
Abstract
Solitary fibrous tumors are rare mesenchymal tumors most commonly arising from the pleura. When associated with paraneoplastic syndrome of hypoglycemia caused by the secretion of a high-molecular-weight form of insulin-like growth factor II, it is referred to as the Doege–Potter syndrome. Surgery with complete tumor resection is the only curative treatment. We present here the case of a 93-year-old female diagnosed with a Doege–Potter syndrome who underwent three repetitive surgical resections of recurrent solitary fibrous tumor.
Keywords
Introduction
Solitary fibrous tumors (SFTs) are rare mesenchymal tumors most commonly arising in the pleura, with 800 cases described in the literature since it was first described by Klemperer and Rabin in 1931. 1 They can also occur in extrapleural locations like in the lung, liver, orbit, nasal passages, skin, thyroid, and gastrointestinal tract. 2 Most SFTs are asymptomatic and incidentally found on chest radiography. 3 However, some tumors may induce dyspnea, chest pain, and cough due to important size or localization. These tumors may also potentially cause extrathoracic symptoms, such as hypertrophic pulmonary osteoarthropathy and refractory hypoglycemia, due to the production of a growth hormone–like substance and an insulin-like growth factor (IGF-II), respectively. 2 When hypoglycemia is associated with an SFT, it is referred to as the Doege–Potter syndrome. Majority of the tumors are benign, but 10%–20% are malignant. 1 Benign SFTs can be cured by complete surgical resection. Recurrences are frequent (9.9%) but second recurrences are exceptional. Here, we describe the case of a 93-year-old woman who underwent three repetitive surgical resections for recurrent SFT associated with refractory hypoglycemia.
Case presentation
A 93-year-old female was referred for recurrent SFT of the right pleural cavity. From the beginning, she demonstrated refractory hypoglycemia and underwent two resections of large SFT by right thoracotomy in 1993 and 2004. The second procedure included residual tumor excision, resection of the fourth, fifth, and sixth ribs followed by chest wall reconstruction. The histopathologic analysis confirmed a benign SFT of the pleura with marginal resection. After a long disease-free interval, she developed a second recurrence 10 years later with repetitive refractory hypoglycemia. Glycemic values ranged between 2.1 and 5.3 mmol/L without administration of intravenous glucose. Chest computed tomography (CT) scan showed two recurrent lesions, the largest measuring 13 × 18.5 cm2 in close contact to the chest wall and infiltrating the apical segment of the right lower lobe (Figure 1). Transient normalization of the gylcemia was obtained after two successive arterial embolizations. Finally, the patient remained symptomatic with refractory hypoglycemia and a third surgical resection was proposed. She underwent “en bloc” resection of previous reconstruction of the chest wall with two recurrent SFTs and apical segment of the right lower lobe (Figure 2). Chest wall was reconstructed with mesh and titanium plates (Figure 3). Glycemia was immediately normalized on postoperative course, with values ranging between 6.4 and 10.5 mmol/L. Pathological exams revealed the presence of benign SFT with marginal resection. The patient was discharged on postoperative day 14.
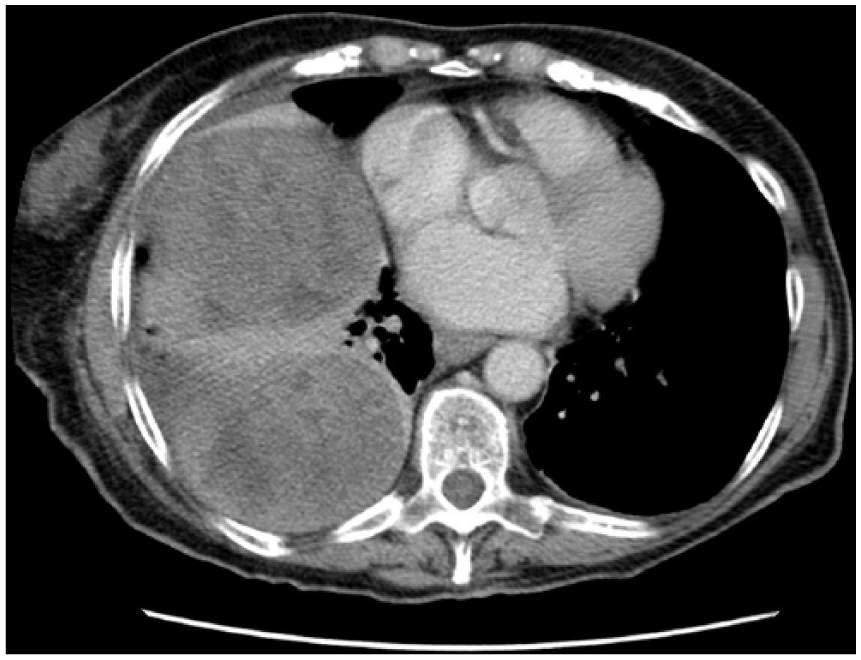
Chest CT scan of the first SFT recurrence in 2004 showing a right large pleural mass with suspected infiltration of the chest wall.

(a, b) Chest CT scan of the second recurrence with two large vascularized pleural masses, despite the two previous arterial embolizations.

Postoperative chest radiography showing the reconstruction of the chest wall with plates and previous coils in intercostal arteries.
Discussion
SFTs of the pleura are rare neoplasms that account for <5% of all pleural tumors. 3 These tumors occur mainly in adults with a peak age of 60–80 years and are equally distributed between genders. The etiological factors are unknown and no risk factor has been identified yet.
Patients with SFT of the pleura are usually asymptomatic and the tumor is discovered incidentally on chest radiography or CT scan. About 50% of the patients may present with dyspnea, cough, and pleuritic chest pain. Paraneoplastic syndrome, such as hypoglycemia or hypertrophic pulmonary osteoarthropathy, may occur in 3%–4% of SFT.1,4 Associated refractory hypoglycemia is reported as Doege–Potter syndrome and is caused by the inappropriate secretion of a high-molecular-weight form of IGF-II. This molecule activates insulin receptors, inhibiting hepatic gluconeogenesis and increasing glucose uptake, which results in hypoglycemia. The laboratory tests show suppressed serum insulin, C peptide, and low IGF-I against the levels of IGF-II that are either normal or elevated. 5
The diagnostic radiologic tests include chest radiography which is not specific and CT scan which can identify a smooth, well-circumscribed, homogeneous mass with or without necrosis or calcifications. Magnetic Resonance Imaging (MRI) and fluorodeoxyglucose positron emission tomography (FDG-PET) are also of some benefit for the diagnosis but less often used. 5
The only definitive treatment is complete surgical excision.1,5–7 For nonresecable and metastatic tumors, chemotherapy and consecutive selective embolization of the feeding vessels of the tumor can be tried to alleviate symptomatic hypoglycemia, but they are not effective treatments. 5 Radiotherapy may be proposed as an adjuvant treatment after surgery in case of marginal resection for malignant SFT. 5
Local recurrence is relatively frequent with a recurrence rate estimated at 9.9%. 7 The incidence of recurrence is more frequent in malignant SFT in comparison with benign SFT (75% vs 25%). 7 Repeated recurrences are rare after complete surgical resection like in our case. Interestingly, both recurrences were recognized because the patient developed symptomatic and refractory hypoglycemia. After the second recurrence, the patient required continuous perfusion of glucose to maintain normal glycemia. Immediately after surgery, glycemia normalized and the quality of life was subjectively greatly improved for the patient. Few cases of recurrence after complete resection have been reported.6,7 Extended surgical resection may be necessary for lesion invading the chest wall, lung, diaphragm, or pericardium. In our patient, chest wall resection was undertaken in both recurrent surgeries with acceptable morbidity despite the advanced age of the patient.
In conclusion, repeated recurrences in SFT are rare after previous surgical resection. Repetitive thoracotomies after chest wall reconstruction can be technically difficult and questionable, especially in old patients. But since the benefits of the surgery outweigh the risks, it should still be considered and discussed with the patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.