
Abstract
Endoscopic cyclophotocoagulation is a relatively safe cyclodestructive procedure with a lower complication rate compared to trans-scleral cyclophotocoagulation. Serous choroidal detachment is a complication that has been reported following endoscopic cyclophotocoagulation; however, it is usually mild and transient. A case of bullous choroidal detachment with a flat anterior chamber requiring drainage after endoscopic cyclophotocoagulation is presented, along with a discussion on the risk factors precipitating such complication.
Introduction
Endoscopic cyclophotocoagulation (ECP) is a glaucoma laser intervention that was introduced in 1992, with the concept of targeting the ciliary body through an endoscopic approach. 1 The technique utilizes diode laser ablation of the ciliary processes leading to a cessation of blood flow and subsequent coagulative necrosis. This, in turn, leads to a reduction in the amount of aqueous inflow inside the eye. ECP has been performed in both adult and pediatric glaucoma, alone or in combination with routine cataract surgery. 2
ECP is considered a relatively safe procedure, especially when comparing it with trans-scleral cyclophotocoagulation (CPC). 3 Common complications reported following ECP are intraocular pressure (IOP) spikes, postoperative inflammation, and hemorrhage. 4 Moreover, it is not uncommon to encounter choroidal detachment after ECP as it can occur due to reduced IOP postoperatively. The incidence of choroidal detachment following ECP in studies that have reported such a complication ranged from 1% to 5%.5–8 Nonetheless, choroidal detachment is usually mild and transient.
We hereby report a case of bullous choroidal detachment requiring drainage that occurred following phacoemulsification combined with ECP (Phaco-ECP), along with a short review of the pertaining literature.
Case report
This is a 75-year-old male with pseudoexfoliative glaucoma scheduled to undergo Phaco-ECP. His past surgical history includes trabeculectomy OD 5 years prior and bleb revision via needling 6 months after initial surgery. The patient was on three topical glaucoma medications in both eyes.
Visual acuity OD was 20/160 and the IOP was 21 mmHg. On slit lamp examination, he had an open angle, a + 2 nuclear sclerotic cataract, 0.8 cup-disk ratio, and his fundus exam was unremarkable. In view of his visually significant cataract, borderline IOP, failed trabeculectomy, and advanced cupping on three topical glaucoma medications the patient was booked for Phaco-ECP OD. Cataract extraction was combined with ECP to reduce the number of glaucoma medications that the patient was using.
The patient underwent uneventful phacoemulsification followed by ECP using the E2 Laser and Endoscopy System with a straight probe (Endo Optiks, Little Silver, NJ, United States) over 200 degrees of ciliary processes. Laser was applied with a power of 0.5 W on a continuous mode for 2 s until whitening and shrinkage of the ciliary process was observed. Postoperatively, the patient was put on topical ofloxacin 0.3% (four times daily), topical prednisolone acetate 1% (every 2 h while awake tapering), and his glaucoma medications were reduced to two drops (a beta blocker and a carbonic anhydrase inhibitor); the prostaglandin analogue was stopped. In his first postoperative visit (day 1), visual acuity was 20/100, IOP was 20 mmHg, the anterior chamber was deep, and the retina was flat without any choroidal effusion.
Two weeks postoperatively, the patient presented to the emergency department with a complaint of worsening in vision. His acuity was 20/400, IOP was 15 mmHg, the bleb was flat, the anterior chamber was shallow, and his fundus exam showed a 360 degree choroidal detachment (Figure 1(a)) that was further confirmed by ultrasonography (Figure 1(b)). The patient was placed on topical prednisolone acetate 1% (every hour while awake) along with topical atropine sulfate 1% (three times daily). Three days later, IOP was 8 mmHg, the anterior chamber was flat (Figure 2), and the choroidal detachment was unchanged. In view of the bullous detachment and flat anterior chamber, the plan was to proceed with choroidal drainage and anterior chamber reformation.
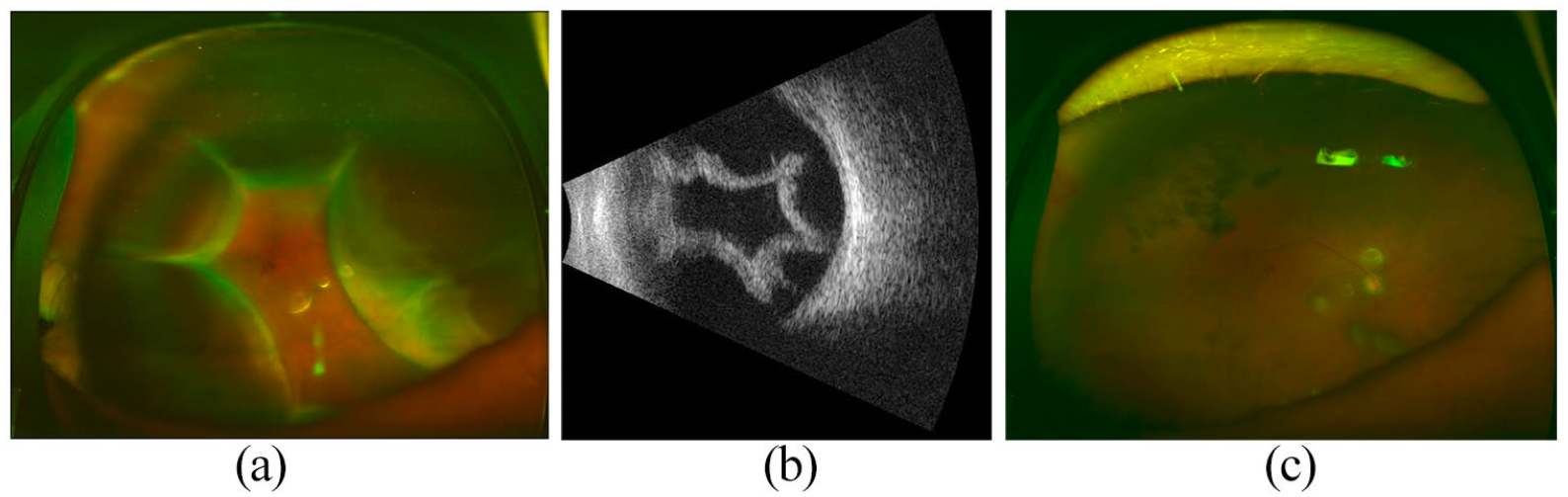
(a) Color fundus photo of the right eye showing bullous choroidal detachment obscuring the view to the optic nerve head. (b) Ultrasonography of the right eye showing 360 degree choroidal detachment occupying two-thirds of the globe. (c) Postoperative color fundus photo of the right eye showing resolution of the choroidal effusion.

Slit lamp photo of the right eye showing a flat anterior chamber (arrow). The choroidal detachment can be seen behind the pupil (asterisk).
After a limited temporal conjunctival periotomy and placement of two infero-temporal scleral incisions, fluid was drained from the suprachoroidal space using a 26-gauge cannula and the scleral incisions were left without suturing to prevent recurrence of choroidal effusion. This was followed by reformation of the anterior chamber using balanced salt solution. Intraoperative fundus examination confirmed the resolution of choroidal effusion. First-day post-operatively, IOP was 16 mmHg, the anterior chamber was deep, and fundus examination confirmed the presence of a flat retina without choroidal effusion (Figure 1(c)).
Six months following drainage, the patient regained a visual acuity of 20/30 and IOP was 16 mmHg on two topical glaucoma medications. The timeline of events is illustrated in (Figure 3).

Timeline illustrating the sequence of events in the reported case.
Discussion
Multiple mechanisms have been proposed to explain the occurrence of choroidal detachment following glaucoma surgery. It is postulated that postoperative hypotony enhances aqueous outflow from the anterior chamber into the suprachoroidal space. 9 Although experimental data suggest that hypotony is a prerequisite for choroidal detachment, clinical studies have shown that a detachment can occur despite a normal IOP level, 10 as seen in our case. Another mechanism of effusion is postoperative inflammation promoting the transudation of fluid into the suprachoroidal space. 11
It is important to identify risk factors that may lead to choroidal detachment in any given patient undergoing glaucoma surgery. Factors of particular note in our case include old age, prior history of glaucoma filtering surgery, and the use of topical glaucoma medications postoperatively. In the present case, the detachment was discovered 14 days after ECP which is considered a relatively late presentation. Haga et al. 10 reviewed 79 cases of choroidal detachment following glaucoma surgery and the mean period between surgery and the appearance of detachment was 6 days.
Our review of the literature on the complications of ECP showed that out of 29 papers published on 2133 eyes, 25 studies did not report a single case of choroidal detachment. On the contrary, 4 articles described choroidal detachment following ECP at a rate of 1%–5% (Table 1).5–8 In spite of that, none of these patients were reported to require choroidal drainage, as indicated in our case.

ECP: endoscopic cyclophotocoagulation.
In conclusion, ECP is a minimally invasive procedure that has a lower complication rate compared to traditional CPC. Choroidal detachment is a complication that may occur following ECP, however, it is usually mild, transient, and resolves without the need for surgical intervention. Our case has demonstrated that in the presence of multiple risk factors (i.e. old age, prior history of glaucoma surgery, and usage of glaucoma medications), the detachment can be bullous requiring choroidal drainage.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Institutional Review Board at King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia (1841-CR)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.