
Abstract
An 83-year-old man received pembrolizumab treatment after anticancer chemotherapy with gemcitabine and cisplatin for advanced bladder cancer. Pathological findings revealed invasive urothelial carcinoma with squamous differentiation before treatment. After seven courses of pembrolizumab treatment, the tumor disappeared. After 15 courses of the treatment, the tumor regrew. Pathological findings revealed invasive undifferentiated urothelial carcinoma consisting of relatively small tumor cells of the same size as lymphocytes, negative for neuroendocrine markers. Programmed death-ligand 1 expressions in tumor tissue changed from positive before treatment to negative after pembrolizumab treatment.
Keywords
Introduction
Programmed cell death-1 (PD-1) is an immuno-checkpoint receptor that is primarily expressed on T cells, monocytes, natural killer cells, and macrophages. Programmed death-ligand 1 (PD-L1) is the primary ligand of PD-1 and is expressed on the surface of dendritic cells and macrophages. In addition, PD-L1 is also expressed on a wide range of tumor cells, including urothelial cancer cells. 1 Immune checkpoint inhibitors (ICIs) such as pembrolizumab (anti-PD-1 antibody) are approved for platinum-refractory urothelial carcinoma. 2 A few patients have durable responses to treatment using an ICI; however, most patients experience progressive disease after the best response. There have been few reports of pathological comparison between the tissue before treatment and those of progressive disease after the best response to treatment using an ICI. We encountered a case of relapse after pembrolizumab treatment for invasive bladder cancer. Pathological findings before treatment were invasive urothelial carcinoma with squamous differentiation, and those of progressive disease after pembrolizumab treatment were undifferentiated urothelial carcinoma. In the present case, PD-L1 expressions in tumor tissue changed from positive to negative with pembrolizumab treatment.
Case report
An 83-year-old man complained of gross hematuria persisting for several days and visited our hospital in August 2017. Cystoscopy revealed papillary tumors on the anterior wall of the bladder. Computed tomography (CT) revealed a muscle-invasive tumor on the anterior wall of the bladder. Urine cytology was Class IV in five classes (negative, suspicious, and positive corresponding to Classes I–II, III, and IV–V, respectively). 3 We diagnosed the patient with invasive bladder cancer T2N0M0. The patient underwent transurethral resection of the bladder tumors (TUR-BT) in October 2017. Pathological findings revealed invasive urothelial carcinoma with squamous differentiation, high grade, G2 > G3, pT1 (Figure 1). The patient did not wish to undergo radical surgery. CT in December 2017 revealed that the tumor had increased in size (Figure 2(a)). Magnetic resonance imaging (MRI) in December 2017 showed that the tumor had invaded the surrounding bladder wall. We diagnosed the patient with invasive bladder cancer T3N0M0. He received anticancer chemotherapy with gemcitabine and cisplatin (GC). However, he developed severe myelosuppression. CT in March 2018 showed that the tumor had grown and invaded the surrounding bladder wall (Figure 2(b)). Therefore, we decided that chemotherapy was ineffective and changed the therapy to pembrolizumab treatment, 200 mg/dose, every 3 weeks. Immune-related adverse events did not develop during pembrolizumab treatment except for asymptomatic thyroiditis. After seven courses of pembrolizumab treatment, CT in September 2018 showed that the tumor had disappeared (Figure 2(c)). However, after 15 courses of the treatment, CT in March 2019 showed that the tumor had regrown (Figure 2(d)). MRI revealed a non-muscle-invasive tumor. Cystoscopy in March 2019 revealed a papillary tumor on the anterior wall of the bladder, again with satellite mucosal lesions. We diagnosed the patient with recurrent bladder cancer T1N0M0. The patient discontinued pembrolizumab treatment, and then underwent TUR-BT in May 2019. The tumor was completely resected. The pathological findings revealed invasive undifferentiated urothelial carcinoma, high grade, G2 consisting of relatively small tumor cells of the same size as lymphocytes, negative for neuroendocrine markers, pT1 (Figure 3). He received Bacillus Calmette–Guérin intravesical immunotherapy, 80 mg/dose, once a week, eight times for treatment with residual superficial mucosal lesions. However, cystoscopy in September 2019 showed the mucosal lesion on the anterior wall of the bladder that previously underwent TUR-BT. The patient did not wish to undergo surgery again. He was observed carefully. In April 2020, the size of the mucosal lesion on the anterior wall of the bladder was stable. Urine cytology was Class II.

Pathological findings before treatment revealed invasive urothelial carcinoma (UC) (luminal-type UC, papillary, G2, high grade (a) H&E stain, (b) GATA3 (+), (c) CK5/6 (−), (d) CK20 (+)) with squamous differentiation ((e) H&E stain, (f) CK5/6 (+), (g) p40 (+)).
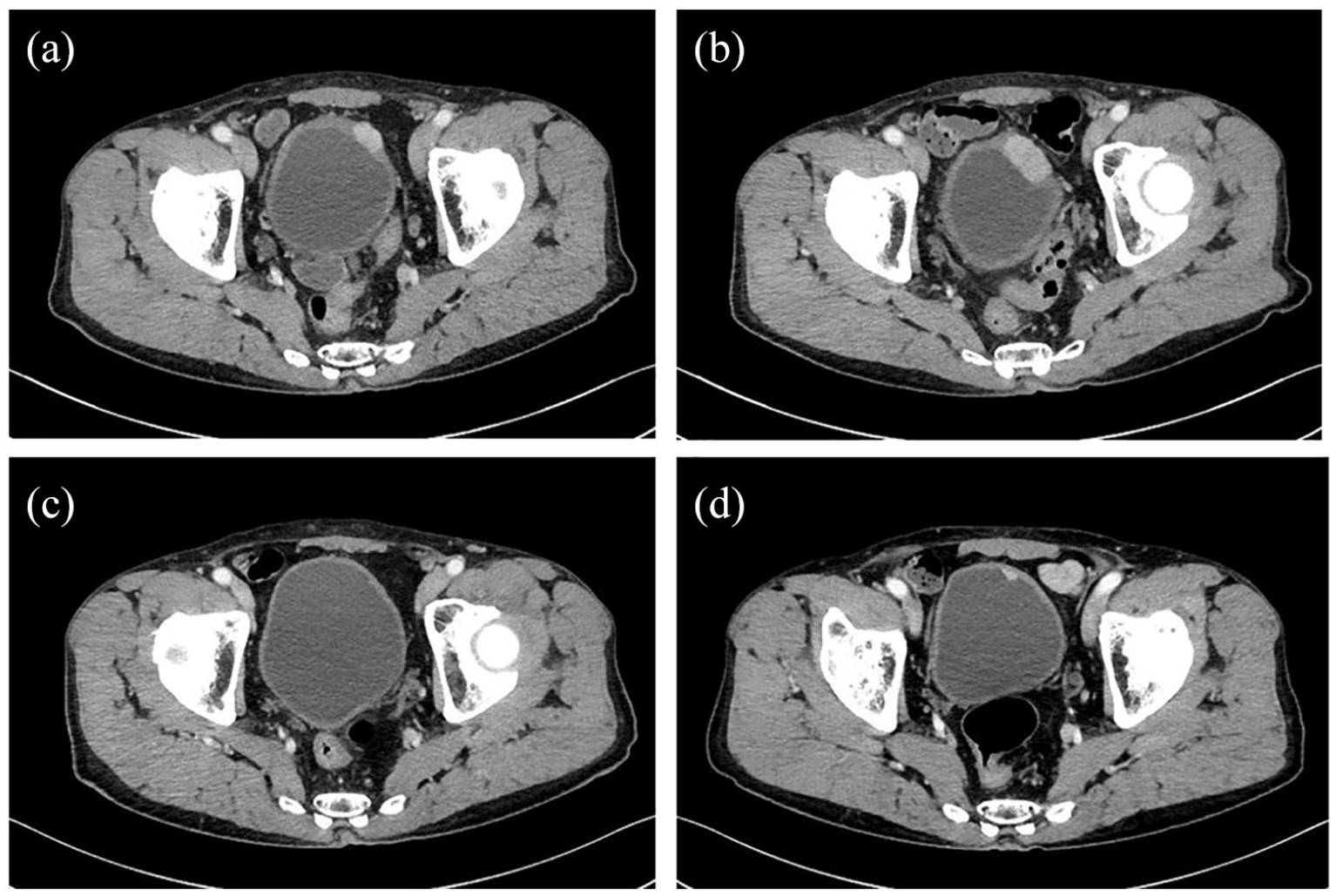
Computed tomography (CT) findings: (a) CT before treatment shows a muscle-invasive tumor on the anterior wall of the bladder, (b) CT before pembrolizumab treatment reveals the tumor invading the surrounding bladder wall, (c) CT shows the disappearance of the tumor after seven courses of pembrolizumab treatment, and (d) CT reveals tumor regrowth after 15 courses of pembrolizumab treatment.

Pathological findings revealed invasive undifferentiated double-negative UC, high grade, G2 ((a) H&E stain, (b) GATA3 (+), (c) CK20 (−), and (d) CK5/6 (−)) consisting of relatively small tumor cells of the same size as lymphocytes, negative for neuroendocrine markers.
Subsequently, we examined the tumor tissues using anti-PD-L1 antibody. The tumor tissues before treatment expressed PD-L1, with PD-L1-positive macrophages in the surrounding area (Figure 4(a)). The tumor tissue after pembrolizumab treatment barely expressed PD-L1, with PD-L1-positive macrophages in the surrounding area (Figure 4(b)).

(a) PD-L1 expression on the tumor before treatment. A total of 70%–80% of the tumor tissue expressed PD-L1, with PD-L1-positive macrophages in the surrounding area and (b) PD-L1 expression on the tumor after pembrolizumab treatment. Less than 10% of tumor tissue expressed PD-L1, with PD-L1-positive macrophages in the surrounding area.
Discussion
The standard first-line treatment of advanced urothelial carcinoma remains cisplatin-based chemotherapy, such as GC. 4 The effectiveness of these treatments against urothelial carcinoma has been confirmed, but they are associated with clinically significant toxicities, including myelosuppression, ototoxicity, neurotoxicity, and nephrotoxicity. Immuno-therapies that take advantage of the body’s immune system to fight cancer have started to be applied for patients with locally advanced or metastatic urothelial carcinoma. 2
PD-L1 expression has been reported to be associated with a poor prognosis in patients with urothelial cancer. 5 The mechanism underlying the antitumor activity of these drugs is immune checkpoint inhibitions, such as anti-PD-1 or anti-PD-L1 treatment. These treatments offer new treatment possibilities for patients who have historically had a few options available to them. Several ICIs, such as pembrolizumab, have been approved for second-line platinum-refractory urothelial carcinoma patients. In 2017, atezolizumab and pembrolizumab were extended to include first-line treatment in cisplatin-ineligible patients in the United States and Europe. ICIs have led to long-term durable responses and shown tolerable safety profiles in several clinical trials. However, approximately 70%–80% of patients may remain unresponsive to ICIs. Furthermore, a few patients show durable responses to treatment using an ICI; however, most patients experience progressive disease after the best response. There have been a few reports of pathological comparison between the tissue before treatment and those of progressive disease after the best response. Histologic transformation from non-small cell lung cancer to small cell lung cancer is a well-recognized mechanism of resistance in epidermal growth factor receptor (EGFR)-mutant adenocarcinoma upon treatment with tyrosine kinase inhibitors (TKIs). 6 There are a few published reports of histologic transformation upon treatment with PD-1 inhibitors in lung cancer; however, the molecular mechanisms leading to transformation have not been elucidated. 7 In the present case, histologic transformation might have occurred from differentiated urothelial carcinoma to undifferentiated urothelial carcinoma during pembrolizumab treatment. PD-L1 expressions in tumor tissue changed from positive before treatment to negative after pembrolizumab treatment. PD-L1 expression may predict the response to anti-PD-1 or anti-PD-L1 treatment.
Conclusion
We encountered a case of relapse with undifferentiated urothelial carcinoma after pembrolizumab treatment for invasive urothelial carcinoma of the bladder with squamous differentiation. PD-L1 expressions in tumor tissue changed from positive to negative with pembrolizumab treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.