
Abstract
This case report describes a novel presentation of a lichen planus and dermatomyositis overlap syndrome. The patient presented with pruritic and painful violaceous erythroderma with biopsy reports suggestive of both lichen planus and dermatomyositis. The patient failed first-line treatment with prednisone and hydroxychloroquine and eventually required treatment with methotrexate and intravenous immunoglobulin to achieve control of her disease. Overlap syndromes have been described between lichen planus and lupus erythematosus; however, to date, little has been described about a dermatomyositis/lichen planus overlap.
Introduction
Overlap syndromes are described as two or more autoimmune conditions manifesting in the same patient. 1 Dermatomyositis (DM) is a rare idiopathic inflammatory myopathy with clinically amyopathic dermatomyositis (CADM) representing up to 20% of the cases. Erythroderma is an uncommon presentation of DM with only six case reports of DM presenting with erythroderma to date. 2 Lichen planus (LP) is a chronic inflammatory disease that can affect the skin, mucosal surfaces and nails; 3 it typically favours the extremities and rarely presents as erythroderma – in a case series of 80 patients presenting with erythroderma, only one was as a result of LP. 4
Case report
A 66-year-old female presented to the Dermatology clinic with violaceous erythroderma, eruptive seborrheic keratosis and alopecia. She had a medical history of oral LP for 3 years, atrial fibrillation and asthma. The patient initially had a rash on her anterior chest that developed to involve more than 90% of her body surface area over 2 months. The rash did not respond to a short course of prednisone 50 mg po od. Prior to referral to Dermatology clinic, the patient had a biopsy that showed compact orthokeratosis, wedge-shaped hypergranulosis, jagged epidermal hyperplasia and a band-like infiltrate of lymphocytes and histiocytes associated with interface changes and was interpreted as LP.
Upon presentation to Dermatology clinic, the patient had violaceous erythroderma, periocular swelling, hyperkeratotic scale throughout her scalp and experienced intense pruritus and pain that would wake her from sleep. Due to the violaceous colour of her skin, likely heliotrope rash, and lack of clinical response to prednisone, repeat biopsies were performed to evaluate for possible DM. The repeat biopsies showed vacuolar interface changes at the dermal–epidermal junction with numerous scattered dyskeratotic keratinocytes, some spongiosis with minimal acanthosis in the epidermis, and overlying focal areas of parakeratosis in the stratum corneum, favouring a diagnosis of DM, with LP as a possible alternative diagnosis. Blood test revealed positive antinuclear antibody (ANA, 1:320) but negative anti–double-stranded (ds) DNA and anti–extractable nuclear antigen (anti-ENA) antibodies. Other blood tests, including complete blood count (CBC), liver and renal function, and serum protein electrophoresis, were unremarkable. Malignancy workup, including computed tomography (CT) chest/abdomen/pelvis, pelvic ultrasound, mammogram and colonoscopy, was normal. Physical examination revealed no dysphagia, muscle weakness, Raynaud’s syndrome or oral ulcers, and she had no associated constitutional symptoms.
The patient was referred to Rheumatology clinic for further evaluation and was initially treated with hydroxychloroquine (HCQ) 200 mg po BID and prednisone 20 mg po od. After 2 months of treatment, the patient remained erythrodermic and developed ‘hiker’s feet’ (Figure 1) and ‘mechanic’s hands’ with deep, painful fissuring of her palms and soles. She was then started on methotrexate (MTX) 25 mg sc weekly and intravenous immunoglobulin (IVIg) 2 g/kg monthly. The HCQ was reduced to 200 mg od as she was experiencing more frequent episodes of atrial fibrillation. The erythroderma and palmoplantar hyperkeratosis responded to MTX and IVIg and the patient’s skin manifestations slowly began to resolve.

Hiker’s foot.
Discussion
Both DM and LP are rare causes of erythroderma.2,4 The punch biopsy results favoured LP the first time and DM with LP on the differential the second time. Differing results and an atypical presentation for either disease begged the question of whether this could be a DM/LP overlap syndrome presenting with erythroderma or whether one disease process was favoured over the other.
There are no official diagnostic criteria for LP; it is a clinical diagnosis confirmed by biopsy. Our patient did not have a classic clinical presentation of LP, and the second punch biopsy favoured DM over LP, making it a diagnostic dilemma.
There are a number of diagnostic criteria for DM – the first set of criteria was developed by Bohan and Peter in 1975 (Table 1). 5 In 2003, the Dalakas and Hohlfeld’s criteria were developed to include CADM (Figure 2). 5 Our patient only met one of five of the Bohan and Peter criteria, but did meet three of five of the Dalakas and Hohlfeld’s criteria. While the dermatologist believed her periocular findings to be in keeping with a heliotrope rash, the rheumatologist was not entirely convinced.The development of ‘mechanic’s hands’ and poikiloderma after 6 months into the disease process eventually enabled both teams to lean towards CADM.
Bohan and Peter criteria, 1975. 5
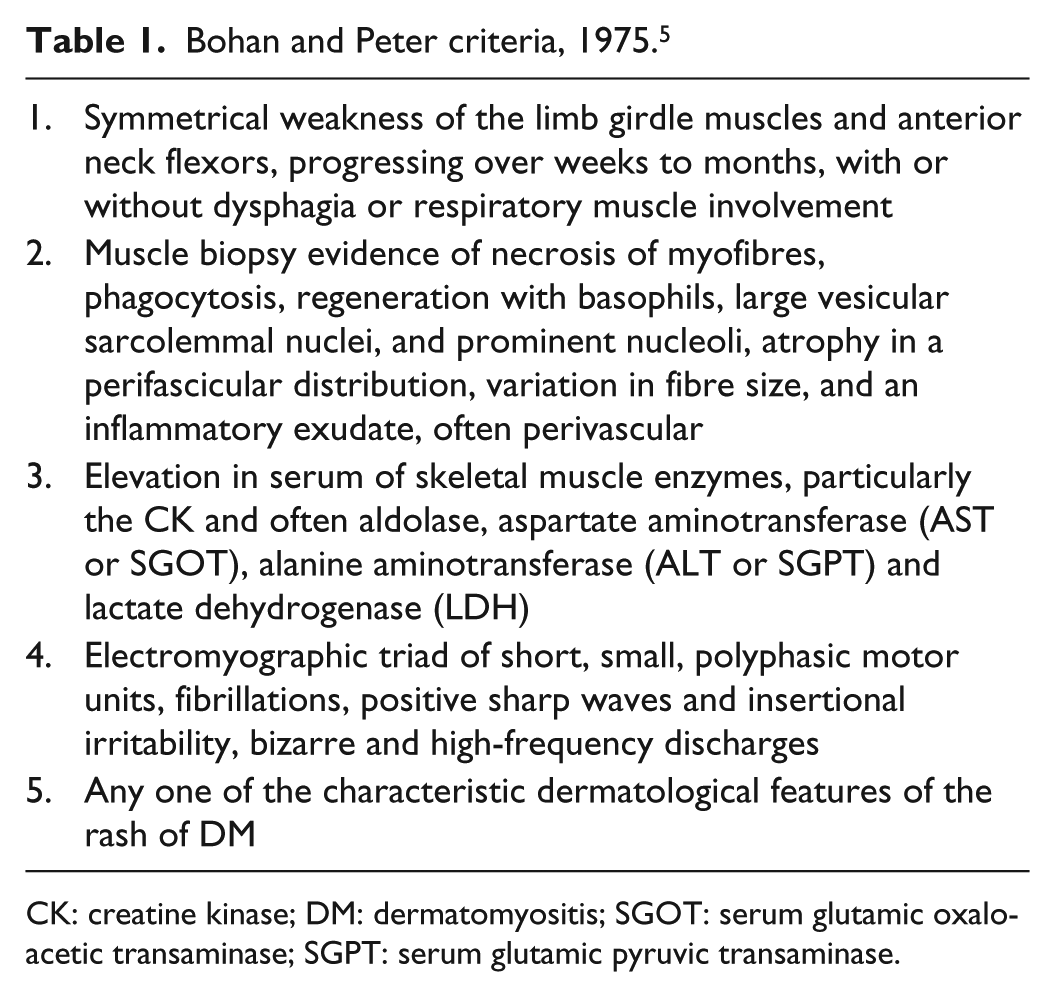
CK: creatine kinase; DM: dermatomyositis; SGOT: serum glutamic oxaloacetic transaminase; SGPT: serum glutamic pyruvic transaminase.

Dalakas and Hohlfeld’s criteria, 2003. 5
DM can be considered clinically amyopathic when there is no evidence of muscle disease on physical examination or on laboratory investigations for at least 6 months. 5 The literature proposes that there is no difference between the two regarding systemic associations with malignancy, interstitial lung disease and cutaneous findings. 6 Our patient was worked up extensively for an underlying malignancy; however, her screening tests were all negative.
Approximately a quarter of patients with early-stage rheumatologic disease meet the criteria for an overlap syndrome. 1 A case report describing a lupus erythematosus (LE)/LP planus overlap defined an overlap as a lesion having features of both diseases and a coexistence as two separate lesions exhibiting two separate disease characteristics. 7 By this definition, our patient presented with a DM/LP overlap. While a DM/LP overlap has not been formally defined, a publication from 1985 described two cases where the histopathology was consistent with LP but the clinical picture was typical of DM. 8
There is conflicting evidence about whether overlap syndromes are more treatment resistant than either disease entity alone. 9 Prednisone is a first-line treatment for both LP 10 and DM. 5 Our patient was showing no signs of improvement on prednisone and HCQ initially, and it was with the addition of MTX and IVIg that her symptoms began to resolve.
Recognition of overlap syndromes is important as they can establish prognosis and aid in tailoring management of specific features of the disease. In this case, the overlap syndrome of DM/LP presented in an atypical fashion for either disease – erythroderma – and required a number of immunosuppressive therapies to control disease progression.
We propose that this case represents a novel clinical entity – an LP/DM overlap syndrome in an erythrodermic patient with clinical and histopathological features of both LP and DM. Whether DM/LP overlap is a true clinical entity and whether it requires more aggressive medical management is a question that can only be answered with further research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent for patient information and images to be published was provided by the patient on 24 May 2018.