
Abstract
Acetamiprid is a type of neonicotinoid that belongs to the new class of insecticides. It is fatally toxic to insects by acting as an agonist to nicotinic acetylcholine receptors. Cases with neonicotinoids including acetamiprid poisoning in humans were reported around the world. Only one case with acetamiprid poisoning associated with severe adverse effects has been described from Sri Lanka. Serious side effects will occur if it is consumed in excess amount. Here, we described a case of acetamiprid poisoning in a man who developed severe lactic acidosis, myocardial suppression, hyperglycemia, and intestinal obstruction following accidental intake of acetamiprid insecticide. The patient was managed conservatively as there is no specific management mentioned in the literature.
Introduction
Neonicotinoid is a relatively newer type of insecticide currently use in agriculture. 1 Among all suicidal and accidental poisoning, pesticide poisoning is mostly reported in Sri Lanka.2,3 However, the recent incidence of insecticides has also become common due to the restriction of usage of pesticides by the Sri Lankan local government. 4 Acetamiprid is a potent and relatively new neonicotinoid insecticide. It acts as an agonist to nicotinic acetylcholine receptors in insects and causes insect paralysis and death. 5 It has selective toxicity to insects as compared to mammals. A case report describes a buffalo with accidental ingestion of acetamiprid, which presented with severe gastrointestinal symptoms and respiratory distress. 6 Available studies among human victims are few and rather still growing because it has begun to use widely in the last decade.7,8 Serious side effects are rarely reported in acetamiprid poisoning.9,10 A Sri Lankan cohort study of case fatality due to agricultural pesticides poisoning, shows no death related to acetamiprid poisoning during 6 years begins with 2002. 11
Case history
A 27-year-old man was admitted to District General Hospital, Kilinochchi, with a history of accidental intake of neonicotinoid poisoning about 50 mL (commercial name is “MIYAKO ACETAMIPRID, Figure 1). The patient was brought to emergency services from the paddy field after an hour delay. At emergency services, he presented with vomiting, shortness of breath, and dizziness. During an initial assessment, he had patent airway but tachypnea with a rate of 22 per minute. SpO2 was 100% on air. Blood pressure was 110/50 mmHg and pulse rate were 86 beats per minute. Capillary refilling time was less than 2 s. Further examination had shown clear lung fields and a soft abdomen. He was alert and his Glasgow coma scale was 15/15. 12

The leaflet of acetamiprid poisoning brought by patient on admission.
His capillary blood sugar was 228 mg/dL. His arterial blood gas showed severe lactic acidosis (Figure 2). His electrocardiogram showed ST depression, and urgent troponin I was positive (Figure 3). His biochemistry panel showed hypokalemia and mild renal impairment (Table 1). He received supportive management including gastric lavage and activated charcoal. He received IV fluid (normal saline) 120 mL/h, IV soluble insulin 4 units/h, and IV ranitidine 50 mg bd. Hypokalemia was corrected by IV KCl 40 mmol with normal saline.
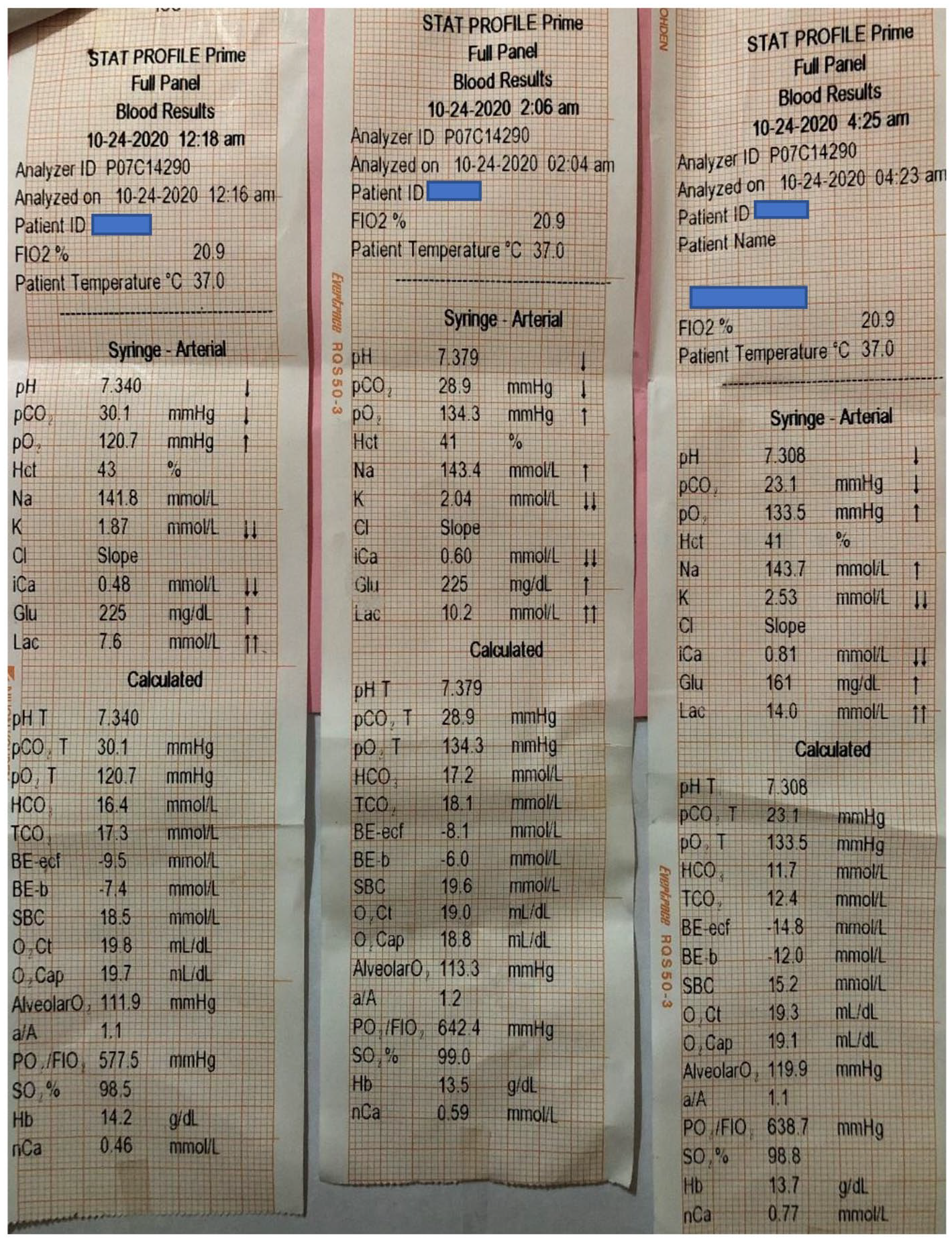
The serial arterial blood gas reports of patient with acetamiprid poisoning.

The 12-lead electrocardiography (ECG) showed wide spread ST depression changes on admission and resolution of ECG changes on discharge in a patient with acetamiprid poisoning.
The biochemical profile of patient is shown with clinical progression of disease.
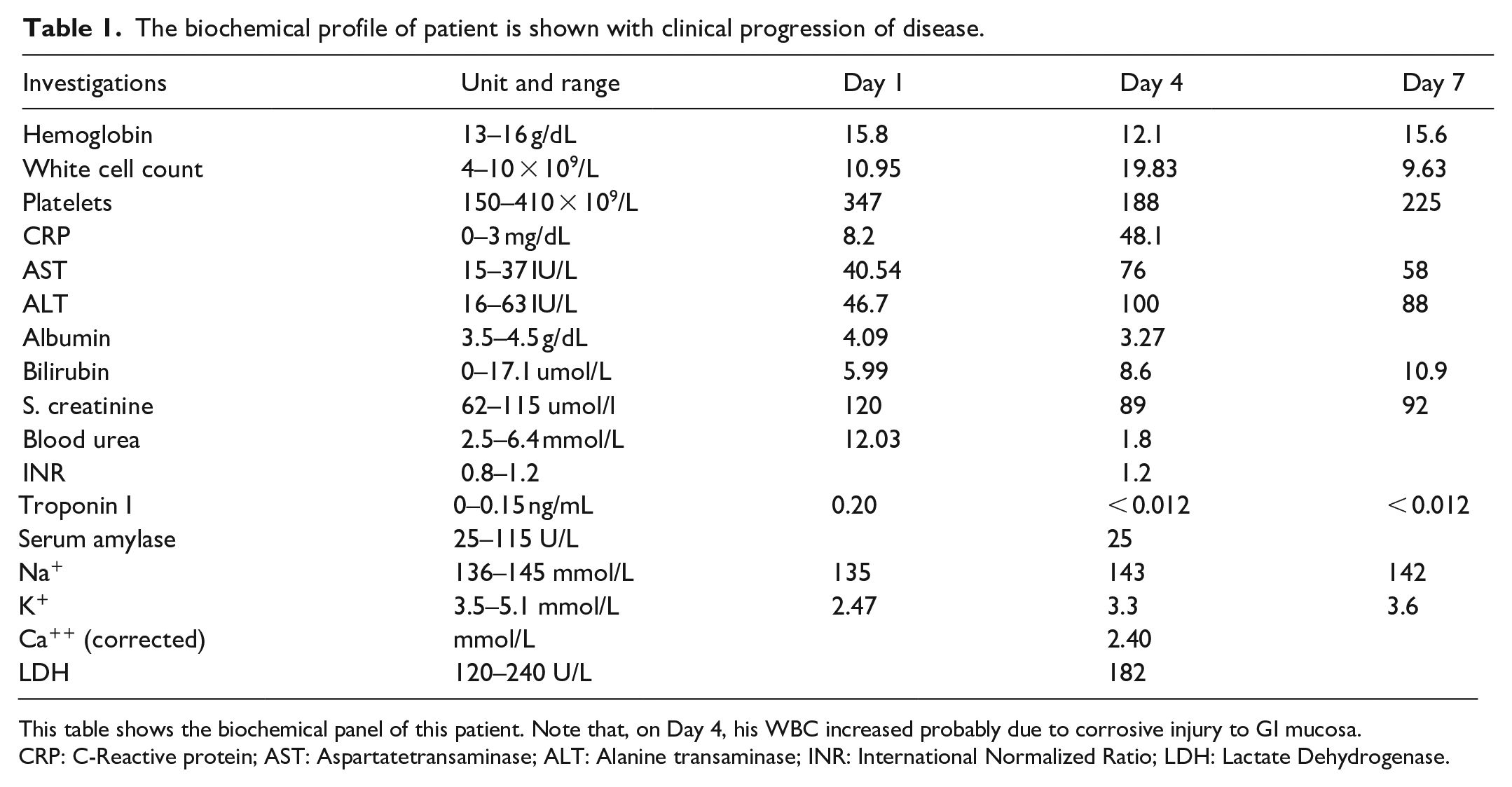
This table shows the biochemical panel of this patient. Note that, on Day 4, his WBC increased probably due to corrosive injury to GI mucosa.
CRP: C-Reactive protein; AST: Aspartatetransaminase; ALT: Alanine transaminase; INR: International Normalized Ratio; LDH: Lactate Dehydrogenase.
The patient immediately was transferred to a tertiary hospital (Teaching Hospital—Jaffna) where he was given NaHCO3 100 mL (4.8%) additionally. Repeat ABG showed improvement of lactate levels. His vitals were stable. His ECG variations have vanished, and his repeat troponin I was negative once his lactic acidosis settled. His 2D ECHO cardiogram showed a normally functioning heart. He was stable at ward stay but later he complained of abdominal cramps, and later he could not make bowel motions. On further examination, he has bowel sounds but had tenderness in the abdomen without rebounding. An esophagus-duodenoscope (OGD) was performed to exclude esophageal erosion or perforation. His abdominal X-ray, chest X-ray, and ultra-sonography could not reveal any evidence of bowel perforation. We did serum amylase level which was within the normal limit. Therefore, we managed conservatively, and he gradually recovered later without any residual complications.
Discussion
Acetamiprid ((E)-N1-[(6-chloro-3-pyridyl) methyl)-N2-cyano-N1-methylacetamidine, CAS 135410-20-7] is a newer member of neonicotinoid class insecticide. Other members of the neonicotinoid class include clothianidin, thiacloprid, dinotefuran, nitenpyram, imidacloprid, and thiamethoxam. 13 All neonicotinoids are structurally similar to nicotine. 14 The binding behavior of neonicotinoids on the insect nicotinic acetylcholine receptor is similar to those of nicotine and nicotinoids in humans. 15 Nicotine and other nicotinoids are both agonists of the nicotinic acetylcholine receptor. 16 The receptors are found in greater numbers in insects than mammals but are expressed primarily in the insects’ central nervous system. 16
Neonicotinoids are high-affinity agonists of insect nicotinic acetylcholine receptors (nAChRs) resulting in paralysis and death in insects. 16 Because neonicotinoids do not have a high affinity for mammalian and other non-insect nAChRs, they are thought to have limited toxicity in non-target organisms, including humans. 17 In 2013, the European Union (EU) identified two neonicotinoids, acetamiprid, and imidacloprid, as potential neurodevelopmental toxins. 18
In this case, this patient took about 50 mL in 250 mL of water from a strength of 20% (200 g/L) acetamiprid, which immediately caused several metabolic and target organ complications. The most serious complication that he had developed was lactic acidosis. He also had mild liver enzyme impairment but not went to hepatic failure. Hepatotoxicity from a neonicotinoid exposure is typically apparent only at high doses and is frequently accompanied by a decrease in food consumption and a reduced body weight. Serum activities of alanine aminotransferase, alkaline phosphatase, and aspartate aminotransferase, markers of hepatotoxicity, are typically elevated in rats exposed to imidacloprid. 19 He also had electrocardiogram changes at the initial state of admission. He did not complain of chest pain or palpitation or we did not notice any hypotensive episodes. Although his initial serum troponin I was positive, subsequent serum test for negative to troponin and no imaging evidence of hypokinesia of myocardial wall in 2D echocardiogram. This was probably due to the improvement of metabolic abnormalities. A Japanese case report suggests that the consequences of the abnormal electrocardiogram changes may be due to the active ingredient acetamiprid. 20
The main muscarinic signs of acute OP poisoning are miosis, mucous super secretion, excessive sweating, bradycardia, epiphora, and diarrhea. They were not observed in this patient. However, a Chinese case report describes severe multiorgan dysfunction including cerebral ischemia and features of organophosphate poisoning required atropine. 9 He also developed epigastric pain with abdominal cramping pain during his hospital stay with elevated white blood cell (WBC) and C-reactive protein (CRP) levels. We have done ultra-sonography of the abdomen and X-ray abdomen to look for perforation and intestinal obstruction, and we performed oesophagio-duodenoscopy to exclude oesphagial perforation and erosions. This could be due to possible toxicity in gastro-hepatic-entero system.
We did not perform gastric lavage and administration of activated charcoal as he presented to the hospital about 3 h after the ingestion. We think that it could not be very effective because he developed severe acidosis at the time of admission. At the time of admission, his blood pressure and pulse rate were within range, but his initial serum urea and lactate levels were elevated. We could not eliminate the possibility of transient hypotension, which led to lactic acidosis before the hospital admission. There is no specific management elsewhere mentioned in previous case reports. 21
Conclusion
In this case report, we describe a case of acetamiprid poisoning, which caused severe lactic acidosis along with acute liver injury and acute myocardial injury. The presence of lactic acid rises the possibility of an unnoticed hypotensive episode, or otherwise, it could be due to direct toxic injury to cells. This observation needs further research. An elevated level of troponin could be explained by the direct toxin effect. There is no specific management mentioned in the literature. Sri Lanka had enough evidence of the adverse effects of pesticides over time. Proper awareness and health education must be conducted repeatedly among farmers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual case reports
Informed written consent
The informed written consent was obtained from patient to publish this case report.