
Abstract
Objective:
There is a need for contraception uptake among people to enable them to fulfil their right to determine the timing, number and spacing of their children. In regions with poor contraceptive prevalence rates, lack of effective education has been largely implicated, and Nigeria falls among such regions. Thus, the present study is designed to examine the impact of an educational intervention on uptake of contraceptives among women aged 18–49 years seeking care at the Nnamdi Azikiwe University Teaching Hospital Nnewi.
Methods:
Being an interventional study to underscore the effect of targeted health education on uptake of contraceptives, a randomized controlled trials design was adopted. A total of 275 women were randomly recruited and allocated into two groups—140 in intervention group and 135 in the control group. Data was collected by trained research assistants using a pretested structured interviewer-administered questionnaire and analyzed using Statistical Package for Social Sciences version 25. The level of significance was set at p < 0.05.
Results:
At baseline, the level of uptake of contraceptives was similar in both the control and the intervention group (control = 2.48 points; intervention = 2.55 points). Overall, there were no statistically discernible differences between the two groups at baseline. The level of awareness and knowledge on contraceptives as well as the uptake of contraceptives significantly increased in both groups at the end of the study period. A statistically significantly higher increase was noted in the intervention group when compared to the control in level of awareness (t = 3.235; p < 0.05) and uptake of contraceptives (t = 2.628; p < 0.05). Significant positive changes in perceptions of contraceptives were observed more among the intervention group when compared to the control. Logistic regression analysis showed uptake of contraceptives was significantly influenced by occupation, monthly income, source of information, time of first use of contraceptives, level of knowledge on contraceptives as well as the targeted educational intervention.
Conclusion:
The targeted health educational intervention had a significant and positive effect on the level of awareness and uptake of contraceptives, as displayed in the intervention group. A significant and positive change in perception of contraceptives was also noted among the intervention group in almost all the questions. Certain factors were found to significantly impact the uptake of contraceptives. There is a need for studies with longer follow-up to ascertain sustained impact of health education on uptake of contraceptives. Further studies should be carried out in the other facilities in Nnewi to ensure a better coverage and representation of the target population. Finally, related studies should be carried out among men.
Introduction
Improving child and maternal health is emphasized in Goal 3 of the Sustainable Development Goals (SDGs) as key targets. 1 Of the many factors that influence child and maternal health, the uptake of contraceptives is rated highly, resulting in several countries measuring the prevalence of contraceptive use among their reproductive population. 2 The uptake of contraceptives has been adopted in family planning, which refers to a couple’s conscious effort to limit or space the birth of their children or completely avoid conceiving children.3,4 Contraceptives are grouped into two, traditional (i.e., rhythm method, withdrawal, fertility awareness-based methods, the lactational amenorrhea method and folk methods) and modern contraceptives (male and female condoms, diaphragm, cervical cap and sponge, hormonal contraceptives such as oral, injectable, transdermal and vaginal ring and implants, intrauterine device). Family planning programs usually promote the use of modern methods rather than traditional methods, as the latter have a higher failure rate. The latter is true, even in Nigeria. 5
Of the top-10 countries with high and reasonable Contraceptive Prevalence Rate (CPR)—defined as having the proportion of women who are currently using or whose sexual partner is currently using any contraceptive regardless of method (modern or traditional) being used as 80% or above—no African country is listed. However, countries like South Africa, Kenya, and Algeria have surpassed 50% CPR, with potential and sustained increase into the future. 6 In Nigeria, there was a benchmark of achieving 36% CPR by 2018, which is yet to be achieved even in 2021. 7 Statistics on CPR from Africa suggest that few African countries are within the 75% CPR global benchmark as specified by the SDGs for 2030. 8 Knowledge and awareness about contraceptives contribute to high performing CPR.5,7,9 Targets for health education on contraception are focused on improving knowledge and utilization of modern contraceptives, while reducing traditional methods of contraception.10,11 Sources of information on contraceptives include Antenatal care Clinics (ANC), media, peers, parents, and patent medicines vendors, among others. 12 A typical example of a program on contraception in Nigeria is The Nigeria Urban Reproductive Health Initiative (NURHI), which aimed to eliminate supply and demand barriers to contraceptive use and make family planning a social norm in Nigeria. NURHI employed a Distance Education tool (iDEA) to provide a platform from which providers can access relevant educational content and resources from Android-based smartphones or tablets. 13 An evaluation of NUHRI by Onwujekwu et al. 14 reports that in the six cities of Nigeria (Ilorin, Benin, Kaduna, Ibadan, Abuja, and Zaria) where NURHI was operational, there were reported improvements in CPR. Notably, this pattern of education has some level of limitation to assessing the materials and learning actively as its direct impact on various target populations may not be satisfactorily ascertained. Targeted education, on the other hand, attempts to deliver well-structured information on contraceptive use to a select population with the goal of increasing their knowledge of contraceptives and their uptake. A study by Abdulrazaq showed that the intervention group had a significant increase in CPR from 11.8% at baseline to 22.4% postintervention among married military barrack women in Northern Nigeria following a 50-min health talk and family planning methods demonstration. 10 There has not been any report on the effect of targeted education on the uptake of contraceptives among women in Nnewi Anambra state.12,15,16 This study aims to investigate the effect of targeted health education on uptake of contraceptives amongst women seeking care in Nnamdi Azikiwe University Teaching Hospital (NAUTH) Nnewi, Anambra, South-East Nigeria.
Method
Study setting
The study was done at the NAUTH in Nnewi, Anambra State with ethical approval obtained from NAUTH Health Research Ethics Committee (NAUTHHREC); NAUTH/CS/66/VOL.15/VER.3/102/2022/041. Nnewi is the second largest commercial town in Anambra with a total population of 224,554 out of which 110,701 (49.3%) constitute women of reproductive age. 17 Nnewi is located east of the Niger River and 22 km South-East of Onitsha in Anambra State of Nigeria with land mass area dimension of over 200 m2. A 2015 study found poor uptake of contraceptives in NAUTH, and further blamed it on weak health education. 15 It is for this reason that the study was undertaken in NAUTH. Notably, the facility has 14 departments and 3 units (NAUTH, 2021). Of the departments, two are concerned with reproductive health, which are (a) Community Medicine and Primary Healthcare Department and (b) Comprehensive Health Centre. The latter two departments formed the focus of this study.
Study design
This is an interventional study to underscore the effects of targeted health education on the uptake of contraceptives among women of reproductive age (18–49 years) in NAUTH, the city of Nnewi, Nigeria. To achieve this, the study adopted randomized controlled trials (RCT) design, which enabled us to prospectively measure effectiveness of a new intervention or treatment while controlling for confounders, serving as a rigorous tool to examine cause-effect relationships between an intervention and outcome. 16 The duration of this study was from February 2021 to September 2022.
Study population
As of the last revision of census figures in Nigeria, both Nnewi local governments have a combined population of 224,554 out of which 110,701 constitute women of reproductive age (18–49 years). 17 Intuitively, since NAUTH with an extension of primary healthcare services remains the only tertiary health institution in the study location, a reasonable number of women of reproductive age should be making use of the facility. Thus, the study population was the 110,701 women who were within reproductive ages (18–49 years) in Nnewi. This suffices for an absence of published figures on reproductive-aged women using the services of NAUTH.
Inclusion and exclusion criteria for the study
The focus of this study was on women of reproductive age (18–49 years) who were sexually active and accessed healthcare at NAUTH Nnewi between February 2021 and August 2022 and voluntarily consented to participate in the research. Alternatively, those who were non-residents of Nnewi Anambra State or were within the ages of 18–49 years but critically unwell were not qualified for inclusion, even if they utilized health services in NAUTH. Finally, those who declined participation in the study were excluded with no consequences for non-participation.
Sample size determination
The sample was derived from the 110,701 women who are of reproductive age in Nnewi. 17 To determine the sample size, the researcher adopted the RCTs formula proposed by Chan 18 for comparison of two proportions (two-sided) using proportion estimates π1 = 0.3 and π2 = 0.5 units respectively at 5% level of significance and constant (C) = 10.5 for 90% power, a target sample size was calculated to be 125 participants per group (Intervention and Control). Assuming an attrition rate of 10%, a total sample size of 275 participants was realized.
Sampling and recruitment
A probability random sampling method was preferred as it aided the researcher generate data that was representative of the target population as well as control for selection bias during the sampling. 19 Specifically, simple random sampling was carried out at the NAUTH, Nnewi facility. A list of all adult reproductive-aged women who attended clinical health-related services at two departments, namely: (a) Community Medicine and Primary health care Department and (b) Comprehensive Healthcare Department in NAUTH, Nnewi during study time was secured. To ensure that everyone on the list got a fair chance to participate in the study, the researcher tied numerical identity to each of the names on the list, following the chronological order they appear. The numerical identity was written on some tiny pieces of paper starting with one (1) corresponding to the first name on the list until the required sample of 275 was arrived at. These tiny pieces of paper were folded and thrown into a box. Next, a simple random sampling technique by balloting and hand-drawing methods was used to pick numbers from the box. Anyone picked was traced to the exact name and contact on the list, and the person invited to participate in the study. In the event of decline or someone who met the exclusion criteria of the study, the next person on the list was selected until the required sample of 275 participants realized.
Randomization
In order to prevent selection bias and confounding, simple randomization technique was employed to produce comparable groups. Each of the eligible participants was given an equal chance to be allocated to the intervention group or the control group. A list of the sampled 275 participants was made by the research assistants and numbered serially. Thus, to make sure the data were collected without biases the research assistants (1 nurse and 1 physician) randomly allocated the participants to either the control or intervention groups using the list of the sampled 275 women. A box containing pieces of paper, each labeled either intervention or control, was used during the allocation. Two hundred eighty pieces of paper were put in the box—140 labeled intervention group, 140 labeled control group. A piece of paper was then picked randomly each time by hand drawing. The outcome of the first picking was marked on the first name on the list. Similarly, the outcome of the second picking was marked on the second name on the list, and so on. In this way, participants were randomly assigned to either the control or intervention group. An allocation list which contained the names and corresponding study groups was therefore developed. This ensured maintenance of balance between the intervention group and control group so that the numbers were not too dissimilar. At the end, there were 135 participants in the control group and 140 participants in the intervention group. Participants were asked not to discuss the details of their intervention with other study participants.
Intervention
The researcher designed an educative intervention on contraception, drawing from his experience as a medical practitioner and reliance on a 2014 study by Abdulrazaq. 10 The intervention group participated in a 60-min oral education on contraceptive basal knowledge and method’s demonstration 3 days per week for a duration of three consecutive weeks. This educational intervention was done alongside one of the health workers in the facility and focused on the various types of modern contraception, their advantages and disadvantages inclusive of side effects, and how effective certain contraceptives can be against STDs. Furthermore, how each contraceptive was used was also taught. Importantly, time was created to entertain conversations on the perceived barriers the targeted women face in a bid to uptake contraception. Room was granted for a question-and-answer session. The intervention was delivered in a large conference room at the hospital. All the women were assumed to have a similar level of knowledge at baseline (preintervention). The effect of the intervention received by one group on contraceptive knowledge and uptake was then assessed. The control group did not participate in the educational intervention throughout the period of the study. The control group participated in the usual health counselling sessions organized by the hospital to enlighten women on health-related issues.
Data collection procedures
A pretested structured interviewer-administered questionnaire was used to collect quantitative data. The questions were organized into two parts—the preintervention and postintervention parts. The questionnaire was developed following review of relevant literature related to the current study.4,7,20 To validate the research instruments, the researcher conducted a pretest with 28 women of reproductive age (representing 10% of the sample size) who accessed health services at Holy Rosary Specialist Hospital and Maternity Onitsha. The outcome of the test-retest analysis to assess the reliability of the instrument showed that the instrument was highly reliable (Cohen’s kappa (k) = 0.894). The instrument was additionally reviewed by three experts in community health, public health, and health policy for their comments. Their suggestions were incorporated to further refine the instrument. The questions in the questionnaire captured the sociodemographic factors of the respondents, as well as their perceptions and scale of uptake of contraceptives and knowledge. Informing the construction of questions were findings from literature review and the objectives of the present study.
To ensure quality data collection, research assistants were trained in questionnaire administration and data collection procedures. They were conversant with both English and Igbo languages in order to enable proper interpretation of the study instrument. Data was collected by the research assistants from the study participants at baseline and 2 weeks after completing the targeted educational intervention via interviewer-administered questionnaires.
The decision to assess study participants 2 weeks after exposure to the educational intervention was based on the reliance that this represents a sufficient interval for study participants to imbibe lessons from the oral educational intervention and make a decision regarding whether or not to take up contraceptives. The study ran between July and September 2022.
Study measurements
Outcome variable: The main outcome/dependent variable for this study was uptake of contraceptives (defined as use of any contraceptive method, including condoms, injectables, intrauterine devices, Implanon and surgical methods) among women who sought care at NAUTH Nnewi.
Independent variable: The other variables were the level of awareness, knowledge and perception of contraceptives and their use. The sociodemographic variables assessed were age, level of education, marital status, religion, occupation, monthly income and number of children.
The levels of awareness, knowledge and uptake of contraceptives were examined by asking the participants to rate the latter based on a 6-point rating scale (scored 1–6 representing none to very high). Scores from 1–2 were classified as low; scores 3–4 were classified as moderate; while scores 5–6 were classified as high. Questions based on a 5-point Likert scale were used to assess participants’ perception of contraceptives. Scores ranged from 1 to 5 (from strongly disagree to strongly agree).
Statistical analysis
Data was analyzed using IBM Statistical Package for Social Sciences (SPSS) Version 25. Responses were coded and entered into the software. Before analysis, the entered data was checked for errors and made clean. Statistical tools like means and standard deviation, percentage and frequency distribution, Fisher’s Exact test, and t-test were used to present the data, test the significance of the relationships between the independent and dependent variables, and to compare mean values of some variables, respectively with the level of significance was set at p < 0.05. Multinomial logistic regression was performed to determine the factors that influenced the uptake of contraceptives; odds ratios were presented with 95% confidence level.
Ethical consideration
Ethical clearance was obtained from Nnamdi Azikiwe University Teaching Hospital Health Research Ethics Committee (NAUTHHREC); NAUTH/CS/66/VOL.15/VER.3/102/2022/041 and Kenyatta University ethics review committee (KUERC). A written consent was obtained from each participant before commencement of interview and collection of data. Participants were assured that every information given would be treated with utmost confidentiality. Trial registration was at Pan African Clinical Trials Registry (pactr.samrc.ac.za); (PACTR202306677547495) (Figure 1).

Flow diagram of participants throughout the research.
Result
The age of the studied population ranged from 18 to 49 years with mean age determined as 31.20 ± 7.03 years (Table 1). As shown in Table 1, the distribution of respondents was similar in both the intervention and control groups studied. Majority aged between 18 and 30 years both in the intervention and control groups (50% and 51.9%, respectively). In both groups, majority had High school as highest level of education—57.1% for intervention group and 55.6% for control group. Most of the participants were civil servants (44.3% intervention group and 40.0% control group). A higher percentage earned below $72 (57.1% intervention group and 61% control group). Majority in both groups were married (73.6% intervention group and 70.4% control group). It was seen that 70.7% of the intervention group and 71.1% of the control group lived with their spouses. Most were Christians of Catholic denomination (intervention group—54.3% and control group—56.3%) (Table 1). Some of the women have given birth. The number of children ranged from 0 to 7 with mean calculated as 2.25 ± 2.02 children (Table 1).
Sociodemographic characteristics of respondents.

FSLC: first school leaving certificate; SSCE: senior school certificate examination; OND: ordinary national diploma; HND: higher national diploma.
In Table 2, result showed that awareness and knowledge of contraceptives, and the uptake of contraceptives significantly increased in both the control and intervention groups when post-interventional scores were compared with pre-interventional scores (p < 0.05 in all cases). However, a higher increase in awareness, knowledge, and the uptake of contraceptives was seen in the intervention group. In the intervention group, perception of contraceptives showed the highest increase (pre-intervention = 2.55; post-intervention = 4.01; t = 8.133; p < 0.05).
Effect of educational intervention on awareness, knowledge, and uptake of contraceptives.
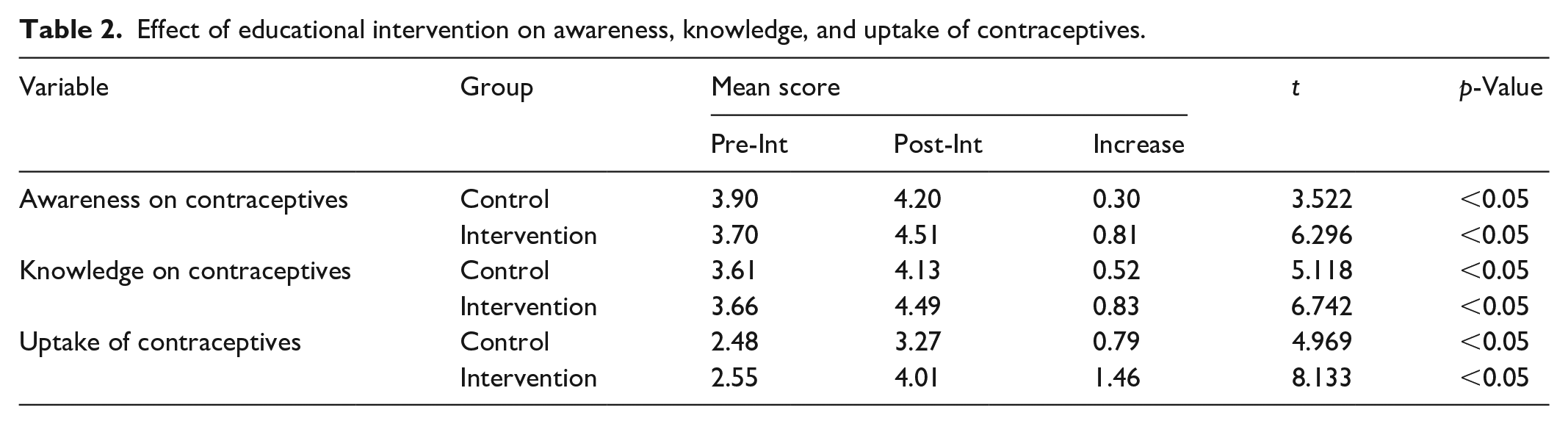
As shown in Table 3, a statistically significant higher increase in level of awareness (t = 3.235; p < 0.05) and uptake of contraceptives (t = 2.628; p < 0.05) was found in the intervention group when compared to the control group. The increase in knowledge on contraceptives did not show any statistically significant difference between the two study groups (t = 1.485; p > 0.05).
Comparison of increase in score between the control and intervention groups after the targeted educational intervention.

Results showing the effect of the targeted educational intervention on perception of contraceptives is presented in Table 4. A significant positive change in perception of contraceptives was found among the intervention group in almost all (80%) of the questions used to assess perception. In contrast, the control group showed significant positive changes in only 20% of the questions.
Effect of educational intervention on perception of contraceptives.

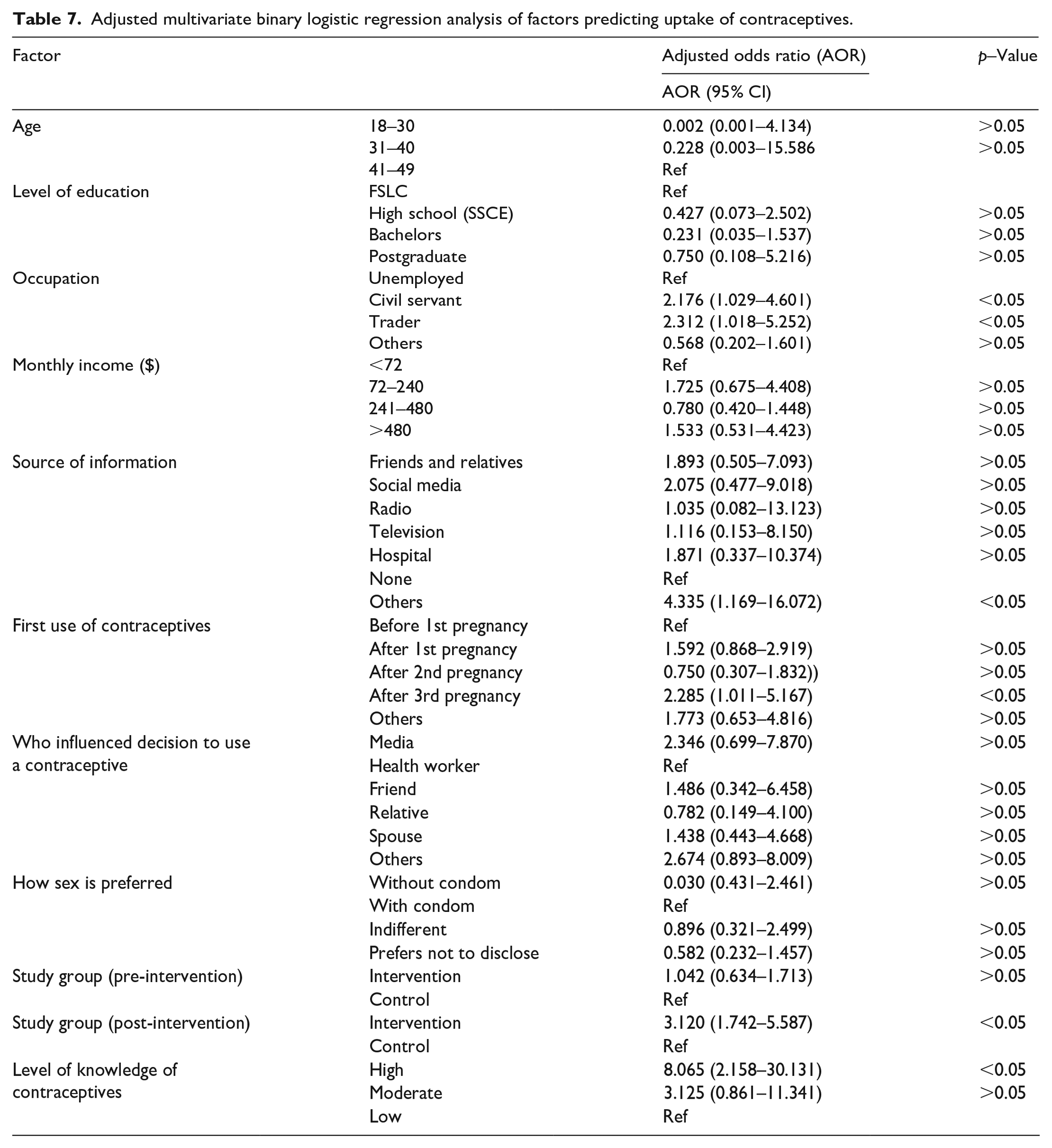
In Tables 5–7, the results of regression analysis on factors influencing uptake of contraceptives are presented. Multivariate binary regression analysis was performed to determine adjusted odds ratio values at 95% confidence interval. The following factors had a significant influence on uptake of contraceptives: occupation, monthly income, source of information, first use of contraceptives, and level of knowledge of contraceptives. Respondents who were civil servants (aOR = 2.176; 95% CI: 1.029–4.601; p < 0.05) and traders (aOR = 2.312; 95% CI: 1.018–5.252; p < 0.05) were more unlikely to take up contraceptives compared to those who were unemployed. Those who sourced information on contraceptives from other sources not listed were more likely to take up contraceptives than those who had no source (aOR = 4.335; 95% CI: 1.169–16.072; p < 0.05). Uptake of contraceptives was also more likely to occur amongst participants who used contraceptives after third pregnancy compared to those who used contraceptives first before first pregnancy (aOR = 2.285; 95% CI: 1.011–5.167; p < 0.05). Similarly, uptake of contraceptives was also more likely to occur among respondents who had high level of knowledge than those who had low knowledge level (aOR = 8.065; 95% CI: 2.158–30.131; p < 0.05). Other factors as outlined in the table showed no significant influence on uptake of contraceptives (p > 0.05 in these cases).
Adjusted multivariate binary logistic regression analysis of factors predicting uptake of contraceptives among the control group.

Adjusted multivariate binary logistic regression analysis of factors predicting uptake of contraceptives among the intervention group.

Adjusted multivariate binary logistic regression analysis of factors predicting uptake of contraceptives.
Discussion
This study aimed to determine the effect of a targeted educational intervention on the uptake of contraceptives among women seeking care at NAUTH Nnewi. A RCTs design was used in this study, and participants were allocated into either of two study groups—intervention and control. At the end of the intervention, a significant improvement was seen in the level of awareness and knowledge of contraceptives. Also, uptake of contraceptives increased. However, the extent of improvement in awareness, knowledge, and uptake of contraceptives was higher in the intervention group when compared to the control group. In the intervention group, remarkable positive changes in perception of contraceptives were seen.
Educational interventions have been shown to be effective in addressing public health concerns, such as uptake of contraceptives. Our findings on the effect of targeted education on knowledge agree with a study by Abdulrazaq et al., 10 which showed that the intervention group had a 7.8 post-intervention mean knowledge score from 5.5 before the intervention. In addition, while CPR increased for the intervention group from 11.8% at baseline to 22.4% post-intervention, the control group showed no significant change. This means that uptake of contraceptives among women of childbearing age would increase when they pay attention to education on contraception, especially as it concerns their health and well-being. Similar studies by Ajayi et al. 3 and Babalola et al. 9 advocated for client-centered contraception education, which can be either done virtually, physically or through drama. In a study by Takagi et al., 21 it was reported that educational intervention led to increases in attitude and knowledge regarding vaccines and was said to be a useful approach in increasing vaccination acceptance. Similarly, uptake of contraceptives would increase when the knowledge level of the population is improved through targeted education and exposure. In a systematic review by Pazol et al., 22 a wide range of mediums are effective at increasing knowledge. The most effective of them was use of simplest presentation of numeric information and simpler materials paired with interactive questions from a healthcare provider. Research from other areas of healthcare suggests that using plain language, 23 attending to the client’s cultural and linguistic preferences, limiting the amount of presented information and discussing important facts first, 24 and simplifying the presentation of numeric quantities 25 are important for promoting client comprehension. More detailed research specific to these topics is needed in relation to contraception.
Following the educational intervention, significant changes in perception of contraceptives were seen at the end of the intervention. Compared to pre-intervention stage, a higher percentage of the participants disagreed that contraceptives were only for adult married persons. This may hold a consequence for those who are not married; they are therefore encouraged to use contraceptives as desired. In a similar pattern, a higher percentage no longer saw contraceptives as expensive and that adolescents who used them were not bad people. Having known the health importance of contraceptives, cost implications became less of a hindrance to its use. Also, a higher percentage disagreed that contraceptives led to infertility at the end of the intervention. On the other hand, a higher percentage of participants agreed that contraceptives were effective in avoiding pregnancy and therefore approved its use. Targeted education is highly valuable in changing false views and perceptions about certain health concerns.
Certain factors were found to influence uptake of contraceptives. It was revealed that educational level had an impact on uptake of contraceptives. Following findings in the current study, higher educational level was more likely to predict high uptake of contraceptives than lower level of education. In same way, having a high level of knowledge on contraceptives could suggest its high uptake. This implies that exposure to information on contraceptives may be a contributing factor to its use. A high uptake of contraceptives was significantly influenced by use of contraceptives before or after first pregnancy. Exposure to contraceptives early could influence increased uptake of contraceptives. Those who were influenced by health workers to use contraceptives were less likely to have high uptake of contraceptives compared to those who were influenced by media, friends and spouses. The use of contraceptives among these persons may have resulted from counselling by the health worker. It follows that counselling and education of women on use of contraceptives could be an influencing factor in their uptake.
Study limitations
In this study, only women who accessed healthcare at the study facility NAUTH within the period of study were invited to participate. Almost all had at least a high school education. This study may have missed the population of women who were not enlightened and unable to assess a tertiary health facility. Consequently, the findings in this study are representative of the population of women who accessed care in tertiary health facilities in Nnewi. The recommendation made was based on the limitations noted above.
Conclusion
Educational intervention had a significantly positive effect on the level of awareness and uptake of contraceptives, as displayed in the intervention group. A significant positive change in perception of contraceptives was noted among the intervention group in almost all the questions. This is in contrast with findings among the control group. There is a need for studies with longer follow-up to ascertain sustained impact of health education on uptake of contraceptives. Further studies should be carried out in the other facilities in Nnewi to ensure a better coverage and representation of the target population. Also, the study should be replicated at the state level for a better appreciation of the uptake of contraceptives in the state. Finally, related studies should be carried out among men.
Supplemental Material
sj-doc-1-smo-10.1177_20503121241237877 – Supplemental material for A randomized controlled study of the effects of targeted health education on uptake of contraceptives among women of reproductive age in Nnewi City, South-East Nigeria
Supplemental material, sj-doc-1-smo-10.1177_20503121241237877 for A randomized controlled study of the effects of targeted health education on uptake of contraceptives among women of reproductive age in Nnewi City, South-East Nigeria by Yanmeer Simeone Tyotswam, Rosebella Alungata Iseme and Eliphas Gitonga Makunyi in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241237877 – Supplemental material for A randomized controlled study of the effects of targeted health education on uptake of contraceptives among women of reproductive age in Nnewi City, South-East Nigeria
Supplemental material, sj-docx-2-smo-10.1177_20503121241237877 for A randomized controlled study of the effects of targeted health education on uptake of contraceptives among women of reproductive age in Nnewi City, South-East Nigeria by Yanmeer Simeone Tyotswam, Rosebella Alungata Iseme and Eliphas Gitonga Makunyi in SAGE Open Medicine
Footnotes
Acknowledgements
We thank the 275 reproductive-aged women in Nnewi for participating in the effects of targeted education on uptake of contraceptives and for sharing very personal information about their health. This study would not have been possible without the support of the Management of Nnamdi Azikiwe University Teaching hospital, Nnewi- Nigeria and the Department of Population, Reproductive Health and Community Resource Management, Kenyatta University, Nairobi-Kenya.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Nnamdi Azikiwe University Teaching Hospital Health Research Ethics Committee (NAUTHHREC). Approval Number/ID: NAUTH/CS/66/VOL15/VER3/102/2022/041.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Trial registration was done with Pan African Clinical Trials Registry (pactr.samrc.ac.za): PACTR202306677547495.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.