
Abstract
Background:
Schizophrenia is a chronic disease that requires long-term management with antipsychotics; however, an important barrier to the success of long-term treatment is drug noncompliance, which increases the risk of recurrence and hospitalization. Second-generation long-acting injectable antipsychotics have improved drug adherence, and the pharmacological effects of the drugs, and therefore, have become useful treatment options.
Methods:
We report on three schizophrenia patients who switched from oral low-dose aripiprazole to aripiprazole once-monthly 300 mg. We examined the efficacy and safety of aripiprazole once-monthly 300 mg, as well as its influence on quality of life, from baseline to 20 weeks after aripiprazole once-monthly 300 mg treatment.
Results:
Aripiprazole once-monthly 300 mg did not exacerbate the depressive and negative symptoms, and extrapyramidal symptoms were improved, which may have helped improve the quality of life.
Conclusion:
The results suggest the efficacy of aripiprazole once-monthly 300 mg in maintenance treatment for schizophrenia when mental symptoms are stable.
Keywords
Introduction
Schizophrenia is a chronic disease that requires long-term management with antipsychotics; however, an important barrier to the success of long-term treatment is drug noncompliance, which increases the risk of recurrence and hospitalization. 1 Second-generation long-acting injectable antipsychotics have improved drug adherence, and the pharmacological effects of the drugs, and therefore, have become useful treatment options. 2 We report on three schizophrenia patients who switched from oral low-dose aripiprazole to aripiprazole once-monthly 300 mg (AOM 300). As preliminary results, we already reported the effects of AOM on cognitive function of the other two schizophrenia patients. 3 In addition, we examined the efficacy and safety of AOM 300, as well as its influence on quality of life (QOL), from baseline to 24 weeks after AOM treatment.
Case report
Three patients fulfilled the following criteria for at least 3 months prior to switching, and their mental symptoms were stable: (1) Positive and Negative Syndrome Scale (PANSS) 4 total score <70. (2) A score below 3 for all the parameters in PANSS, namely, conceptual disorganization, hallucinatory behavior, suspiciousness, and unusual thought content. (3) Clinical Global Impression–Severity (CGI-S) 5 score below 3 (Table 1). Written informed consent was obtained from the patients. Their anonymity has been preserved. QOL was assessed using the Heinrichs–Carpenter Quality-of-Life Scale (QLS). 6
Subject characteristics.

CGI-S: Clinical Global Impression–Severity scale; PANSS: Positive and Negative Syndrome Scale.
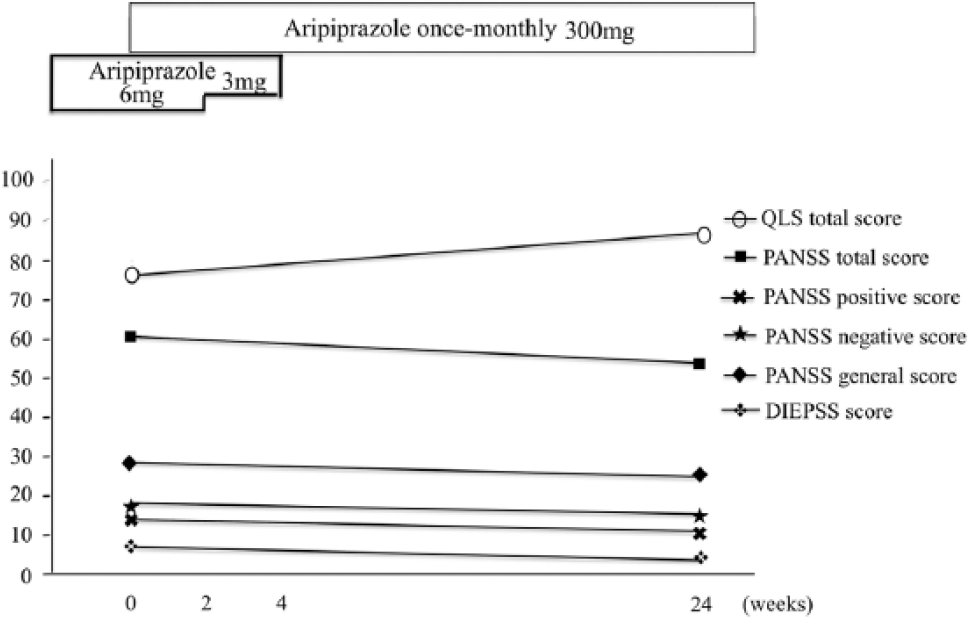
The first outpatient was a 37-year-old woman with paranoid schizophrenia who experienced akathisia and dystonia under aripiprazole treatment (9 mg; Figure 1). AOM 300 was administered and oral aripiprazole was reduced to 6 mg. Oral aripiprazole was reduced to 3 mg after 2 weeks and stopped after 4 weeks. AOM 300 received gluteal injections at 4-week intervals, alternating the left and right sides. 24 weeks after switching from oral low-dose aripiprazole to AOM, the following characteristics improved: PANSS total score (59 to 53), positive score (14 to 13), negative score (18 to 15), general score (27 to 25), QLS total score (86 to 94), and drug-induced extrapyramidal symptoms scale (DIEPSS) 7 (5 to 2) (Figure 1, Table 2). On the other hand, there was no change in the CGI-S (3 to 3).

Patient 1 progress chart.
Change in level of functioning per QLS total and QLS subscale scores from baseline to endpoint.

QLS: Quality-of-Life Scale.
The second outpatient was a 45-year-old woman with paranoid schizophrenia who experienced bradykinesia and akathisia under aripiprazole treatment (6 mg; Figure 2). AOM 300 was administered to oral aripiprazole 6 mg. Oral aripiprazole was reduced to 3 mg after 2 weeks and stopped after 4 weeks. AOM 300 received brachial injections at 4-week intervals, alternating the left and right sides. 24 weeks after switching from oral low-dose aripiprazole to AOM, the following characteristics improved: PANSS total score (60 to 54), positive score (14 to 12), negative score (18 to 15), general score (28 to 27), QLS total score (78 to 86), and DIEPSS (6 to 3) (Figure 1, Table 2). On the other hand, there was no change in the CGI-S (3 to 3).
Patient 2 progress chart.
The third outpatient was a 26-year-old man with paranoid schizophrenia who experienced akathisia under aripiprazole treatment (6 mg; Figure 3). AOM 300 was administered to oral aripiprazole 6 mg. Oral aripiprazole was reduced to 3 mg after 2 weeks and stopped after 4 weeks. AOM 300 received brachial injections at 4-week intervals, alternating the left and right sides. 24 weeks after switching from oral low-dose aripiprazole to AOM, the following characteristics improved: PANSS total score (52 to 47), positive score (11 to 10), negative score (13 to 11), general score (28 to 26), QLS total score (97 to 106), and DIEPSS (4 to 2) (Figure 1, Table 2). On the other hand, there was no change in CGI-S (3 to 3).

Patient 3 progress chart.
Discussion
This is the report of three patients who received aripiprazole in long-acting injectable formulations. In this study, three schizophrenia patients switched from oral low-dose aripiprazole to AOM 300 in order to improve extrapyramidal symptoms (EPS) and negative symptoms to some extent during maintenance therapy. The psychiatric symptoms were stable during therapy, leading to improved QOL and living skills. Consistent with this case report, previous studies have reported AOM 300 was no worsening of mental symptoms or EPS (bradykinesia, akathisia, and dystonia) in the 24 weeks of treatment. 8 Consistent with previous studies, 9 for all three patients, of the four areas of QLS, improvement was seen mainly in intrapsychic foundations. Previous studies reported that depressive and negative symptoms have a significant impact on the QOL of schizophrenia patients. 10 Furthermore, changing to AOM 300 did not exacerbate the depressive and negative symptoms, EPS, common objects and activities and intrapsychic foundation were improved, which may have helped improve the QOL. Therefore, the results suggest the efficacy of AOM 300 in maintenance treatment for schizophrenia when mental symptoms are stable.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.S. has received honoraria from Janssen, Otsuka, Dainippon Sumitomo, Shionogi, and Yoshitomiyakuhin. H.H. has received honoraria from Janssen, Lilly, Otsuka, and GlaxoSmithKline. Y.I. received honoraria from Eisai, Novartis, and Meiji. H.M. has received grant support from Dainippon Sumitomo, Mitsubishi Tanabe, Otsuka, Lilly, Shionogi, and honoraria from Lilly, Novartis, Yoshitomiyakuhin, GlaxoSmithKline, Dainippon Sumitomo, Pfizer, Meiji Seika, Otsuka, Janssen, Shionogi, Eisai, Astellas, and Mitsubishi Tanabe for lectures. K.M. received research supports from Mitsubishi Tanabe, Otsuka, and Shionogi, and honoraria from Otsuka, Mitsubishi Tanabe, and Lilly.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.