
Abstract
Background:
Vision impairment among school-aged children, from uncorrected refractive errors, represents a major public health concern. In Pakistan, organized school-based vision screening programs are limited, and there is insufficient evidence regarding their effectiveness. This study evaluates an optometrist-led, school-based vision screening intervention designed to enhance early detection, awareness, and correction of refractive errors among children in a group of underserved schools in Karachi.
Methods:
A quasi-experimental study was conducted in Azam Basti, Karachi, targeting five low resource schools. Lady health workers received structured training from optometrists to screen visual acuity and detect ocular misalignment in 5–17-year-old students. Students with visual acuity <6/9 and/or obvious ocular pathology were referred for a complete eye exam by an optometrist. The optometrist also delivered education sessions to students. Baseline and 6-month post-intervention surveys assessed changes in knowledge, attitudes, and practices among students.
Results:
A total of 384 students were screened with 72 (18.8%) identified as having refractive visual impairment; they were provided with prescription spectacles free of charge. Astigmatism (9.3%) and myopia (6.3%) were the most common refractive errors. Among primary students (grades 1–5), knowledge and eye health practices improved significantly post intervention (e.g., eye health knowledge: 31.3%–89.8%, p < 0.001). Among secondary students (grades 6–10) similar gains were noted (e.g., basic eye knowledge increased from 27.2% to 84.4% (p < 0.001), and correct eye care habits improved from 46.2% to 99.4% (p < 0.001)).
Conclusions:
Optometrist-led school screenings, including interactive student education combined with standardized lady health worker training to assist with initial screening, effectively enhanced detection and correction of refractive errors while promoting sustainable eye health practices. These findings support the integration of similar programs into school health policies to reduce avoidable childhood visual impairment in underserved urban community schools.
Keywords
Introduction
Vision problems in children represent a significant public health concern globally, particularly in low- and middle-income countries (LMICs), where healthcare infrastructure is often inadequate and access to specialist services limited.1,2 According to the World Health Organization (WHO), ~12.8 million children worldwide suffer from visual impairments (VIs) caused by uncorrected refractive errors, with a disproportionate number residing in LMICs. 3
Children with vision problems may not be able to articulate their symptoms, and parents often lack the awareness to identify such issues at an early stage. VI can lead to developmental delays, limit social development, result in poor academic performance, and reduce economic opportunities.4-6 Moreover, children frequently adopt compensatory behaviors, such as eye strain or sitting too close to screens. 7 A significant barrier to regular eye care in LMICs is the scarcity and urban concentration of eye care professionals. 4 Rural and peri-urban populations face logistical and financial obstacles in accessing timely eye health services. 5 This gap can be successfully addressed over school-based vision screening curriculums led by trained optometrists. According to Opare et al., school-based screenings conducted by eye care specialists have the potential to identify 70% or more of VIs. 1 Basrowi et al. highlighted that early identification of VI through such programs allows timely interventions and helps to prevent long-term complications. 6
Studies from other LMICs, including Nigeria and India, indicate that optometrist-led screenings significantly increase the detection of refractive errors and additional ocular conditions in children.7,8 For example, Morjaria et al. demonstrated that incorporating optometrists in screening programs improves referral accuracy and reduces unnecessary follow-ups. 8 Furthermore, Minnies et al. found that such models contributed to a 35%–50% increase in the detection and correction of VI in targeted regions. 6
Despite this potential, Pakistan lacks large-scale, organized school-based vision screening programs. Data on the prevalence of childhood VI and the effectiveness of screening models remain limited. This study aims to address this gap by implementing and evaluating an optometrist-led vision screening initiative in Azam Basti, a peri-urban locality in Karachi. The program leverages standardized training for lady health workers (LHWs) to screen school children for refractive errors and VI while simultaneously building capacity through awareness sessions conducted by optometrists. Awareness sessions educate children on eye health and the importance of timely intervention. Key outcomes of this study include the prevalence of VI in the targeted schools, the effectiveness of the LHW screening model coupled with an optometrist exam (for students who failed screening criteria), and the benefit of an optometrist awareness program regarding eye health knowledge and health-seeking behavior. This study supports evidence-based recommendations for integrating optometrist-led vision screening programs in underserved urban schools, providing a foundation for sustainable, community-oriented approaches to reducing preventable blindness and improving educational outcomes.
Aim
The aim of this study was to evaluate the effectiveness of an optometrist-led, school-based vision screening, and eye health education program in improving early detection of VIs and enhancing eye health knowledge and practices among school-aged children in underserved schools in Azam Basti, Karachi.
Objectives
To determine the prevalence and types of VIs among students.
To evaluate the effectiveness of an optometrist-led school screening program, assisted by LHWs (trained to screen for VI), in detecting refractive errors and providing timely correction.
To assess changes in students’ eye health knowledge and practices before and after structured educational sessions.
Materials and methods
Study setting
This study was conducted in Azam Basti, a densely populated urban slum placed in District East of Karachi, Pakistan. The community, with an estimated population of ~100,000 residents, comprises low-income families, including daily wage laborers and small business owners. The literacy levels are low, and school enrollment remains limited, with fewer than 40% of school-aged children attending formal schooling due to financial limitations, child labor, and limited parental awareness regarding the importance of education and health.
Azam Basti comprises 26 schools, most of which are low-cost private institutions with limited structure and scarce educational resources. Access to health care is likewise limited, with only a single government dispensary providing basic medical services. The locality was therefore identified as an appropriate setting for a school-based eye health improvement initiative.
Five schools were selected through purposive sampling based on convenience, school population size, and the willingness of school administrations to participate. The study population was clearly defined as school-aged children (5–17 years) enrolled in the selected low-cost private schools in Azam Basti, District East, Karachi.
Study population
Both male and female students from primary (grades 1–5) and secondary (grades 6–10) levels were included. These schools represent a cross-section of the local educational environment and serve as suitable site for implementing and evaluating an optometrist-led vision screening program aimed at early detection and referral of VI.
The total number of children enrolled in the specified grade levels was recorded to estimate the participation rate of the study population.
Study period
The study was conducted over a 1-year period. It is commenced after receiving ethical approval from the Ethics Review Committee of Aga Khan University on April 23, 2024. Baseline assessments were conducted in May 2024. No study activities were carried out during June and July 2024 due to summer vacations.
Study design
A quasi-experimental design was employed. The study utilized pre- and post-intervention assessments without a control group, focusing on measurable changes over time.
Prior to the intervention, a structured questionnaire was administered to assess students’ baseline knowledge, attitudes, and practices (KAP) related to eye health. The questionnaire included items measuring awareness of common vision problems, hygiene behavior, and the perceived importance of regular eye examinations. In addition, baseline vision screenings were conducted to document each student’s initial visual acuity status.
The KAP questionnaire included items on eye knowledge, screen time management, hygiene behaviors, and protective practices, tailored separately for primary (grades 1–5) and secondary students (grades 6–10). Responses were scored as correct or incorrect, and pre- and post-intervention percentages were calculated to measure improvements. Multiple-choice questions were used for most items, with optional open-ended responses counted if matching any correct option. The full questionnaire, including response options with pre and post percentages, is provided as Supplemental Material.
Following completion of these assessments, students attended interactive educational sessions by optometrists, covering topics such as basic eye care, red eye, refractive errors, and preventive measures. A post-intervention evaluation was conducted 6 months later, during which the same questionnaire was re-administered to measure changes in awareness and behaviors. A follow-up visual acuity screening was also performed to identify improvements in visual health and determine whether further referrals required.
This design facilitated a clear comparison of pre- and post-intervention outcomes, enabling an assessment of the intervention effectiveness in enhancing visual acuity, increasing awareness, and promoting positive eye health practices among school-aged children.
Outcomes
The primary outcomes were the prevalence and types of VIs and changes in visual acuity status identified through baseline and 6-month follow-up vision screening. Secondary outcomes included changes in eye health knowledge and practices measured using pre- and post-intervention KAP questionnaires, and identification of students requiring spectacle correction or referral for further eye care.
Sampling strategy
The study employed a universal sampling method, targeting all students enrolled in five local government schools in Azam Basti. Given the aim of including the entire population of students in these schools, a formal sample size calculation was not performed.
Inclusion criteria: All the students aged 5–17 years enrolled in the selected schools with written parental or guardian consent.
Exclusion criteria: Students who did not return consent forms or were absent during baseline assessments.
Screening procedures
Screening procedures were conducted by two LHWs who received standardized training delivered by an optometrist. The training began with an instructional session on common childhood eye conditions, followed by hands-on demonstration on conducting vision screening. LHWs were trained to measure visual acuity using the Snellen chart at 6 m and accurately document findings. They were also taught to perform a basic torchlight examination and identify signs of ocular misalignment including strabismus. To ensure competency, each LHW was required to examine 20 students under optometrist supervision before being authorized to conduct screenings independently. Once trained, the LHWs screened students for visual acuity and ocular misalignment. Students presenting visual acuity worse than 6/9 in either eye as measured using the alphabet-based Snellen chart with optotypes increasing from a single-letter 6/60 line to six letters on the 6/6 line were referred to the optometrist for a comprehensive examination, including cycloplegic refraction, squint assessment, and anterior segment examination. Cycloplegic refraction was performed using Cyclogel 1% (cyclopentolate hydrochloride). One drop was instilled in each eye, and after 15 min, a second drop was administered if adequate cycloplegia was not achieved, taking into account iris pigmentation. Refraction was conducted in a darkened room once full cycloplegia was confirmed. Objective refraction was performed using retinoscopy, followed by post-mydriatic subjective refraction 1–2 days later, and final spectacle prescriptions were based on these cycloplegic refraction measurements. Those diagnosed with refractive errors were provided prescription eyeglasses at no cost; however, students requiring further assessment or surgery were referred to nearby designated eye care services.
Educational component
As part of the intervention, an optometrist conducted educational sessions for students, focusing essential eye health knowledge and practical habits for maintaining good vision. Sessions were conducted in every class and during four consecutive weekly school assemblies after baseline assessments. The sessions covered key topics including the importance of regular vision screening, appropriate lighting while reading or studying, maintaining safe viewing distance from screens, and recognizing early signs of visual problems. Interactive activities and visual aids were incorporated to enhance student engagement and support effective learning. Students were encouraged to adopt these healthy practices in their daily routines and to share the information through their families and peers. The objective was not only to increase immediate awareness but also to faster long-term behavioral improvements ensuring that positive eye health practices would continue beyond the duration of the program.
Operational definitions
Normal vision was defined as visual acuity of 6/9 or better in each eye, measured using a Snellen chart at 6 m. VI was defined as visual acuity worse than 6/9 in either eye and/or the presence of a refractive error or ocular misalignment requiring referral. Refractive errors, based on cycloplegic refraction, included one or both eyes with myopia (defined as a spherical equivalent of ⩽−0.50 diopters), hypermetropia (defined as a spherical equivalent of ⩾+0.50 diopters), and astigmatism (defined as a cylinder power of ⩾±0.50 diopters). Eye alignment was categorized as orthophoria (no ocular deviation), esotropia (inward deviation of one or both eyes), exotropia (outward deviation of one or both eyes), and convergence insufficiency (reduced ability to maintain binocular convergence at near fixation). Primary students were children enrolled in grades 1–5, and secondary students were those enrolled in grades 6–10. Completed follow-up referred to students who completed both baseline and 6-month post-intervention screening and questionnaire assessments. Knowledge and practices were measured as composite scores derived from questionnaire responses.
While AAPOS recommends higher thresholds for amblyopia risk (hypermetropia ⩾+4.0 D, anisometropia ⩾1.25 D), this study used lower cut-offs (+0.50 D for hypermetropia and ⩾±0.50 D for astigmatism) to estimate refractive error prevalence across all age groups. Similar thresholds have been applied in population-based studies to capture mild errors that may affect visual development, ensuring uniform definitions and comprehensive reporting. 9
Ethical considerations
The study was approved by the Ethics Review Committee of the Aga Khan University (ref: 2024-8505-28790), and written informed consent was obtained from legally authorized representatives of all the participating students and parents or guardians.
Data collection and analysis
Data on VIs and the prevalence of ocular conditions were systematically collected through structured screenings conducted by LHWs using standardized forms. Students that failed the screening exam (vision worse than 6/9 and/or obvious ocular misalignment) were examined by an optometrist (S.J.). Records of visual acuity and the diagnosis of refractive errors or other ocular conditions were documented during the initial screenings, and complete ocular examination. These examinations included cycloplegic refraction, squint assessment, and anterior segment evaluation using appropriate ophthalmic instruments. To assess the effect of the intervention, a baseline assessment was conducted prior to the educational sessions, followed by a repeat assessment 6 months post intervention.
Key domains included awareness and adoption of accurate eye care behaviors, such as correct eye hygiene practices, the use of sunglasses for ultraviolet protection, adherence to regular eye examinations, early recognition of symptoms such as redness or pain, avoiding overcrowded environment to reduce infection risk, avoiding eye rubbing to prevent irritation and injury, and wearing protecting sunglasses when needed. Primary and secondary students were included to facilitate a comparative assessment of the intervention’s effectiveness across age groups.
Data were analyzed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize demographic characteristics and questionnaire responses. Paired t-test was applied to compare pre- and post-intervention scores on knowledge and practices; chi-square tests measured association between categorical variables and intervention outcomes. The significance was set at p < 0.05.
Results
Demographic characteristics
A total of 384 students from the five participating schools were screened in this study. All the students enrolled in grades 1–10 at these schools were invited to participate. The mean age was 9.1 years (range 5–15 years), with 43.8% (n = 168) female and 56.2% (n = 216) male students. Both primary (from grades 1 to 5) and secondary (from grades 6 to 10) levels were included in the demographic profile (Figure 1). The demographic distribution of the screened students is presented in Table 1.

Flowchart of vision screening and outcomes in school-aged children (grades 1–10).
Demographic of screened students.

VI and eye conditions
Of the 384 students screened, 72 (18.8%) were diagnosed with visual problems, while 312 (81.2%) had normal vision. All the children requiring correction received spectacles. Among those with refractive errors, myopia accounted for 24 (6.3%), hypermetropia for 12 (3.12%), and astigmatism for 36 cases (9.4%). Eye alignment testing revealed orthophoria in 93%, esotropia in 2.9%, exotropia in 2.1%, and convergence insufficiency in 2.1 (Tables 2 and 3). All the refractive errors were measured under cycloplegia using 1% Cyclogel (cyclopentolate) and retinoscopy.
Vision impairment among children from five school sites.

Age-stratified visual impairment and refractive error.

Gender differences in refractive errors
Refractive errors were more common among girls versus boys across all age groups (Table 4). Of the 72 children with refractive errors, 66.7% were girls and 33.3% were boys (Figure 2). Although girls consistently showed higher proportions of refractive errors, these differences were not statistically significant. Using visual acuity as the primary screening criterion, amblyopia was defined as best-corrected visual acuity worse than 6/12 in either eye in the absence of observable ocular pathology. Based on this definition, no students met the criteria for suspected amblyopia.
Gender-stratified distribution of refractive errors.

p values were calculated using the chi-square test to compare proportions between boys and girls.

Children identified with visual problems (n = 72) who received prescription spectacles following optometrist evaluation.
Knowledge and practice improvements
Group 1: Primary students (grades 1–5)
Among the 147 primary students (mean age 6.0 years; 42% female), significant improvements were observed across all domains of eye health knowledge and practices following the intervention (Figure 3(a)). Exact practices for handling screen time increased from 36.1% to 95.2%; however, proper use of sunglasses improved from 15.0% to 89.1%. Awareness related to healthy food, hand hygiene, and infection prevention likewise improved significantly (Table 5).

Comparison of pre- and post-intervention eye health knowledge and practices among (a) primary students (grades 1–5) and (b) secondary students (grades 6–10), showing significant improvements across all domains.
Summary of ocular hygiene and health survey for group 1 (primary students).

p values were calculated using McNemar’s test to compare pre- and post-intervention responses for the same students.
Group 2: Secondary students (grades 6–10)
In the secondary group (n = 173, mean age 11.3 years; 65% female), post-intervention (Figure 3(b)) assessments also demonstrated highly significant gains. Basic eye knowledge rose from 27.2% to 84.4%, recognition of eye problems from 28.9% to 94.8%, and correct eye care habits from 46.2% to 99.4%. Improvements were also observed in adherence to regular eye examinations, identification of eye symptoms, and protective behaviors (Table 6).
Summary of results from ocular hygiene and health survey for group 2 (secondary students).
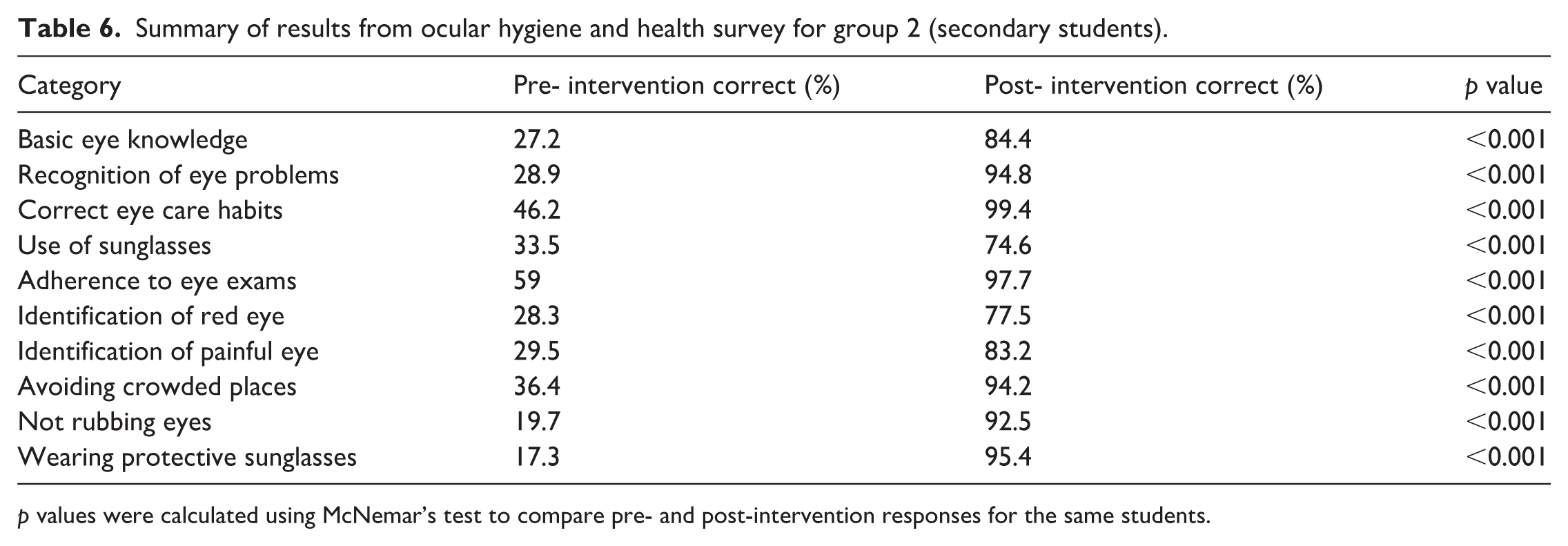
p values were calculated using McNemar’s test to compare pre- and post-intervention responses for the same students.
Discussion
This study highlights the prevalence of VIs among primary and secondary school-aged children in an underserved urban population within Karachi, Pakistan, with 18.8% needing corrective correction. Based on an educational intervention, we also noted significant improvement in children’s knowledge and practices related to eye health. These outcomes highlight the need for regular vision screening as well as eye health education in schools, especially in underserved areas.
Hypermetropia in our study showed a slight increase with age, likely reflecting persistent, clinically significant hyperopia, as physiological hyperopia common in younger children was not included. Myopia prevalence also tended to increase with age, consistent with expected age-related patterns. These findings align with population studies showing that low-grade hyperopia declines with age due to emmetropization, while persistent hyperopia and myopia remain detectable in school-aged children. 10
When compared internationally, our observed prevalence (18.8%) is broadly comparable to estimates reported in other LMICs, where the prevalence of refractive errors among school-aged children typically ranges from 10% to 25%,11,12 for example, studies from India and Nepal have reported prevalence rates of ~13%–22%,13–15 while reports from parts of sub-Saharan Africa show lower but variable rates (5%–15%).16,17 In contrast, higher prevalence has been documented in East Asian countries such as China and South Korea, where school-based studies frequently report refractive error prevalence exceeding 30%–40%, largely driven by high rates of myopia in urban populations.18,19 The higher prevalence of refractive errors among girls compared to boys supports previous research shown in Pakistan and other LMICs.19–22 Similar studies in India 22 reported that girls were more likely to present with untreated refractive errors. Although our study used lower cut-offs for hypermetropia and astigmatism, the AAPOS guidelines recommend considering hypermetropia ⩾+4.0 D, anisometropia ⩾1.25 D, and significant myopia or astigmatism as clinically relevant risk factors for amblyopia in children aged 5–7 years. Using uniform lower thresholds allowed us to standardize screening across all age groups, but the true risk for amblyopia in younger children may be limited to higher refractive errors.
In Pakistan, school-based vision screening programs have been implemented intermittently with outcomes affected by inconsistent protocols, limited resources, and inadequate coordination across educational and health sectors, often with varying degrees of success.20–22 The lack of standardized protocols and limited resources often hinder the scalability of these programs. Globally, school-based eye health programs are recognized as a best practice for improving visual health in children. 23 The WHO recommends integrating vision screening into school health services as part of a broader strategy to combat childhood blindness and VI. In high-income countries, such as the United States 24 and the United Kingdom, 25 school vision screening takes place regularly in order to detect vision impairment and refer for early intervention.
Our intervention aligns with global best practices 23 including multiple components such as screening (assisted with LHWs), corrective measures, education, and teacher training.
Earlier research has shown that taking ownership of one’s own health is associated with improved understanding and better adherence to treatment.24,25 An important element of our intervention was empowering children to take responsibility for their health by promoting a sense of responsibility and increasing health awareness among students. This empowerment spreads outside the school, as students can share their knowledge with their families promoting a wider culture of health awareness within the community. Although not assessed formally, involving families likely strengthens the information provided at school and strengthens support at home.
The participation of the school administration and local community provided valuable support and was instrumental in achieving the objectives of the program. The sustainability of community-based health interventions is vital,26,27 as it fosters a sense of responsibility and ownership among stakeholders. Through the engagement of local stakeholders and the integration of eye health education into the school curriculum, the initiative helped establish a foundation for an accessible and sustained program. This community-centered approach ensures that the benefits of the intervention extend beyond the immediate participants, making a supportive environment for ongoing health improvements.
This study has several implications for practice and policy in Pakistan and other LMICs. Firstly, it shows the efficacy and feasibility of an optometrist-led school-based eye health program in addressing VIs and improving children eye health knowledge. Secondly, empowering LHWs to identify the signs of VI and refer students appropriately will help sustain this program. If LHWs are not available, one can consider training school nurses and/or teachers to do the initial screening.
Our post-intervention results show significant improvement in eye health knowledge and practices among students demonstrating the efficacy of incorporating eye health education into the school curriculum. This approach not only addresses current VIs but also supports long-term eye health and the prevention of future problems. Policymakers should consider integrating regular vision screenings with eye health education into national education policies to ensure complete coverage.
This study has several limitations. First, purposive sampling of schools from underprivileged areas may introduce selection bias and limit generalizability. Second, the KAP questionnaire used to assess eye health knowledge and practices was not formally validated or pilot-tested, which may affect measurement precision. Finally, the absence of a control group limits the ability to attribute observed changes solely to the intervention.
Future research should focus on conducting similar studies in other underserved regions to test generalizability. Longitudinal studies can also be conducted to assess impact of school-based eye health programs on academic performance and quality of life. Furthermore, exploring innovative methods such as mobile health applications for vision screening and follow-up care might improve program reach and effectiveness. Collaborating with government and international civil society organizations and leveraging global best practices can support local efforts and help ensure such program are sustainable and accessible.
Conclusion
This initiative demonstrates that an optometrist-led multifaceted vision screening program advances child eye health within underserved urban school communities of Karachi. The program included standardized training of LHWs, who screened students and referred those needing further care to an optometrist. An optometrist then performed a complete eye exam and prescribed glasses as needed. The optometrist also delivered eye health education which resulted in significantly improved knowledge and eye health practices among students. This comprehensive approach addressed immediate visual health requirements while encouraging sustainable improvements through education and capacity building. This multidimensional strategy is essential for creating long-term change, as supported by similar successful programs in other LMICs such as Nepal. 28 Although the study faced certain limitations such as the absence of a control group, short follow-up duration, and restricted geographic scope, its outcomes serve as a promising model for further validation and adoption, particularly among underserved urban schools.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261429666 – Supplemental material for Optometrist-led vision screening: Enhancing child eye health in underserved district schools within Karachi
Supplemental material, sj-docx-1-smo-10.1177_20503121261429666 for Optometrist-led vision screening: Enhancing child eye health in underserved district schools within Karachi by Saima Jamil, Hamza Inayat, Sana Hyat and Karim F. Damji in SAGE Open Medicine
Footnotes
Acknowledgements
The authors sincerely thank the school administrations, teachers, and students of the participating schools, as well as the lady health workers (LHWs), for their cooperation and support throughout the study. We also acknowledge the Department of Community Health and Dr. Sameen Siddiqui for initiating programs that facilitated this study, and the Department of Ophthalmology and Visual Sciences for providing manpower, optometric equipment, and necessary eye drops. This study was a collaborative effort, and the authors express their gratitude to all the stakeholders.
Author contributions
Saima Jamil drafted the complete article, including methodology and data compilation. Dr. Sana Hyat (principal investigator) designed and supervised the study, coordinated logistics, and oversaw all the study procedures. Dr. Karim F. Damji provided senior guidance, reviewed the article, and assisted in addressing reviewer comments. Hamza Inayat drafted the discussion section and contributed to integrating study findings with relevant literature.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received no financial support for the research, authorship, and/or publication of this article. All resources, including manpower and materials, were provided through institutional support from the Department of Community Health and Department of Ophthalmology and Visual Sciences, Aga Khan University Hospital.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.