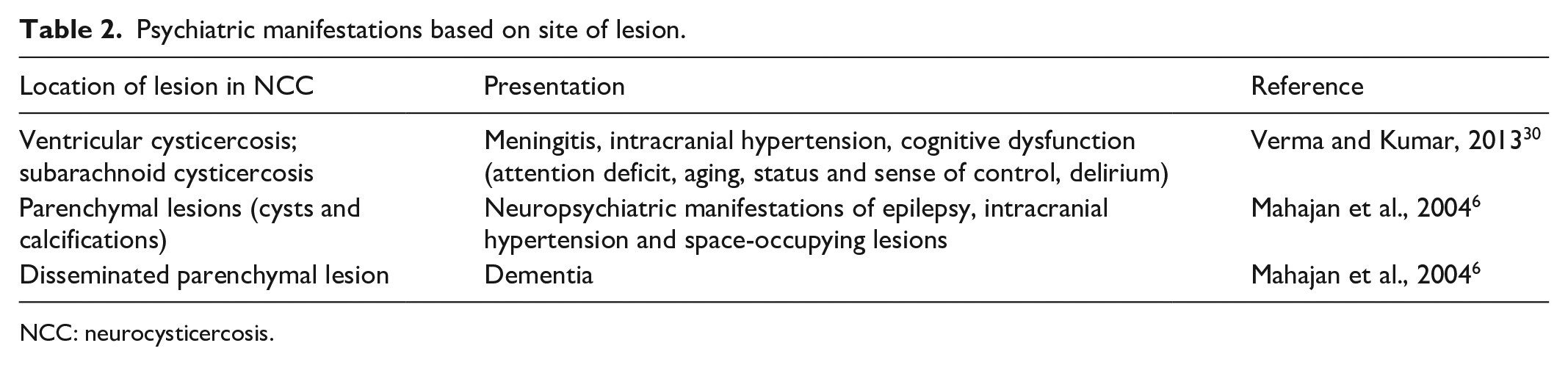
NCC: neurocysticercosis.
The case reports support the high frequency of neuropsychiatric symptoms in patients with NCC. Ms Ana had headaches with psychotic symptoms, as recorded in nine other case reports.6,12,18,23,24,26,30,31 Many intracranial infections cause headaches. 32 Most headaches subside once the infection is resolved, but chronic post-infectious headaches can last for months. 33 Infectious headaches require antimicrobial therapy due to viable microorganisms. 33 People with calcified parenchymal brain cysticercosis are more likely to suffer from primary headache disorders than head trauma and cerebrovascular disease. 34
The current case suffered from depression, which was also reported in three other case reports.6,23,26 Depression generally accounts for 56.2% of NCC cases. 35 It has been associated with various neurobiological mechanisms, such as changes in neural biology, abnormal neuronal adaptive capability, decreased neurotransmitter levels and endocrine variations. 36 Neuroinflammation is also thought to cause depression. 37 Although there is no established causal relationship between neuroinflammation and depression, studies show that neuroinflammation caused by various diseases alters an individual’s risk profile for developing depression either immediately or later in life. 38
One study examined the prevalence of depression in NCC patients. 39 The researchers reported depression rates of 83% in the NCC group with epilepsy, 88% in the NCC without epilepsy group, 92% in epilepsy without NCC group and 100% in the epilepsy without headache group. The study found a link between moderate-intensity depression and chronic illnesses. Another study that measured the activity of NCC disease through total protein levels in the cerebrospinal fluid (CSF-TP) found an inverse relationship between NCC and the presence of depression, with patients with higher CSF-TP readings having minimal or no depression. 19
Seizures are NCC’s most common neurological manifestation in intraparenchymal, enhancing and discrete lesions. 3 Nine cases had GTCSs, one had focal seizures, and one case report presented with partial seizures.2,3,5,8,15,26,27,29,30,40 Focal seizures occur when cysticercosis invades the temporal-limbic area of the cerebral cortex, whereas GTCS occurs when the cerebral cortex develops multiple parenchymal cysts and calcifications.2,5 GTCS is caused by changes in CSF pressure and inflammation in the brain’s frontal lobe.29,26,40 Similarly, genetic predispositions to seizures have been observed in patients with NCC. 21 Matrix metallopeptidase-9 (MPP-9) is an enzyme involves NCC calcified cysts, triggering seizures. 21 Furthermore, Toll-like receptors (TLRs) are thought to be responsible for the brain’s immune response to NCC, resulting in seizures. 21
Diagnostic imaging
Imaging modalities like CT (with contrast) and MRI are the mainstays for the diagnosis of NCC. When imaging was performed to look for anatomical causes, CT imaging revealed multiple hypodense lesions or cysts with calcifications in both the right frontal and parietal lobe, consistent with cysticercus cellulose. This was also reported by other case reports.12,20,24,40 MRI showed blurred cortical margins in the parietal region. Fourteen case reports showed scattered lesions all over the cerebrum.6,13,17,18,22,23,26,28–31,41,42 Features consistent with cysticercus racemosus were reported by only one case report. 42 Imaging techniques like CT and MRI have considerably improved the accuracy of diagnosing NCC by providing information about the number and location of the lesions. 43 The appearance of these lesions on imaging depends on whether the cysticerci are living, degenerating or dead. Living cysticerci appear as well-marginated cysts with no surrounding inflammation; degenerating cysticerci are irregularly shaped with surrounding inflammation while dead or calcified cysticerci look like hyperdense lesions but are smaller without any surrounding edema or contrast enhancement. 44 False negatives are commonly seen in CT and MRI in the remission phase of NCC. 45
Antibody testing
Other tests that can be used to diagnose NCC are enzyme-linked electroimmunotransfer blot (EITB) as mentioned in previous case reports and enzyme-linked immunosorbent assay (ELISA) test.22,23,29– 31 The EITB has a sensitivity ranging from 90% to 100% and a specificity of 100% in individuals with multiple cysticerci, while the sensitivity drops to 65% in patients with a single cyst. 25 The ELISA test measures immunoglobulin G (IgG) antibodies against either the somatic antigen or the excretory–secretory (ES) antigens. 46 The sensitivity of the ELISA test for somatic antigen is 76% in serum and 75% in CSF samples, while specificity is 97% in serum and 96% in CSF. 46 The sensitivity of the ELISA test for ES antigen is 88% in serum and 64% in CSF, while specificity is 96% in serum and 97% in CSF. 46
Treatment in case studies
The treatment modalities used to treat NCC psychosis in our patient were albendazole, an antiparasitic and haloperidol, an antipsychotic. Similarly, albendazole was prescribed in 11 out of the other 20 cases.12,13,18,20,22,23,24,29,41,47 Other medications used to treat NCC were dexamethasone in 11 cases to reduce brain edema caused by perilesional inflammation.12,18,20,22,23,29,41,47 Praziquantel was used in three cases.26,28,40 Ventriculoperitoneal shunting was performed to improve symptoms of hydrocephalus in three cases.24,26,42
Although our patient was discharged with a complete recovery similar to most other case reports, only one patient succumbed to his illness in the intensive care unit (ICU) after 1 month of extensive treatment due to profuse cerebral edema/diffuse global hypoxic ischemia. 47 These treatments mentioned above are effective against NCC. However, continuation may be difficult if the symptoms do not resolve sooner or due to side effects associated with antipsychotic medicines. Non-compliance is an essential factor to consider for the recurrence of NCC in these patients. Non-compliance can be attributed to the lower socio-economic status of some of these patients rendering them incapable of acquiring the recommended treatments. Several cases of NCC psychosis have shown that long-term therapy, particularly with antipsychotics (haloperidol, olanzapine, risperidone, aripiprazole), continued for approximately 6 weeks to 22 months.2,3,22,26,28 When the treatment was interrupted for any reason, the symptoms of psychosis resurfaced, resulting in rehospitalizations for those individuals.2,3,22,26,28
Lesion localization and psychosis
Koropouli E et al. 48 found a distinct region in the right rostral tectum, near the lesion, whose activity is inversely connected to the activity of the left amygdala, whereas the left amygdala is functionally coupled with select areas of the temporal, parietal and occipital lobes. Psychiatric disorders can occasionally be linked to structural changes in the brain. Corpus callosum lesions, in particular, appear to have a role in the change in patients’ behavior. Pavesi G et al. 49 described a case of a rapid psychotic crisis caused by a hemorrhagic cavernous angioma of the corpus callosum, which was surgically excised and the symptoms were completely resolved. Although a developmental abnormality such as agenesis or lipoma is present in the majority of these instances, a developing corpus callosum lesion is only rarely the underlying cause. Clinicians should be aware of this link since it is possible to cure these people.
Barahona-Corrêa JB et al. 50 collected 211 lesional mania cases among 201 individuals with focal lesions, 60.7% had lesions affecting just the right hemisphere, while 11.4% had lesions involving only the left hemisphere. The right-sided predominance of lesions was confirmed across multiple brain regions, including the temporal lobe, fusiform gyrus and thalamus, in additional analyses of 56 eligible lesion images.
Recommendations
The literature indicates various antiepileptic drug (AED) treatment durations. Two years of therapy with AED was found to be similar to 1-year treatment in terms of rate of seizure recurrence. 51 Lesions caused by NCC take a long time to calcify, 52 AEDs are gradually tapered down through incremental doses and eventually broken. 53 Abrupt discontinuation of AEDs is not recommended in patients with multiple cysts as many would develop calcified lesions, which increases the risk of repeated episodes of seizures. 52 Although steroids have been used as an anti-inflammatory to combat perilesional edema and inflammation, rebound edema can commonly occur if steroids are not tapered appropriately. 54 Vesicular cysts are immune-tolerant and do not degrade on their own with time, and increases the frequency of seizures. 55 Therefore, it is recommended to treat with antiparasitic drugs as evidence suggests better outcomes when compared to no treatment or placebos. 56 The treatment regimen for NCC is albendazole (15 mg/kg per day for 2 weeks) and praziquantel (50 mg/kg per day for 2 weeks), which are the two most commonly used antiparasitic drugs, with the former being more effective than the latter. Since both these antiparasitic drugs have different mechanisms of action, combining the two can increase the efficacy of treatment. It has also been observed that treatment with albendazole and praziquantel simultaneously increases the plasma concentration of albendazole by 50%. 56
It is also recommended that antiparasitic treatment is not needed in patients with calcified lesions and NCC encephalitis. 43 Encephalitis is an inflammatory process, and beginning antiparasitic treatment can exacerbate the inflammation. Steroids and osmotic diuretics can be used to prevent ICH. 8 A craniotomy can decompress if medical treatment fails. 57
Conclusion
Diagnosis of NCC psychosis can be challenging despite advances in neuroimaging and immunological diagnostic tests. Clinical manifestations can be non-specific, and neuroimaging findings are mostly not pathognomonic. Immune diagnostic tests lack sensitivity and specificity. A thorough history and a full workup to rule out any organic cause of psychosis are vital to prevent the consequences of undiagnosed and untreated NCC. Early detection and timely treatment are critical because untreated NCC mortality can reach up to >50%. NCC must be placed in the top differential diagnosis in patients in endemic areas with psychiatric symptoms and a history of seizures who poorly respond to standard treatment.
Footnotes
Acknowledgements
The authors would like to thank Drs. Rizwan Ahmed and Zeenat Habibullah for their assistance with the literature search and manuscript preparation.
Author contributions
Dr S.A., Dr S.U., Dr S.J., Dr A.H., Dr Su.S., Dr A.H., S.M.S. and S.S. have been involved in the conception and design of the study, along with acquisition of data. All authors have participated in the drafting of the article and revising it critically for important intellectual content. All authors have provided final approval of the version to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published.