
Abstract
Mycobacterium elephantis was first described when isolated from an elephant that succumbed to lung abscess. However, despite this namesake, it is not associated with animals and has been described most often as a probable colonizer rather than pathogen in humans with chronic lung disease. In this report, we describe the first case of lymphocutaneous infection from M. elephantis, likely as a result of cutaneous inoculation with contaminated soil. This offers further evidence to its capabilities as a pathogen. We provide a review of the limited prior reports of M. elephantis and outline the available in vitro data on efficacy of various antimycobacterial agents.
Keywords
Introduction
Lymphocutaneous spread of infection may be caused by a broad variety of bacterial and fungal organisms, with nontuberculous mycobacteria (NTM) species representing particularly characteristic pathogens. While Mycobacterium marinum is classically described as causing this syndrome, it may caused by a variety of atypical mycobacterial species and in particular, rapid-growing mycobacteria (RGM).
Mycobacterium elephantis is infrequently described in the literature and when referenced is often suspected as a colonizer of respiratory secretions in patients with pre-existing pulmonary disease. Its pathogenicity is debated, and it has never previously been described as a cutaneous pathogen. Here, we provide the first description of lymphocutaneous spread of M. elephantis and highlight the available data on pharmacological management. Similar to other atypical mycobacteria, it is likely best managed with a combination of antimycobacterial agents. Consent was provided from the patient to publish this report.
Case report
A 66-year-old immunocompetent female was seen in the dermatology clinic for ulcerations of her right hand, ascending her arm in a lymphocutaneous distribution. She denied trauma preceding the lesions. There was no exposure to animals aside from a domesticated dog and cat. Her only travel was to Arizona 6 months before. She had exposure to floodwater in her home 5 months before. She was an avid gardener, working with soil on a daily basis. One month prior to symptom onset, she had received a potted plant (Haworthia fasciata) imported from the Eastern Cape in South Africa.
Clinically, she had punched-out ulcerations with yellow-white crust and minimal surrounding erythema (Figure 1). Histology of skin biopsy demonstrated a dense papillary dermal lymphohistiocytic infiltrate without well-formed granulomata. Gram, Fite, and Ziehl-Neelsen staining were negative. Aerobic culture was positive for Candida parapsilosis. She was treated with cephalexin and fluconazole without response. Mycobacterial culture was positive on BACTEC MGIT for M. elephantis at 23 days of incubation (acid-fast bacilli smear negative). Drug susceptibility testing results using microbroth dilution are outlined in Table 1. Additional scattered lesions on her legs were negative for acid-fast bacilli smear and mycobacterial culture. She was initiated on azithromycin and moxifloxacin with improvement after 3 months of treatment.

Lymphocutaneous infection from Mycobacterium elephantis (a) prior to treatment initiation and (b) 3 months into treatment with combination of azithromycin and moxifloxacin.
Reported clinical isolation and drug susceptibility of Mycobacterium elephantis infection.
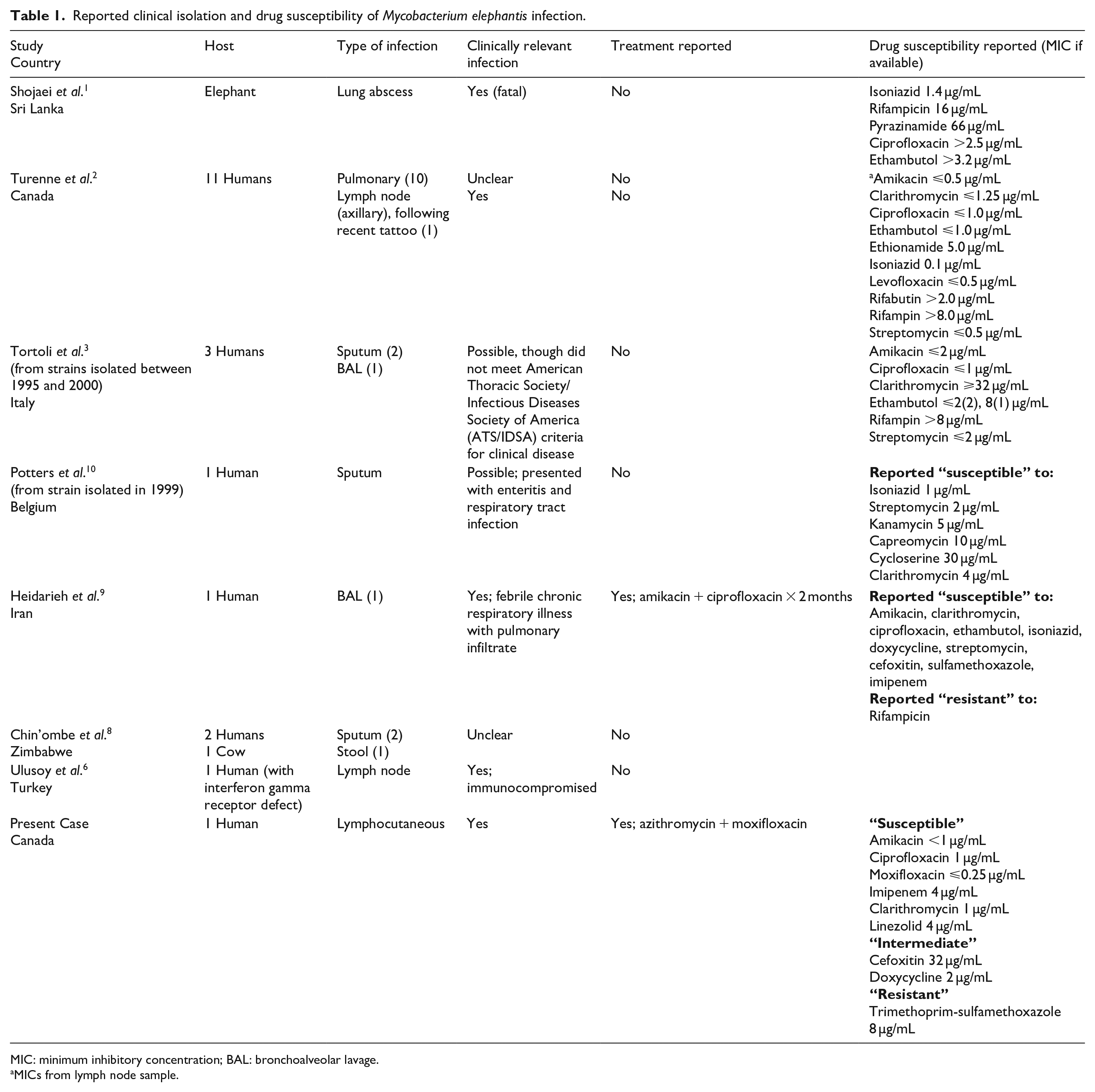
MIC: minimum inhibitory concentration; BAL: bronchoalveolar lavage.
MICs from lymph node sample.
Discussion
M. elephantis was first described 20 years ago in an elephant that succumbed to chronic lung abscess. 1 The species is phenotypically similar to Mycobacterium flavescens though genotypically more closely related to Mycobacterium pulveris.1,2 M. elephantis is recognized as a rapid- or intermediate-growing Mycobacterium (growth detected at less than 7 days (rapid) or 10 days (intermediate)), although it appears to grow at a slower rate than other rapid-growers (RGM).2,3 RGM are frequently associated with cutaneous disease, 4 but this is the first described case of M. elephantis infection in the skin.
Similar to other environmental mycobacteria, the pathogenicity of M. elephantis is debated. In the largest report, M. elephantis was described in 11 patients in Ontario, Canada (10 sputum, 1 lymph node excision). 2 Most were elderly patients with prior mycobacterial disease, and all sputum samples were smear negative with single-positive cultures, questioning the clinical significance. 2 Due to its relative scarcity of description, M. elephantis has not been described in international guidelines for diagnosis and management of mycobacteria.4,5 Nonetheless, invasive disease has been confirmed in animals 1 and in humans.2,6
Contact with animals is not a recognized risk factor. M. elephantis has environmental reservoirs including natural and man-made water sources and soil.7,8 Only one patient report described immunocompromise. 6 Similarly, our case had no recognized predisposing factors but suggests that M. elephantis may extort breaks in cutaneous defenses. It is unknown if M. elephantis occupies a particular ecological niche to localize where infection was acquired. The most likely mechanism of acquisition was cryptogenic penetrating trauma to her extremity, contaminated by soil colonized with M. elephantis. Exposure to the plant/soil imported from South Africa is an interesting theory but could not be proven.
Lymphocutaneous spread of infection ascends the lymphatic pathway with intermittent subcutaneous nodules and ulcerations and is often termed a sporotrichoid pattern, named after Sporothrix schenckii. The infectious differential diagnosis includes M. marinum and RGM such as Mycobacterium chelonae and Mycobacterium fortuitum, but M. elephantis has not been reported.
Susceptibilities of M. elephantis are not established. Similar to other RGM, minimum inhibitory concentrations (MICs) to antituberculosis medications are usually elevated2,3,9,10 (Table 1). MICs to macrolides and fluoroquinolones are typically low.2,3,9 Due to the recognized potential of Mycobacterium to develop mutational macrolide resistance, we suggest a prudent approach is to utilize at least a two-drug therapy for several weeks beyond resolution of the lesions.
Herein, we report the first case of M. elephantis presenting as a cutaneous pathogen in a lymphocutaneous pattern. Although the pathogenicity of this organism in pulmonary samples is debated, our case adds further support to its potential pathogenicity in immunocompetent human hosts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed patient consent was provided for the publication of this report.