
Abstract
Objectives:
Spine injuries seldom affect the subaxial spine in children less than 9 years of age. We describe the management of a chronic paediatric bilateral facet dislocation.
Methods:
Case report and literature review. A 6-year-old boy presented 10 weeks after a motor vehicle collision with bilateral C4–C5 malunited facet dislocation. He had an incomplete spinal cord injury; right brown sequard hemiplegia, Frankel grade D.
Results:
Surgical management was through posterior–anterior–posterior approach without preoperative skull traction. Two years postoperatively, the child was asymptomatic, ambulating and functioning well. The injury had healed in radiographs.
Conclusion:
A combined approach for chronic bilateral facet dislocation applies to the paediatric age group to realign the spine.
Introduction
Spine injuries are rare in the paediatric population and are inherently different. Motor vehicle collisions are the leading cause of such injuries. In patients less than 9 years of age, the upper cervical region is more frequently affected compared with the subaxial vertebrae. Moreover, approximately 50% will have a spinal cord injury on admission.1,2
Facet dislocation (FD) on the subaxial spine is secondary to flexion distraction force. 3 Chronic presentation is defined as more than 3 weeks from the injury, and adds to treatment complexity.4,5 The delay in presentation might be secondary to missed diagnosis or a failure to transfer the patient to a specialised centre in a timely fashion.
There are a few reports of acute FD and chronic unilateral FD in patients less than 9 years of age, but chronic bilateral FD has not been reported.6,7 The aim of this report is to highlight the importance of combined surgical approaches.
Case report
Presentation
A 6-year and 2-month-old boy who was admitted to our institution 10 weeks after a rollover motor vehicle collision. The child was ejected and found transiently unconscious and hypotensive. At the local hospital, he was intubated and underwent immediate exploratory laparotomy where a splenectomy was performed. He also had a right tibia fracture that was treated with immobilisation. The cervical spine injury was detected while recovering from the laparotomy. His initial cervical radiographs and magnetic resonance imaging (MRI) were obtained after noticing right-sided weakness (Figure 1(a) and (b)). The family brought the child to our institution after his tibia fracture had healed. The neurological assessment at arrival revealed a Frankel grade D incomplete spinal cord injury. Right brown sequard hemiplegia was documented. There was more motor weakness in the right upper extremity, especially of the hand along with sensory loss in the left hand. A repeated MRI that was done under fiberoptic intubation with general anaesthesia on the way to the operating room showed improvement of the abnormal signal intensity and reduction of the impinging C4-5 disc (Figure 1(c)).

Preoperative images. (a) Lateral radiograph showing antrolesthesis of C4 on C5 with more than 25% translation indicating biarticular injury. (b) Parasagittal T2 weighted MRI at the local hospital showing cord oedema and disc herniation. (c) Repeated MRI 10 weeks later.
Operative procedure
We did not perform skull traction as the CT scan did show at least partial healing of the dislocated facets (Figure 2), and we started posteriorly because remodelled facets were felt to be restrictive to any anterior manipulation. Altering the natural facet articulation for the posterior release increases instability even after reduction and because of the small C4 lateral mass, we instrumented two vertebrae above and below the injured level.

Computerised tomography (CT). (a) 3D images of the bilateral facet dislocation (arrows). (b) The right dislocated facet with partial union. (c) The left ‘perched’ facet.
The surgical procedure constituted three approaches, starting posteriorly for facets release, which did not result in reduction (Figure 3(a)), then anteriorly where we did a C5 corpectomy as well as discectomy of the adjacent discs. For the reduction, standard techniques were employed to realign the vertebrae. 8 Despite the small size of the vertebrae, we were able to place divergent distraction pins and used them effectively (Figure 3(b)). After the reduction, a structural allograft was placed followed by an anterior plate. We then turned the patient prone again and placed lateral mass screws and rods. The fixation was extended between C3 and C6. Due to anatomical constraints, the C4 lateral masses were not instrumented. The transcranial motor evoked potentials deteriorated momentarily twice: first, after log-rolling to the prone position while adjusting the Mayfield frame before we started the procedure, which improved once we flexed the neck slightly and corrected translation; and second during an attempt at reduction anteriorly using a laminar spreader. The deterioration resolved immediately after the release of the distraction. Although the C4-5 facets were released posteriorly, the anterior lamina spreader did not lead to satisfactory realignment under fluoroscopic assessment. Postoperatively, he was kept intubated for 2 days in the intensive care unit. He was then admitted to the rehabilitation hospital for 4 weeks and used a semi-rigid cervical collar for 3 months.

Intraoperative images. (a) The injured facets are shown in the clinical photograph. (b) The reduction manoeuvre used.
Outcome
During rehabilitation, the patient regained independent ambulation without walking aids or orthoses. At 2-year follow-up, the patient had no pain or functional limitations, and there was no notable restriction in neck range of motion or a limp. His neurological exam improved, but remained Frankel grade D. He was able to write clearly with his right hand. The final radiographs showed union (Figure 4(a) and (b)).

Final radiographs 24 months postoperatively. (a) Anteroposterior. (b) Lateral.
Discussion
Chronic healed FD is a distinct entity that requires unique management strategies that are summarised in Table 1.4,8,9 Subsequent reports in an adult age group are primarily a variation of the earlier reports.
Summary of the reviewed literature on the treatment of chronic subaxial facet dislocations.
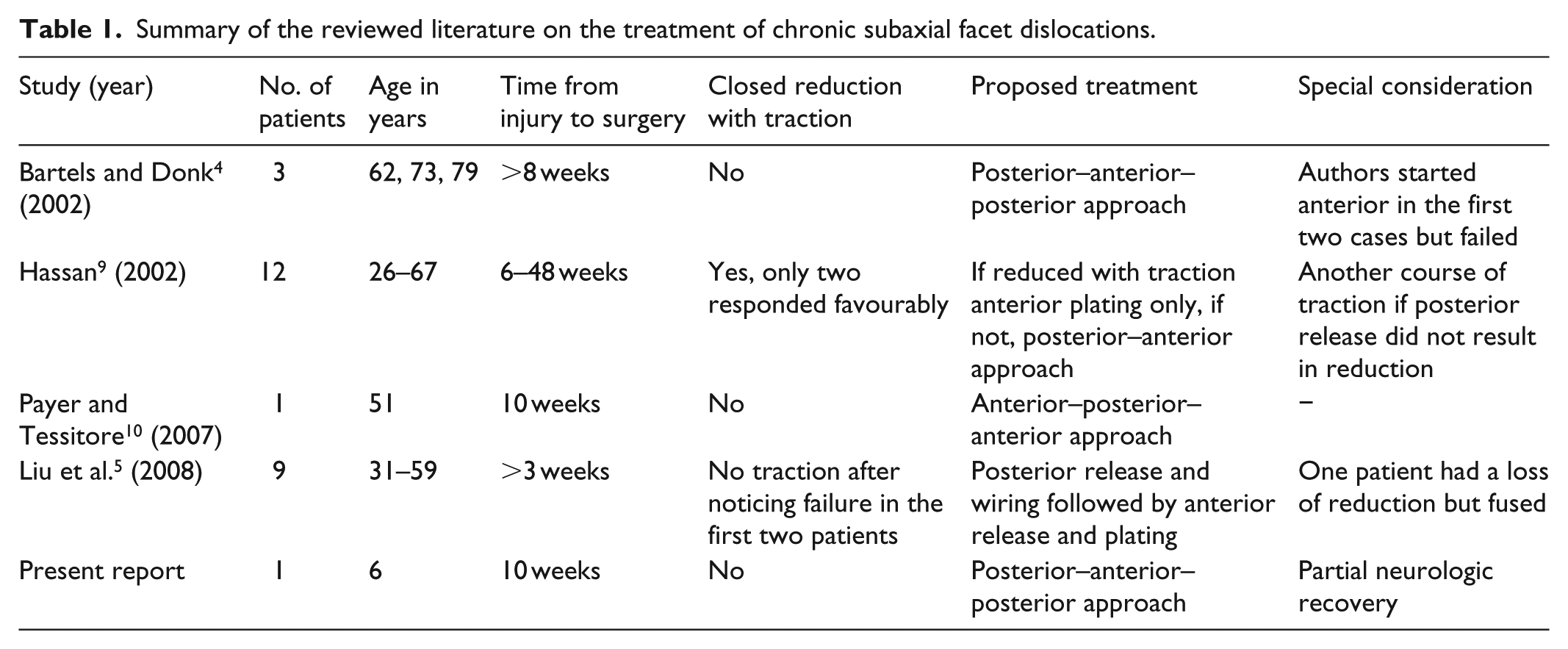
We are not aware of any published case of chronic bilateral FD in the paediatric population. Cobanoglu et al. 6 treated a 9-year old who presented 3 months post-injury with locked unilateral perched facet with a combined posterior, then anterior reduction and fixation. Faschingbauer et al. 11 reported a unilateral facet dislocation in a 12-year-old girl that was treated by posterior open reduction and tension band sutures. She subsequently developed bilateral dislocation with neurological compromise requiring reduction and anterior–posterior stabilisation. Parada et al. 12 reported their experience in an acute unilateral facet dislocation in a 9-year-old boy that was successfully treated by closed reduction under general anaesthesia followed by a rigid cervical collar for 12 weeks. Chen et al. 13 treated a 22-month-old girl with a unilateral dislocation using a posterior approach and titanium miniplates. Sellin et al. 14 reported on eight children with unilateral facet injuries along with their surgical management, however, only one subject in the cohort was under 10 years of age. Quinn et al. 7 used posterior reduction and fixation in a 4-year-old child, where lateral mass screws were used on one side and sublaminar wire on the other side for bilateral perched facets. Qu et al. 15 reported on a 5-year-old who presented with unilateral jumped facet, and they had deterioration in neurophysiology signals during closed reduction. Therefore, they performed an open posterior reduction and used a bioabsorbable plate for stabilisation.
The reference standard is to use an autograft anteriorly, but based on the family’s preference, we used a structural allograft. 16 In a recent report of 18 cases of allografting of the paediatric cervical spine, the fusion rate was 87%. 17 Concerns related to subaxial spinal growth after arthrodesis remain theoretical as the spinal canal diameter reaches an adult size by 6 years of age. 18
Finally, the Advanced trauma life support (ATLS) protocol was not followed during resuscitation in the peripheral hospital, and this may have impacted the identification and prevention of the spinal cord injury and early definitive treatment.19,20
Conclusion
This case report discusses the applicability of a 540-degree approach to chronic bilateral facet dislocations in a 6-year-old child. Careful intraoperative head positioning and judicious use of distractive force are paramount. The long-term effect of spinal instrumentation in the growing cervical spine remains unknown.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from King Fahad Medical City, Institutional Review Board (log number 17-076).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorised representative(s) for anonymised patient information to be published in this article.