
Abstract
Computed tomography–guided spine biopsy is a routine procedure in diagnosing vertebral infection or tumor. Following a thoracic intervertebral disc biopsy for presumed osteodiscitis, a patient immediately presented with flaccid paralysis and loss of temperature and pinprick sensation below biopsy level, followed rapidly by complete sensation loss. There was no evidence of direct injury during the biopsy, and emergent post-biopsy magnetic resonance imaging revealed no cord signal abnormality or compression. Later magnetic resonance imaging demonstrated corresponding-level cord edema, presumed secondary to transient cord ischemia during the procedures. Despite frequent utility, authors recommend caution in utilization of computed tomography–guided spine biopsy.
Keywords
Introduction
Computed tomography (CT)-guided biopsy of the spine is a routine procedure performed by interventional and musculoskeletal radiologists to obtain tissue samples for microbiology and pathology evaluation.1–6 The percutaneous vertebral biopsy was first described in 1949 by Siffert as a solution to the relative inaccessibility of the vertebral body in open biopsy techniques. 7 In this original technique, the needle was placed blindly by palpation only after careful study of plain radiographs. It was not until 1981 that the first CT-guided percutaneous technique was described and subsequently widely adopted for its ease and relative safety. 8
Compared to open surgical biopsy, the CT-guided percutaneous technique has been shown to decrease hospital stay, decrease medical cost, and have lower morbidity.4,5 Despite the proximity of vital structures to the vertebral column, rates of complication following the procedure are relatively low with documented rates of less than 10% for any complication and less than 1% for serious complication, with some studies even citing no complications.1,2,5,6,9 Typically, cited complications are attributed to a procedural technical error or needle tract damage. We present a case of acute spinal cord injury (SCI) resulting in complete paraplegia following a technically successful, appropriately performed CT-guided biopsy for thoracic osteodiscitis.
Case presentation
A 58-year-old female with chronic kidney disease stage 3, recurrent nephrolithiasis, hypertension, and morbid obesity (body mass index: 53 kg/m2) presented to the emergency room of a large academic medical center with 3–4 weeks of progressively worsening thoracic back pain and subjective fevers. She had no history of spinal surgery or chronic back pain. She did not have any history of implanted devices/prostheses (peripherally inserted central catheter (PICC), central line, orthopedic implants, pacemaker, etc.), and the patient was not immunocompromised. She endorsed sharp midline pain in her mid-thoracic spine which was non-radiating. On physical examination, she was neurovascularly intact with 5/5 strength in all muscle groups of her lower extremities, intact rectal tone, but was tender to palpation over the midline of her mid-thoracic spine. She had no long-tract tension signs and was not hyperreflexic. Laboratory findings were notable for erythrocyte sedimentation rate (ESR) of 112 (reference < 20) and C-reactive protein (CRP) of 16.5 (reference < 0.5). Blood cultures were obtained as part of infectious work-up which remained negative throughout the patient’s hospital course. A magnetic resonance imaging (MRI) (Figure 1) was obtained that demonstrated findings consistent with T5–T6 osteodiscitis without any evidence of cord compression or cord signal. The decision was made to treat conservatively with antibiotics in the setting of no cord threatening lesion, normal neurovascular exam, and morbidity associated with surgery.10,11 She was admitted to the hospital and was started on empiric broad-spectrum intravenous (IV) antibiotics which were continued for 36 h with continued fevers and without significant improvement in symptoms. In an effort to help guide targeted antibiotic therapy, a CT-guided bone biopsy was performed by musculoskeletal radiology. The intent was for the sample obtained to be used in confirmation of diagnosis and also for bacterial culture and antibiotic sensitivity testing. The biopsy was performed under general anesthesia due to the patient’s body habitus, inability to tolerate prone positioning for the duration of the biopsy, and anxiety. The procedure was performed without technical difficulty. Figure 2 is an axial image from the patient’s CT scan during the biopsy which demonstrates appropriate needle positioning during the procedure as described in the technical literature.1,5,6,8,12
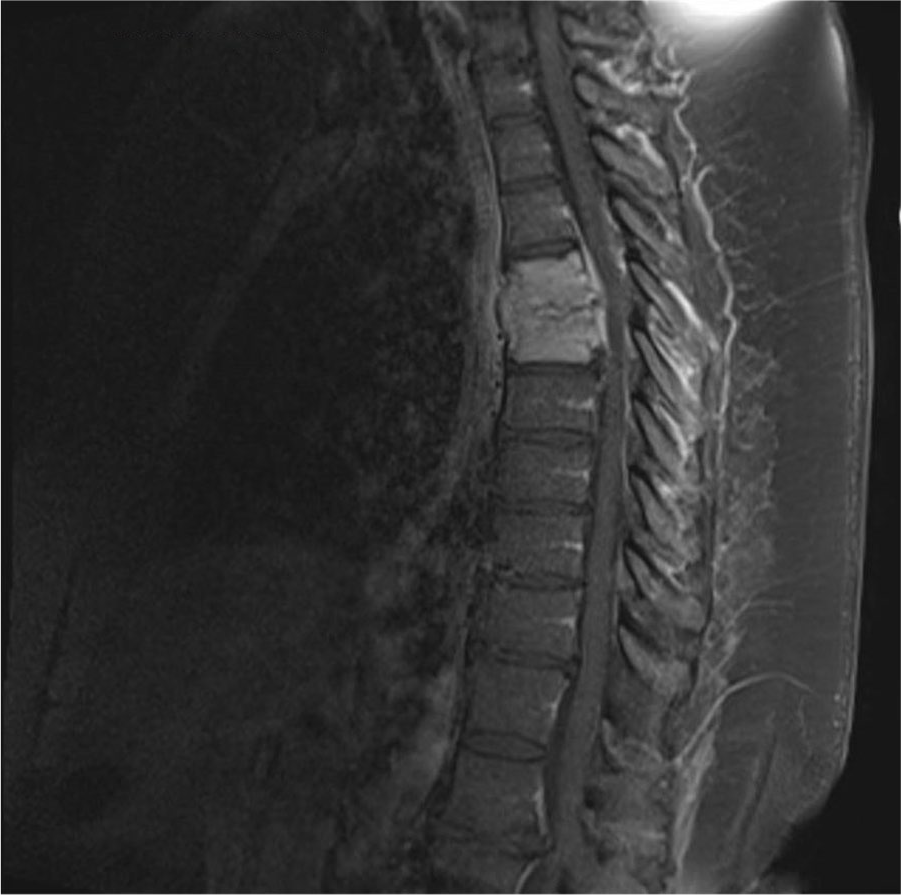
Sagittal T2 MRI post-contrast image of the patient’s thoracic spine demonstrating findings consistent with T5–T6 osteodiscitis without any evidence of cord compression or cord signal, at the time of presentation.
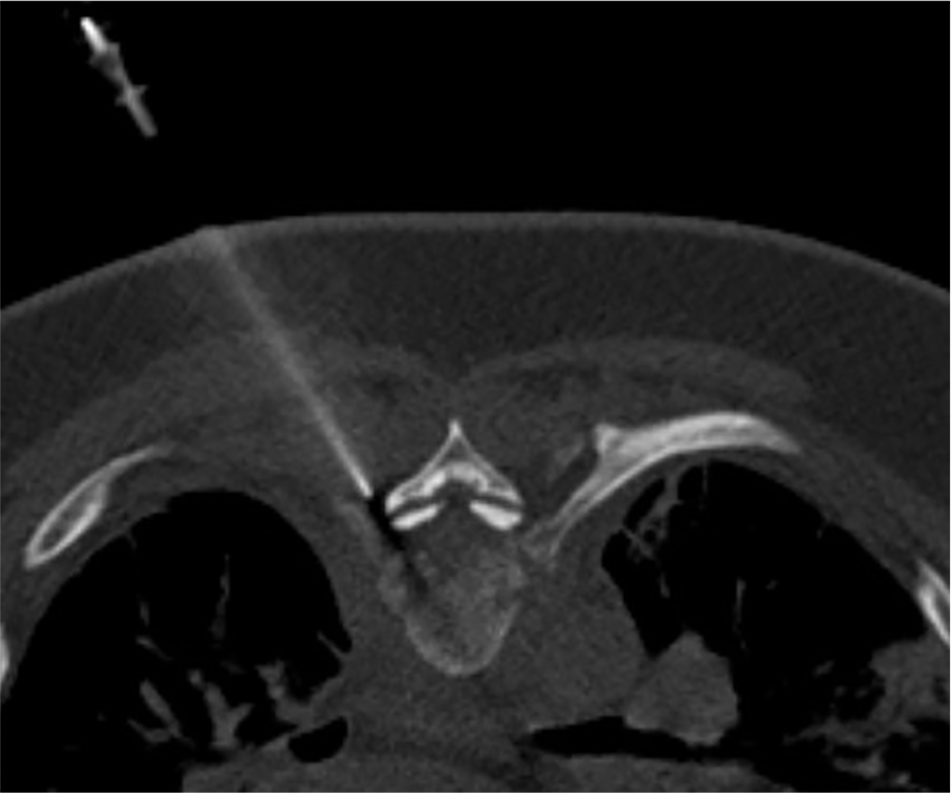
Axial CT image from biopsy performed, confirming appropriate needle positioning during the procedure.
Immediately following the biopsy and after anesthesia emergence, the patient reported an acute change in neurologic status. Immediate physical examination revealed complete loss of motor function in the bilateral lower extremities, T5 sensory level with absent posterior and lateral column/tract sensation (proprioception, pinprick, temperature), intact anterior spinothalamic tract (light touch), intact rectal tone, and present bulbocavernosus reflex (ASIA B). An emergent MRI revealed no evidence of cord signal abnormality or compressive epidural hematoma (Figure 3). The patient’s examination rapidly deteriorated to complete flaccid paralysis and loss of all sensation below the T5 level over the next 60 min (ASIA A). The patient was subsequently transferred to the intensive care unit (ICU) for close neuromonitoring and maintenance of mean arterial pressure goals greater than 80 mmHg. The patient’s examination and clinical parameters remained unchanged and she was continued on empiric IV antibiotics for her osteodiscitis. She was discharged from the hospital to a skilled care facility 1 week later.

Sagittal T2 MRI post-contrast image of the patient’s thoracic spine demonstrating findings consistent with continued T5–T6 osteodiscitis without evidence of cord signal abnormality or compressive epidural hematoma, immediately following biopsy and recognition of flaccid paralysis.
Eight months following SCI, she has had no recovery in neurologic function. Her course has additionally been complicated with a stage 4 sacral decubitus ulcer, numerous indwelling urinary catheter infections, and bilateral full thickness necrotic pressure wounds to her heels and plantar feet. Of note, MRI 7 weeks post-biopsy revealed T5–T6 cord signal change and edema consistent with SCI at that level.
Discussion
CT-guided percutaneous biopsies are common procedures with diagnostic accuracy of spinal lesions estimated from 67% to 97% in the literature.1,3,9,12 There are five major indications for CT-guided percutaneous biopsy: unknown spine mass, expected infectious lesion not responding to empiric antibiotics, discitis with failure to improve in a child, intractable or worsening back pain along with a vertebral compression fracture, or increasing pain in a patient with Paget’s disease of the spine.3,5 The caveat to this is that while useful in the thoracic spine, diagnostic accuracy and quality of sample is significantly poorer in the thoracic spine.3,6 This is thought to be due to anatomy-related technical challenges in obtaining the CT-guided sample, making thoracic vertebral biopsy the most technically dangerous.2,6,9 The Infectious Disease Society of America (IDSA) publishes periodic practice recommendations which does recommend obtaining a sample for culture and antibiotics testing unless blood cultures were found to be positive within the 3 months prior to presentation. 13 The IDSA goes on to provide a strong recommendation against obataining a tissue sample in the setting of positive blood cultures. There is some variability within the literature regarding the necessity of obtaining a sample for microbiological study. Some authors advise simply initiating empiric antibiotic treatment and go on to report and cite high cure rates. Other authors advise that antibiotic therapy with a course of external immobilization is appropriate and this has been well cited in the literature.10,11,14
In the case presented, there is no evidence of direct injury to the cord verified both by intra-procedure CT and emergent post-procedure MRI (Figures 2 and 3, respectively). Multiple hypotheses exist and include procedure hypotension, needle misplacement, iatrogenic positioning injury, or reticular spinal cord branch injury. The exact etiology is unclear; however, after multi-disciplinary root cause analysis, a single theory has prevailed. During the biopsy procedure, which was performed under general anesthesia, there was a period of relative hypotension when compared to the patient’s hypertensive baseline. The exact duration is unknown as the patient data logging system only records every 15 min, but at one point during the biopsy, the patient’s blood pressures were as low as 80/40 mmHg. It is believed that in the setting of the increased metabolic demand from the neighboring infection, the mild compression from bulging area of osteodiscitis, and with the patient’s hypertensive baseline, this short period of hypotension resulted in an ischemic insult to the thoracic spinal cord. The 7-week post-biopsy MRI demonstrates cord edema at this level which would be consistent with this theory. This is further supported by the presence of a bulbocavernosus reflex immediately following the insult. The presence of this reflex demonstrates the absence of spinal shock as would be more likely to be present following a traumatic insult to the spinal cord. 15
To the author’s knowledge, this is the first report of flaccid paraplegia following a CT-guided biopsy of the thoracic spine despite the often cited theoretical risk. Neurological injury including SCI is a well-documented risk of the percutaneous procedure, but most reported neurological complications pertain to nerve root irritation and are transient in nature.2,9 This case report highlights the relative unpredictability of invasive CT-guided procedures of the thoracic spine and devastating potential outcomes.
Conclusion
The CT-guided percutaneous biopsy of the spine has revolutionized orthopedic and neurosurgical medical care, but this case report serves as a reminder that any invasive procedure, no matter how routine, puts our patients at risk for a potentially devastating complication. The authors would urge for careful consideration of the clinical risks and benefits in collaboration with their patients prior to a vertebral biopsy and advise against the use of general anesthesia for the procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting anonymized individual cases or case series.
Informed consent
Written informed consent was obtained from the patient directly who had/has decisional capacity to provide informed consent for anonymous patient information to be published in this article.