
Abstract
Xanthomas are plaques or nodules consisting of an accumulation of excess lipids, resulting in the formation of foam cells in the skin or tendons. Typically, xanthomas are not accompanied by other symptoms. Here, we report a patient with a presentation of painful palmar xanthomas and subsequent diagnosis of metabolic and cardiovascular morbidities. A 44-year-old man presented with multiple yellowish, firm, and painful nodules on his right palm and fingers. Lipid panel and medical examination revealed a diagnosis of type III hyperlipoproteinemia and diabetes mellitus type II. Histopathological examination of the lesions revealed numerous lipid-laden foamy cells surrounding the nerve bundles through the dermis. This unique presentation of painful xanthomas prior to the manifestation of more significant underlying conditions suggested that xanthomas might be used as early diagnostic indicators. Based on this case, we propose more thorough examinations of palmar xanthomas in patients for earlier detection of potentially lethal diseases.
Introduction
Xanthomas are plaques or nodules consisting of an accumulation of lipids, resulting in the formation of foam cells in the skin or tendons. The appearance of xanthomas is usually a sign of various underlying lipoprotein disorders. Xanthomas may arise due to primary dyslipidemias or systemic disorders, such as hepatic, hematologic, and endocrine diseases, resulting in secondary dyslipidemia. Typically, xanthomas are not accompanied by other symptoms. Here, we report a patient with painful palmar xanthomas. We hypothesize that the pain may be induced by the compression of nerve bundles in the palm by the xanthoma cells.
Case report
A 44-year-old man presented with multiple yellowish firm nodules on his right palm and fingers (Figure 1(a)–(c)). The nodules appeared 2 months prior and induced pain whenever he performed a grasping motion with his hands. The number and size of the lesions gradually increased. Upon physical examination, similar lesions were not found elsewhere on the body, including achilles tendon, cornea, knees, and buttocks. His medical history was unremarkable, except for his recent diagnosis of diabetes mellitus type II and arterial hypertension. A lipid panel examination revealed hypertriglyceridemia (1465 mg/dL; reference range = 0–149 mg/dL) and hypercholesterolemia (420 mg/dL; reference range = 125–200 mg/dL). At an additional history taking, he had no family history of hyperlipidaemia. Lipoprotein electrophoresis finding yielded a broad beta band and suggested type III hyperlipoproteinemia. Histopathological examination of the lesions revealed numerous lipid-laden foamy cells surrounding the nerve bundles through the dermis (Figure 2(a)–(c)). Collectively, our investigations resulted in a final diagnosis of painful planar xanthoma in palmar area with dyslipidemia. The patient was referred to a physician for further investigations such as cardiovascular evaluation, and he started the hypolipidemic treatment. The patient is currently under the follow-up of his physician.

Multiple yellowish firm nodules on the fingers and palm, marked above as (a), (b), and (c).
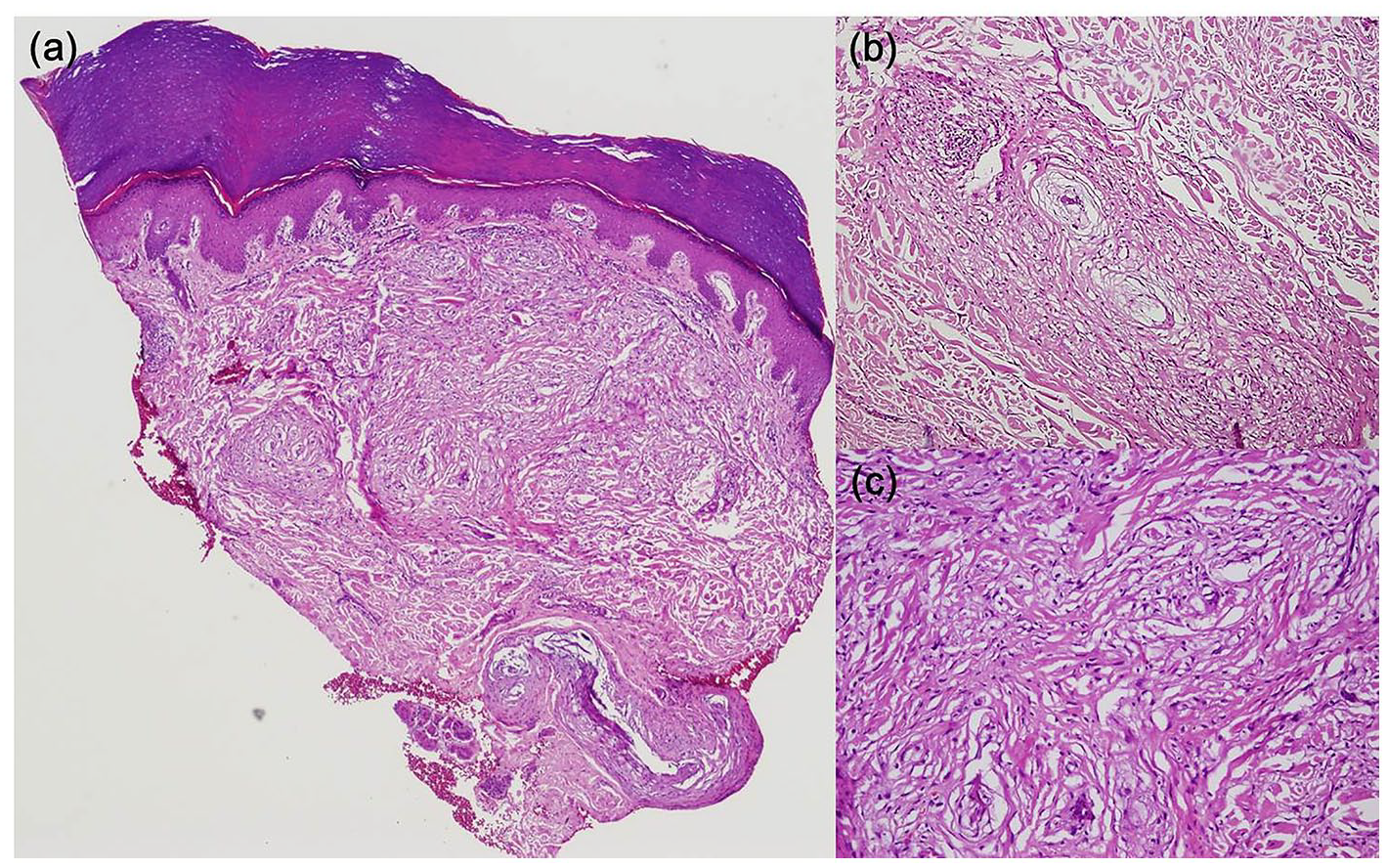
(a) There are nerve bundles and numerous lipid-laden foamy cells in the interstitium through the dermis (H&E, ×40). (b) and (c) Nerve bundles are surrounded by foamy macrophages in the dermis (H&E, ×100 and ×200).
Discussion
Xanthomas develop predominantly due to increased local extravasation of lipids from the vessels into the surrounding tissue. 1 Monocytes and macrophages in tissues phagocytize these lipid particles either through specific receptors or through phagocytosis of low-density lipoprotein (LDL) aggregates and lipid complexes with antibodies, enabling the formation of foam cells. 1 Seven distinct types of xanthomas have been described thus far, tendon xanthoma, xanthelasma palpebrarum, eruptive xanthoma, tuberous xanthoma, planar xanthoma, xanthoma disseminatum, and verruciform xanthoma. 2 Among them, planar xanthomas mostly present as macular lesions with elevations occurring rarely and found commonly on the upper eyelids near the inner canthus, the wrists and palms, and in intertriginous areas. The planar xanthomas include planar xanthomas of cholestasis, intertriginous xanthomas, palmar crease xanthomas, and diffuse plane xanthoma. Planar xanthomas in the palm are commonly referred as palmar crease xanthomas, presenting yellow–orange macules involving the palm creases and typically diagnostic for type III hyperlipoproteinemia. Unlike palmar crease xanthomas, planar xanthomas of cholestasis are well-demarcated plaques that extend beyond the palmar creases. 3 The patient in our case was diagnosed with planar xanthomas of cholestasis in that he developed well-demarcated, beige–orange plaques on his hand, had diabetes mellitus, and showed high-density lipoprotein (HDL) deficiency.
In general, xanthomatous lesions have no associated symptoms such as pain or pruritus. However, our patient with xanthomatous lesions was symptomatic. Based on histological evidence, we attributed the pain to the compression of nerve bundles by the xanthoma cells. There have been a few reported cases of xanthoma of the palm with pain,4–6 but there has not been any prominent case that has demonstrated that foam cells invade the nerve bundles. Interestingly, planar xanthomas have been known to be pathognomonic in type III hyperlipoproteinemia and are found in patients with newly diagnosed diabetes mellitus, primary biliary cirrhosis, and premature atherosclerosis. 7 Consistent with this, our patient was subsequently diagnosed with severe metabolic and cardiovascular morbidities following the presentation of palmar xanthomas. This suggests that palmar xanthomas may be early manifestations of pernicious underlying metabolic conditions. 8
A genetic basis for type III hyperlipoproteinemia is well established. Mutations in the apolipoprotein E cause broad beta diseases due to a binding defect to beta-very low-density lipoprotein (VLDL). 2 Most patients are homozygous for the apolipoprotein E2 variant. 7 Therefore, apolipoprotein E genotyping may be required to elucidate the genetic predisposition in patients who presenting xanthomas. In addition, since planar xanthoma may be related to monoclonal gammopathy or diffuse large B cell lymphoma, various systemic evaluations are required (Table 1).
Systemic evaluations of xanthomas.
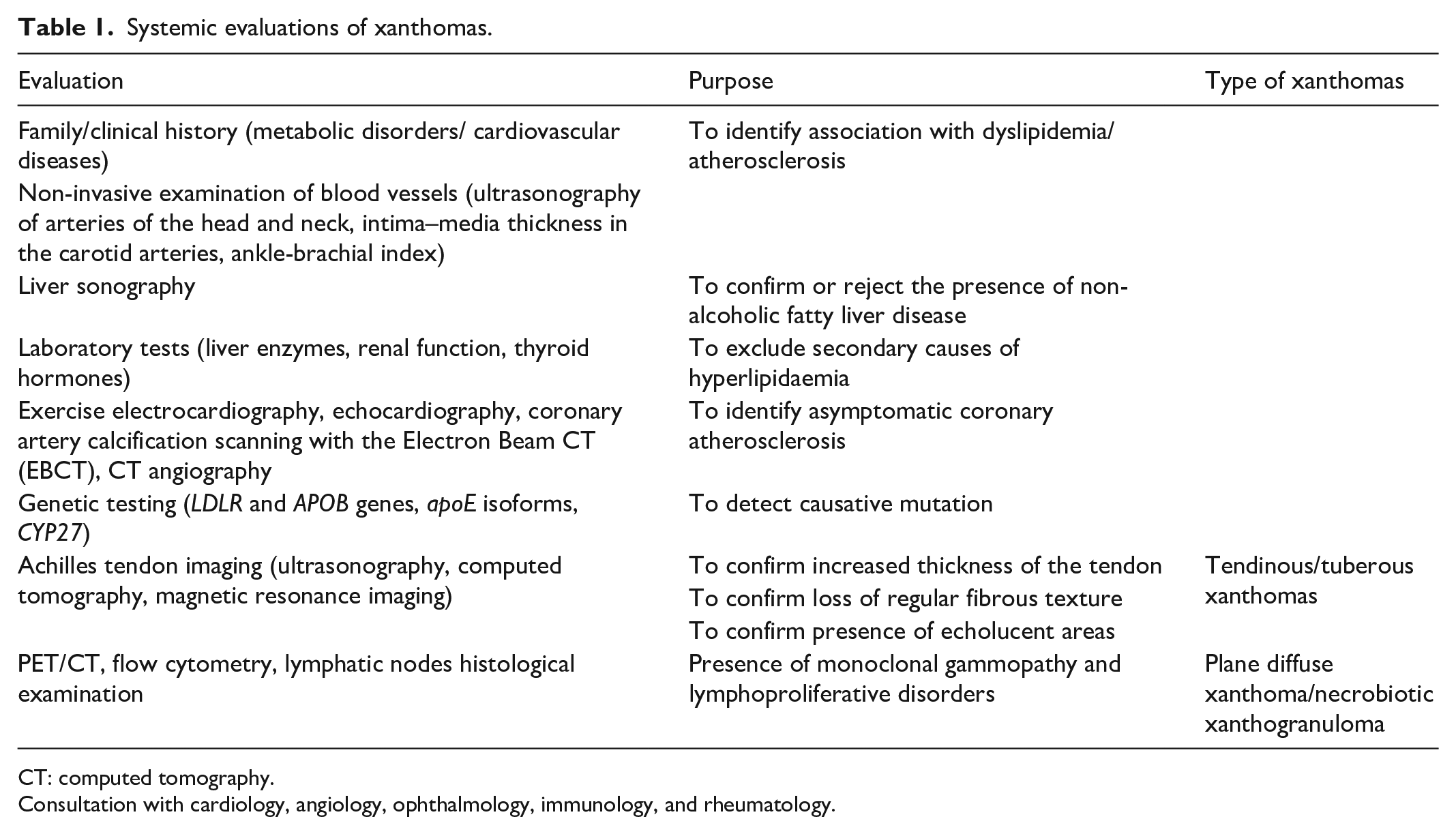
CT: computed tomography.
Consultation with cardiology, angiology, ophthalmology, immunology, and rheumatology.
Failure to diagnose and initiate treatment for hyperlipoproteinemia could potentially lead to serious cardiac morbidity. Earlier diagnoses of these diseases can result in increased life expectancy due to proper medical intervention in the form of antihyperlipidemic drugs and dietary modifications. We propose more thorough examinations of palmar xanthomas in patients to enable earlier detection of potentially fatal diseases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient prior to publication.