
Abstract
Spleen tumors are an uncommon disease. Littoral cell angioma belongs to the group of vascular tumors. It is believed that this tumor originates from the tissue of the red pulp sinuses, specifically from the cells that are lining the sinuses. If this rare tumor is diagnosed, it is necessary to search for synchronous or metachronous visceral neoplasia. Littoral cell angioma can also mimic metastatic lesion of the spleen. This case report wants to draw attention on this rare tumor of the spleen which is very often associated with other visceral malignancy.
Introduction
Spleen tumors are an uncommon disease. Most often we find a tumorous involvement of splenic parenchyma as part of dissemination of hematological malignancies or secondary metastatic disease. Primary tumors originating directly from the spleen tissues are very rare. In general, these neoplasms can be divided into two basic groups. Tumors originating from splenic lymphatic tissue divided into non-Hodgkin’s and Hodgkin’s lymphomas, although primary lymphoma involvement of the spleen is very rare in itself and accounts for only about 1% of all cases. 1 The second group includes neoplasms originating from non-lymphatic tissue of the spleen. These include, in particular, tumors originating from vascular tissue and tumors from tissues of mesenchymal origin. Tumors in both groups can be of a benign or strongly malignant nature. 2 Secondary involvement of the spleen may also occur, in particular hematogenous dissemination of malignant tumors of various, even relatively distant localizations.
Littoral cell angioma (LCA) belongs to the group of vascular tumors. It is believed that this tumor originates from the tissue of the red pulp sinuses, specifically from the cells that are lining the sinuses. These “littoral cells” combine an endothelial and histiocytic immunophenotype allowing for their immunohistochemical identification. Although these are almost always benign tumors, malignant variants have also been described. 3 The clinically significant feature of these tumors is their very common coincidence with other visceral tumors, in up to 60% of cases. 4
To date, about 150 cases of this cancer have been known worldwide. The first population of these tumors was published in 1991 by Falk. 5 The second and larger group of 25 cases was published by Czech authors in 2016. 6
Clinically, LCA is usually a random finding in an asymptomatic individual. Possible symptoms may include non-specific abdominal pain or certain abdominal discomfort along with elevated body temperature of unclear origin. Other symptoms may result from hypersplenism, which may lead to anemia, thrombocytopenia, or pancytopenia. Splenomegaly can be diagnosed by physical examination, but that is not necessarily the rule. Usually, the next step in the diagnostic algorithm is an ultrasound scan of the abdomen that can confirm splenomegaly. LCA does not have a specific ultrasound picture, so it cannot be clearly distinguished from other focal spleen processes, especially lymphoma or metastatic involvement. Also, computed tomography (CT) scan cannot be used to identify LCA reliably. 7
The causal treatment of LCA is, of course, surgery in the form of splenectomy with subsequent histological examination, which is the only method providing reliable identification of this type of cancer. If this is confirmed, it is necessary to search for synchronous visceral neoplasia.
In the following case report, we would like to present the LCA case managed at the Department of Surgery, University Hospital Plzeň.
Case report
A 53-year-old female with a congenital developmental defect of the upper limbs was admitted to the Department of Gynecology and Obstetrics, University Hospital in Pilsen in May 2009 for normocytic anemia and an unclear mass in the left ovary, with a suspected malignancy. The diagnosis was made by transvaginal ultrasound. Surgery was indicated after the necessary preparation to manage this finding. The gynecological team performed a laparotomy and found a tumor originating from the sigmoid area. The Surgical Department team was called in and managed the finding by radical sigmoid resection and end-to-end intestinal anastomosis. The postoperative course was uncomplicated. Histology revealed a well-differentiated, tubular adenocarcinoma of the sigmoid, pT3N0M0. Adjuvant chemotherapy was subsequently indicated in the patient. As part of staging to exclude distant metastases, the patient underwent an ultrasound scan of the abdomen, with unclear findings in the spleen area, and multiple metastatic involvement was suspected. A similar picture was seen in a CT scan with a contrast agent. A hematological malignancy was also considered in the differential diagnosis. The oncologist discontinued chemotherapy until a full explanation of the findings, and the patient was referred to the care of a hematologist. However, bone marrow biopsy did not confirm any signs of hematologic malignancy. Splenectomy was considered in the patient but, on the follow-up ultrasound scan, including the administration of a ultrasound (USG) contrast agent, the finding appeared to be multiple hemangiomas. Magnetic resonance imaging (MRI) was also recommended for definitive verification of the finding. In the MR image, however, the finding did not appear to be typical for metastatic disease, and further monitoring by USG was recommended by the radiologist. Follow-up colonoscopy revealed a normal finding. As part of cancer follow-up, a positron emission tomography in combination with computed tomography (PET/CT) scanning was performed in February 2011, but without a contrast agent for poor peripheral venous circulation due to a developmental defect of the upper limbs. In the PET/CT scan, the spleen appeared to be normal, without accumulation of fluorodeoxyglucose (FDG). Thus, the patient was followed repeatedly until 2016, always without the administration of a contrast medium due to insufficient venous circulation in the upper limbs. Repeated ultrasound of the abdomen was not indicated. Anemia was repeatedly detected in the patient since the first abdominal surgery, which was initially attributed to the sigmoid tumor. Due to its recurrence after resection of the tumor, the patient was subsequently referred again to the care of hematologists. Repeated decreases in blood count were also attributed to hypermenorrhea, but repeated gynecological examinations revealed physiological findings, including biopsy of the endometrium. Gradually, the patient developed fluctuating thrombocytopenia. The hematologist indicated the appropriate pharmacological treatment, but without greater effects. The latest PET/CT scan in September 2016 revealed progression of splenomegaly (Figures 1 and 2). Due to unclear repeated anemia and decreased platelet count, a splenectomy was subsequently indicated by the hematologist. This was performed without complications in February 2017. The removed spleen was voluminous (22 × 15 × 10 cm), with a native weight of 1.5 kg. The histological examination demonstrated the presence of LCA (Figure 3). The postoperative course was without complications, and the patient was released on the sixth postoperative day and referred to the care of her hematologist. After the splenectomy, only secondary leukocytosis was present in the blood count, the platelet count normalized, and the patient was no longer anemic. The sigmoid cancer disease is in full remission from 2009, according to the last examination.

Splenomegaly on PET/CT, frontal plane.

Splenomegaly on CT, transverse plane.
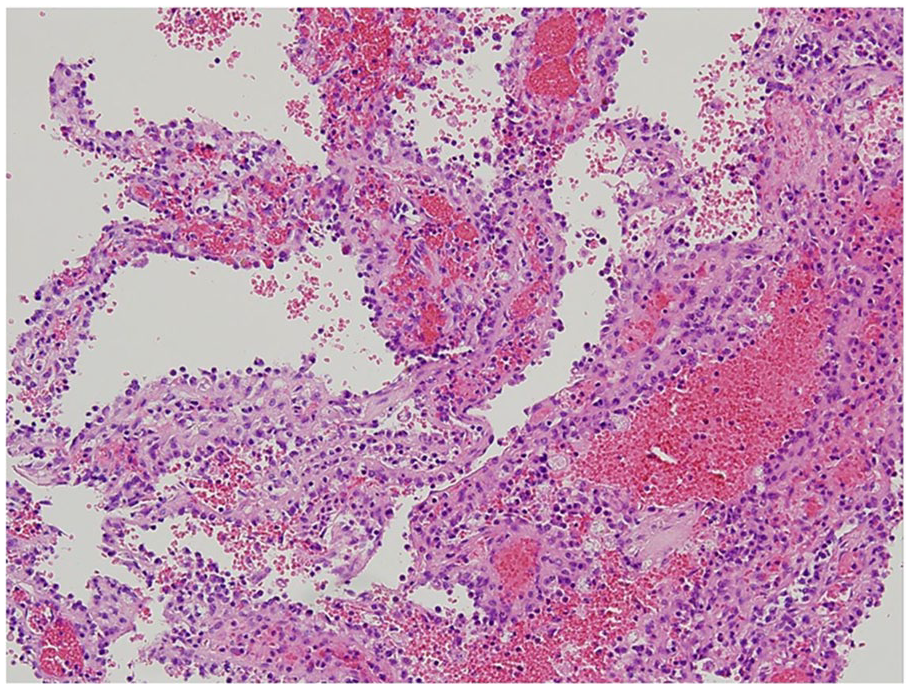
Histologic section shows vascular channels lined by littoral cells, 200 × magnification.
Discussion
Primary malignancies of the spleen are rare and include aggressive forms of lymphomas, hemangiosarcomas, lymphangiosarcomas, fibrosarcomas, or leiomyosarcomas. 1 More frequently, the splenic parenchyma is affected as part of the metastatic spread of another tumor disease. Hematogenous metastases are observed in breast carcinoma, bronchogenic carcinoma, malignant melanoma, gastric carcinoma, pancreatic carcinoma, and colorectal carcinoma. 8 The latter tumors, along with malignant kidney and adrenal gland tumors, can grow directly into the spleen. LCA is classified in the group of rare primary spleen tumors. From the clinical point of view, frequent coincidence with other visceral tumors is important in this cancer. In the largest published group of 25 LCA patients, tumor duplicity was present in 15 cases, most often represented by colorectal and renal carcinoma. 6 The symptoms of this tumor disease are not specific. These may include pressure pain in the left subcostal region, mesogastrium, and splenomegaly which can be detected during clinical examination. The blood count may be completely physiological, but anemia, thrombopenia, or even a picture of pancytopenia is often present with hypersplenism. Ultrasound is the first-line imaging technique, preferably supplemented with a contrast agent. If diagnostic uncertainty persists, the next method of choice is computerized tomography or magnetic resonance imaging, again with a contrast agent. However, as can be seen from the presented case report, not all of these examinations are able to reliably distinguish LCA from simple hemangioma of the splenic parenchyma. In contrast enhanced CT pictures, a well circumscribed, hypodense lesions can be found. In unenhanced T2-weighted images, the LCA shows a high-signal intensity, as in T1-weighted images of the LCA is hypointense in signal. 7 Although this is, in fact, a benign tumor, its surgical removal is always indicated. Primarily, progressive splenomegaly may even rupture over time, and poorly correctable pancytopenia may occur, placing the patient at risk of bleeding complications. In rare cases, LCA can become malignant. 9 A definitive diagnosis is determined by histopathological examination of the sample; use of immunohistochemistry markers such as CD31, CD34, and CD68 is recommended to confirm the diagnosis. Multinodular growth, replacing normal splenic parenchyma, is a typical histopatological finding. There can be anastomosing vascular channels, divided by stromal septa. 6 In our case report, the sequence of events was the opposite, a malignancy of the digestive tract was treated first and then LCA was revealed.
Conclusion
LCA is an unusual benign spleen tumor that is often present with another visceral malignancy and can also mimic metastatic lesion of the spleen. Therefore, if this finding is diagnosed, the patient should be thoroughly screened to exclude tumor duplicity. However, the diagnosis of LCA is often difficult, and the definitive diagnosis is only determined by histological examination. Surgical treatment including splenectomy is the method of choice.
Footnotes
Author contributions
VO: writing of manuscript, VT: supervising, TW: pathological analysis, JM: data collection, writing of manuscript.
Availability of data and material
Please contact author for data request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Progres Q39 (Charles University research Program).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.