
Abstract
Introduction:
Immunization helps reduce morbidity and mortality attributable to severe vaccine-preventable childhood illnesses. However, vaccination coverage and the quality of immunization data remain challenging in Ethiopia. This has led to poor planning, suboptimal vaccination coverage, and the resurgence of vaccine-preventable disease outbreaks in under-immunized pocket areas. The problem is further compounded by the occurrence of the COVID-19 pandemic and the disruption of the health information system due to recurrent conflict. This study assessed the current status of the immunization service and its challenges in Ethiopia.
Methods:
A mixed-methods study was conducted in three regions of Ethiopia from 21 to 31 May, 2023. A survey of administrative reports was done in a total of 69 health facilities in 14 woredas (districts). Nine KIIs were conducted at a district level among immunization coordinators selected from three regions to explore the challenges of the immunization program. Linear regression and descriptive statistics were used to analyze the quantitative data. Thematic analysis was applied to analyze the qualitative data. The findings from the qualitative data were triangulated to supplement the quantitative results.
Result:
Two-thirds (66.4%) of the children were fully vaccinated, having received all vaccines, including the first dose of the MCV1, by 12 months of age, as reported through administrative reports collected from health facility records. Catchment area population size and region were significantly associated with the number of fully immunized children (p < 0.001 and p = 0.005, respectively). The vaccination dropout rates of the first to third dose of pentavalent vaccine and the first dose of pentavalent vaccine to the first dose of MCV1 were 8.6% and 7.4%, respectively. A considerable proportion of health facilities lack accurate data to calculate vaccination coverage, while most of them lack accurate data for dropout rates. Longer waiting time, interruptions in vaccine supply or shortage, inaccessibility of health facilities, internal conflict and displacement, power interruption and refrigerator breakdown, poor counseling practice, and caretakers’ lack of awareness, fear of side effects, and forgetfulness were the reasons for the dropout rate and low coverage. The result also showed that internal conflict and displacement have significantly affected immunization coverage, with the worst effects seen on the most marginalized populations.
Conclusion:
The study revealed low vaccination coverage, a high dropout rate, and poor quality of immunization data. Access and vaccination coverage among marginalized community groups (e.g., orphans and street children) were also low. Hence, interventions to address organizational, behavioral, technical, and contextual (conflict and the resulting internal displacement) bottlenecks affecting the immunization program should be addressed.
Keywords
Introduction
Vaccination has significantly contributed to public health, including the eradication of diseases such as smallpox. It has also led to a significant reduction in morbidity and mortality from vaccine-preventable diseases.1,2 Expanding access to immunization is crucial to achieving the Sustainable Development Goals. 3 However, vaccine-preventable diseases are still responsible for about 25% of the 10 million deaths occurring annually among under 5-year-old children. 4
Ethiopia started routine immunization in 1980 and has made notable progress in increasing vaccination coverage. 5 Between 2000 and 2019, the basic vaccination coverage had progressed from 14.3% to 44.1%. The vaccination coverage was estimated to reach 53.6% by 2025, indicating a significant gap in achieving the intended target of 90%. 6 The 2019 Ethiopian demographic health survey also indicated that almost two-thirds of children in Ethiopia are unprotected against major childhood diseases. 7 In addition, the regional vaccination coverage in Ethiopia over the last 2 decades has also shown considerable variability among regions, with the lowest in Afar (37.2%) and the highest in Addis Ababa (77%). 8
In the past 5 years, the coverage of immunization services has remained suboptimal because of the impact of COVID-19 and internal conflict. The destruction of health system infrastructure, internal displacement, and vaccine supply disruption, including a ban on movement, have impacted the immunization program. This may have hampered regular immunization campaigns, resulting in decreased coverage and increased dropouts.9–11 A further decrease in routine immunization coverage would cause many children to be unvaccinated or under-vaccinated, putting their lives at risk of vaccine-preventable diseases. 12 In addition, the massive internal displacement in Ethiopia and the disruption and destruction of the health system have affected immunization programs.13,14
According to a study conducted in Ethiopia, only 39.9% of children aged 12–23 months had received all recommended vaccinations. 15 This demonstrates the necessity of assessing the regular immunization program’s efficacy to identify areas that call for improvement. Furthermore, data quality issues that emanate from poor recording and reporting affect the accuracy of vaccination coverage. Studies show a gap in the timeliness and accuracy of reporting on vaccination records (tally sheet and register) and district health information system 2 (DHIS2).16,17
Given the recurrent conflicts and political instability in Ethiopia, understanding the current immunization program performance and contextual bottlenecks is important to inform immunization programs and strategies. Therefore, this study aimed at determining the current vaccination coverage, dropout rate, and data quality and explored the challenges of the expanded program of immunization (EPI) in Ethiopia.
Methods and materials
Study setting and period: This study was conducted in Amhara and Oromia regions and Addis Ababa City Administration in Ethiopia. The data were collected from 21 to 31 May 2023.
Study design: A mixed-method study was conducted. A cross-sectional study design was used to assess immunization status and the quality of immunization data. An interpretative phenomenological approach was used to collect data using key informant interviews (KIIs) about the challenges facing the immunization program.
Study population and data source: Vaccination records of <1-year-old infants were used as a source of data. Data for the following variables or indicators: percent of fully vaccinated children, vaccination coverage for different antigens, dropout rate, and percent of children protected at birth (PAB) were extracted from different records. Data quality was also assessed from facility records. The data were retrieved from the administrative records, including tally sheets, health management information system (HMIS) registries, DHIS2, and EPI reports. For the qualitative study, woreda (district) EPI focal personnel were included in the KIIs.
Eligibility criteria: For the quantitative study, infants who received their vaccinations at selected health facilities were included. Infants with incomplete records about their vaccination history were excluded.
For the qualitative study, health professionals who oversee immunization programs at the woreda level, aged 18 years or older, consented to participate in the study, and who worked for more than 6 months were included.
Sample size: The sample size was calculated using a formula used for a facility-based survey 18 by assuming an anticipated proportion (p) of 50%, a confidence level (z) of 1.96, a margin of error (ME) of 15%, and a design effect (d) of 1.5. The total number (N) of facilities in the study area was 587.



By adding a 10% non-response rate, the final sample size was 69 health centers. On average, five health centers are expected per woreda. Hence, to calculate the required number of woredas to cover 69 health centers, the calculated sample size was divided by 5, which equaled 14 woredas.
To complement the quantitative data, nine KIIs were conducted among EPI focal personnel from woreda or district health offices. In a qualitative study, achieving information saturation is deemed sufficient instead of setting a predetermined sample size. Studies also suggest 5–50 interviews as adequate. 19 Hence, the nine KIIs were determined based on information saturation during data collection.
Sampling method: A multistage stratified probability sampling method was employed. First, the regions were selected purposively, and then a list of woredas from the selected regions was prepared. Second, the 14 woredas were proportionally allocated to each region. Next, the allocated numbers of woredas were randomly selected from the list of woredas prepared for each region. Accordingly, seven, six, and one woredas were included from Oromia and Amhara regions and Addis Ababa city administration, respectively. All health centers in the selected woredas were included in this study. For the qualitative part, the nine key informants were purposively selected from the three regions (five, four, and one from Oromia, Amhara and Addis Ababa, respectively) and interviewed.
Data collection tools and method: For the quantitative study, an immunization data abstraction checklist was developed and used to collect data from the administrative records that included HMIS registers, tally sheets, DHIS2, and reports. For the qualitative part, a KII guide was developed and used. The English version of the KII guide was translated into local languages (Amharic and Afan Oromo) for data collection. The data collection tools (the immunization data abstraction checklist and KII guide) were pretested and based on input from the pretest, revisions were made before the actual data collection. The data were collected electronically using Open Data Kit (ODK) software by trained data collectors.
The qualitative data was collected by four (three male and one female) trained health professionals who hold a master’s degree in public health and have qualitative data collection experience. The data collectors received training for 2 days, along with a simulation. No relationship was established with the study participants prior to the start of the study. The study participants were informed about the name of the interviewer and the objective of the study, and informed consent was sought before initiating the data collection process. The data were collected at their workplace using face-to-face interviews and were conducted in an environment that ensured privacy. The interviews were tape-recorded, and side notes were taken. The KIIs were conducted until data saturation was reached, which was achieved with the nine KIIs. The interview lasted 30–45 min on average.
Data analysis: The quantitative data were exported to STATA version 17 StataCorp LLC for analysis. A descriptive analysis was used to summarize the data. A linear regression model was used to identify the factors associated with the number of fully vaccinated children at 5% level of significance and 95% confidence interval. In this study, the dependent variable is the number of fully vaccinated children, while the independent variables are population size, health worker volume (the ratio of health care providers to catchment area population), and regions.
The qualitative data were transcribed verbatim in the language of the interview and then translated into English. The translated data were cross-checked with the audio file to ensure consistency. The data were exported to MaxQDA 2022 software VERBI Software for analysis. First, line-by-line coding was done by the researchers to reduce the data. Then, similar codes were combined to produce categories. Finally, thematic analysis was applied to analyze and present the data. To ensure saturation, themes were identified until no further new themes appeared. The findings from the qualitative data were triangulated to supplement the quantitative results. In addition, representative quotations were included to contextualize the themes. Licensed versions of STATA version 17 and MaxQDA 2022 were used for data analysis.
Data quality assurance and management: The checklist used to collect the quantitative data was pretested in 5% of the health facilities prior to the data collection. The data obtained from the pretest was used to modify the checklist. Training was given to data collectors and supervisors. Supervisors closely monitored the data collection process. The completeness and credibility of the data were also ensured by using aGlobal Positioning System (GPS)-enabled ODK.
The KII guide was pretested, and a revision was made accordingly. Credibility was ensured through probing, the use of experienced data collectors who are familiar with the immunization settings in Ethiopia, training of data collectors, in-depth methodological description, and ensuring the adequacy of the data (saturation). The research team carefully read the information obtained from individual interviews and field notes. All the information provided by the participants was fully presented. Participant validation was also made by returning the transcripts to participants to check for accuracy and resonance with their experiences, and their feedback was considered. To ensure transferability, a detailed and complete description of the data and context was provided.
Ethical approval and consent to participate: This research was undertaken in accordance with the Declaration of Helsinki. Ethical approval was obtained from the John Snow, Incorporated (JSI) Institutional Review Board (IRB) (approval number IRB #22-54E). Formal permission was obtained from the Federal Ministry of Health, the Regional Health Bureaus, and the heads of the sampled health facilities before data collection. Written informed consent was obtained from all study subjects. The confidentiality of the information was maintained, and the data were recorded anonymously throughout the study. The vaccination-related data and KII recordings and transcripts were stored on a password-protected computer. Side notes and any other recordings were destroyed once the summary was prepared.
Operational definitions for indicators
Percent of fully vaccinated children: Proportion of infants that received all doses of all EPI vaccines, including the first dose of measles conjugated vaccine (MCV1), before the age of 1 year (the number of infants that received all doses of all vaccines divided by the number of infants in the target population multiplied by 100).
Vaccination coverage rate: Proportion of infants that received doses of a particular vaccine (number of infants that received doses of a particular vaccine divided by the number of infants in the target population multiplied by 100).
Dropout rate: Infants who started vaccination but did not complete the schedule: - Pentavalent (penta)1 to penta3 dropout rate is estimated as the difference of penta1 and penta3 divided by penta1 multiplied by 100. - Penta1 to MCV1 dropout rate is estimated as the difference of penta1 and MCV1 divided by penta1 multiplied by 100.
Percentage of children PAB from neonatal tetanus: This is an alternative method to determine TT2+ coverage to monitor PAB (number of infants PAB divided by the number in the target population multiplied by 100).
Data accuracy: the number of vaccinations re-counted from the source document (register) to the number of vaccinations reported through DHIS2.20,21
In this study, penta1 coverage was used to assess access; penta1, penta3, MCV1, and TT+ coverage were used to measure vaccination coverage; and dropout rates (penta1 to penta3 and penta3 to MCV1) were used to measure utilization.
Result
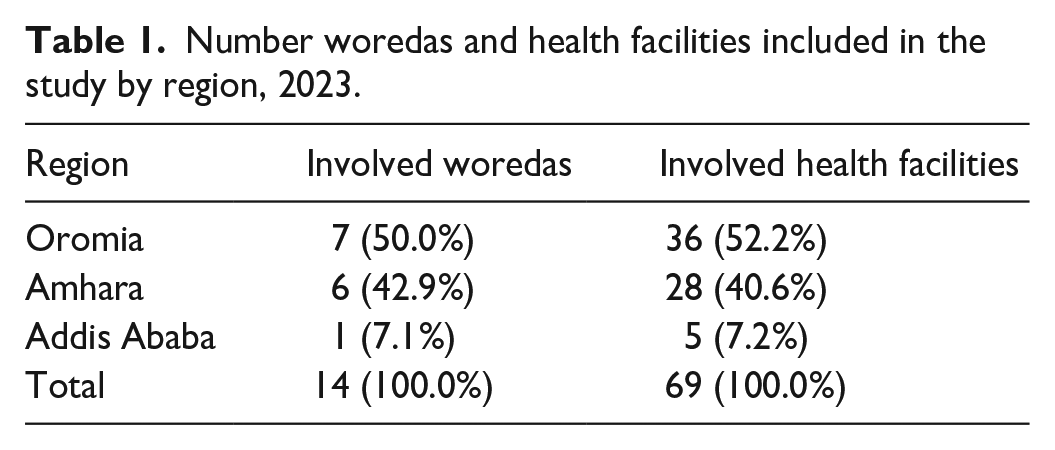
Overview of the study sites: A total of 69 health centers from Oromia and Amhara regions and Addis Ababa City administration were included in the study. More than half (52.2%) of the facilities were from Oromia region, while the remaining 40.6% and 7.2% were from Amhara region and Addis Ababa City Administration, respectively (Table 1).
Number woredas and health facilities included in the study by region, 2023.
A total of nine KIIs were conducted. About two-thirds (65.6%) were females. The majority of them (66.7%) were health officers by profession, and 55.6% were bachelor’s degree holders (Table 2).
Socio-demographic characteristics of the key informants, 2023.

Immunization coverage: Vaccination records of 17,927 children aged less than 12 months were retrieved from the sampled health facilities, covering the period 1 January–31 March 2023. Two-thirds, 66.4% (95% CI: 51.9, 80.8), of children were fully vaccinated, having received all doses of all vaccines, including MCV1, by 12 months of age. The proportion of full immunization in the health facilities in Amhara, Oromia, and Addis Ababa was 56.1%, 70.7%, and 85.6%, respectively.
More than three-quarters (77.4% (95% CI: 62.7, 92.2)) of the children received the first dose of pentavalent vaccine, 70.1% (95% CI: 55.5, 84.7) of them received the third dose, and 68.1% (95% CI: 54.2, 82.0) of them received MCV1. In addition, 73.4% (95% CI: 58.5, 88.4) of infants were protected at birth from neonatal tetanus (Table 3).
Proportion of under one child who received vaccines by regions, 2023.

Aggregate refers to the total data across the three study sites.
Generally, successful vaccination requires the presence of adequate vaccines, adequate storage and distribution, proper vaccine administration, public trust, monitoring system, and government support. However, most respondents reported several challenges, such as long waiting times, inaccessibility of health facilities, shortage of vaccines, and challenges related to basic amenities, mainly electric power and refrigerators. Vaccine shortages made it difficult to vaccinate children during their visit and reach out to those who missed their schedule.
We do not have a generator or a means to maintain damaged refrigerators. This is significantly affecting the delivery of vaccination services. (EPI focal person from Debrebirehan, Amhara) . . .Vaccines are not enough to immunize the children. (EPI focal person from Agaro Woreda, Oromia)
In urban areas like Addis Ababa, shortages of staff and rooms for the immunization program were mentioned as challenges for the performance of the EPI program. This has led to long waiting time, delays in service delivery, and even missed opportunities for immunization.
The challenge that we are facing is that we have a single room where vaccines are given and few health workers responsible for it. In addition, we have a schedule, which means a designated day when specific vaccines are given. These all bring long waiting time against which clients get bored and sometimes decide to leave the facility without getting the vaccine (EPI focal from Addis Ketema Sub-city, Addis Ababa)
In addition, there is an observable disparity in access to vaccination services, significantly affecting children from homeless families, orphans, and the internally displaced segments of the population, mainly exacerbated by the recent conflict in the country.
It is difficult to know the status of children who received their vaccine in other places and came to us. Especially here in Debre Birhan, there are many families and children who are displaced due to the current conflict. We can’t address all of them. Not only that, we may not address street children, and we cannot address those who have migrated from different places. So, there are caretakers and babies who are missed because of this.(EPI focal person from Debrebirehan, Amhara)
Human resources and competency appear to be even more prominent. Most of the key informants mentioned that there is a high turnover of healthcare providers and limited opportunities for training. Untrained staff and a heavy workload affected client counseling and the practice of record-keeping during vaccination.
During our health facility visits, we have seen that staff were overloaded. This is because health professionals are leaving health facilities in search of better-paying jobs. There is also a skill gap among newly hired professionals. This is affecting the immunization program. (EPI focal from Agaro, Oromia)
Lack of compliance with instructions given by service providers regarding immunization and lack of awareness of its benefits also affected the EPI implementation.
It feels nice when caretakers respect their appointment dates, and it is discouraging when they sometimes do not bring their children on the dates of appointment because of this it seems like we are not doing our work. (EPI focal person from Arsi Negelle, Oromia)
Dropout rate: The dropout rate from the first to the third dose of the pentavalent vaccine was 8.6%, and from penta1 to MCV1 vaccination was 7.4%. There was a statistically significant difference in the penta1 to penta3 dropout rate among regions, with Addis Ababa having the largest dropout rate (p < 0.05). However, there was no statistically significant difference in penta1 to MCV1 dropout rate among the regions (p ⩾ 0.05) (Figure 1).
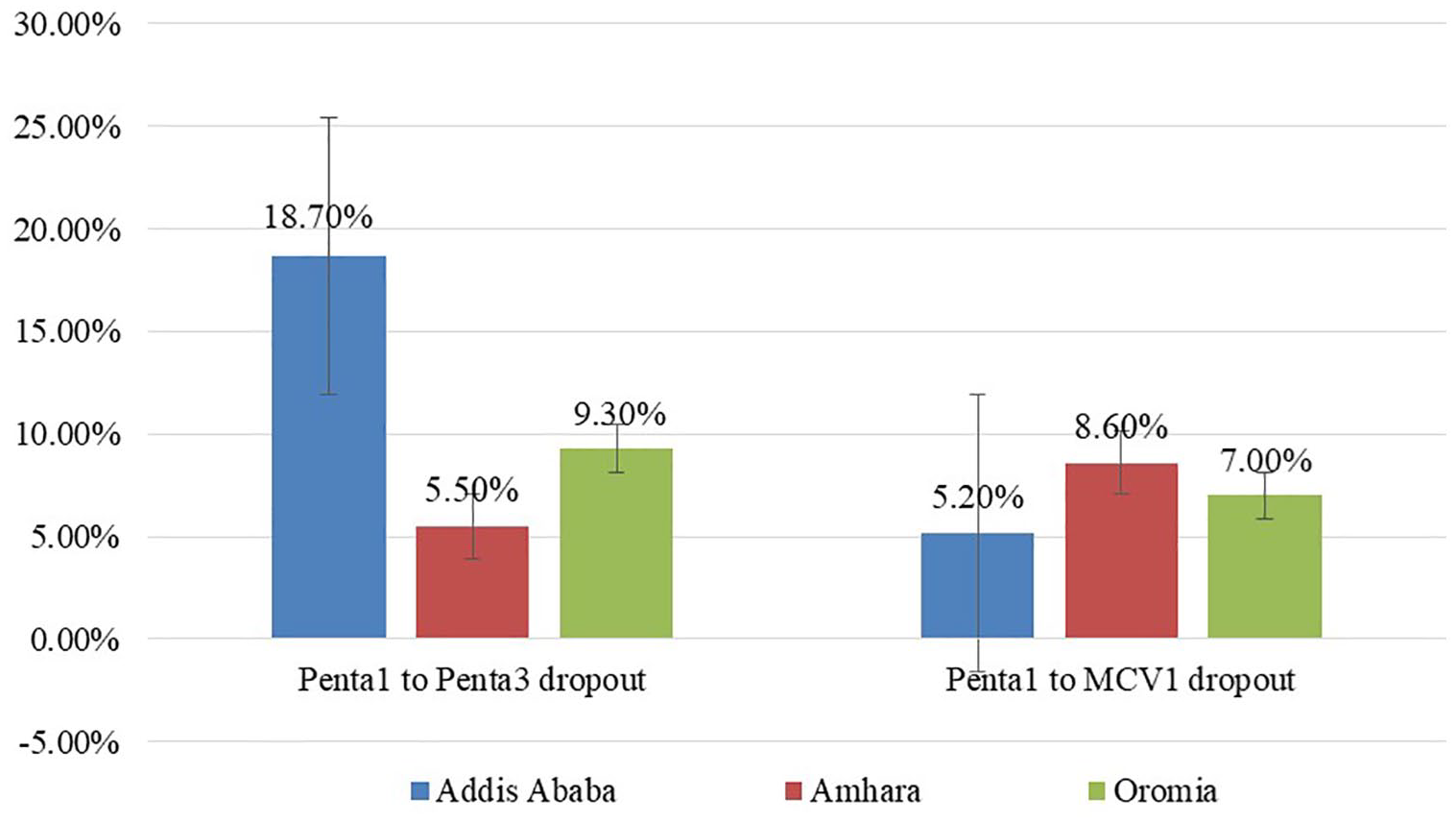
Dropout rate by region and antigens, 2023.
Proper counseling and reminders enhance vaccine uptake. On the other hand, poor counseling practice and a lack of reminders from health workers can lead to delays or missed opportunities for immunization and increase the risk of vaccine-preventable diseases. Key informants reported poor counseling practice, forgetfulness, long waiting time, and fear of side effects as barriers resulting in dropout from the EPI schedule.
The counseling provided by health care providers is minimal and mostly nothing more than telling the next appointment date. Caretakers are often not told about the types of vaccines, including the benefits and the possible side effects. (EPI focal person from Legetafo, Sheger City)
In rural areas, where there are long distances between health facilities and communities, it can be challenging for people to access immunization services. This can be due to a lack of transportation, poor infrastructure (roads, electricity, etc.), or the limited availability of health workers and supplies. As a result, many children may be left unvaccinated, which can lead to outbreaks of vaccine-preventable diseases. Respondents mentioned that, despite the presence of outreach services, the distance to access health facilities challenged them to access immunization services.
Accessibility of health facilities remains a challenge to us. Women from faraway places are less likely to complete the schedule. That is why we work hard on the outreach service. (EPI focal person, Chagni Wereda, Amhara)
Most health facilities have a shortage of health workers. One or two healthcare workers provide vaccination services, leading to long waiting times. Some caretakers get fed up with waiting too long and decide to go back home without getting their children vaccinated. Moreover, immunization service quality is another factor that causes dropout. Some healthcare providers do not appropriately administer the vaccine, causing complications and leading to lack of trust in the quality of services.
There is a heavy client load here and the waiting time is very long. A caretaker who comes in the morning may have to wait until 12 p.m. or 1 p.m. to get her child vaccinated. Sometimes they are fed up, and there are instances where they leave without getting the vaccines. (EPI focal person from Addis Ketema Sub-City, Addis Ababa)
Data quality
Data accuracy: Data accuracy, the percent of reported data against recounted from source documents, was determined by comparing DHIS2 reports of penta1, penta3, and MCV1 coverage and penta1 to penta3 dropout against facility registers and tally sheets, which are source documents. The data accuracy shows that there is a tendency to overreport performance. Penta1 coverage recounted from registers and tally sheets and reported through DHIS2 was 77.40%, 79.40%, and 82.35%, respectively. This indicates a 6%–16% discrepancy of the DHIS2 report against the source documents. Similarly, the penta1 to penta3 dropout rate was 8.60%, 13.20%, and 13.40% from registers, tally sheets, and DHIS2, respectively, signifying more than 10% discrepancy between DHIS2 and the EPI registers (Figure 2).

Coverage and dropout rates of antigens by source of immunization data, 2023.
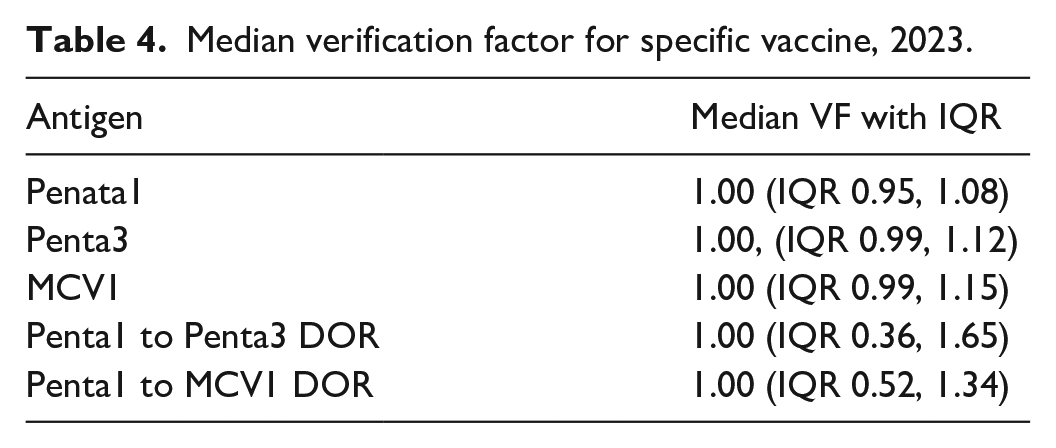
The median of the data accuracy ratio, or verification factor (VF), for each sampled health facility, was calculated as the ratio of the number of vaccinations recounted to the number of vaccinations reported by DHIS2. Accordingly, the median interquartile range (IQR) VF for penta1, penta3, and MCV1 was 1.00 (0.95, 1.08), 1.00 (IQR 0.99, 1.12), and 1.00 (IQR 0.99, 1.15), respectively. The upper margin of the IQR for penta3 and MCV1 is above the threshold, indicating poor data quality based on the WHO DQR guidelines. 21 Similarly, the median VF (IQR) for penta1 to penta3 and penta1 to MCV1 dropout was one with an IQR of (0.36, 1.65) and (0.52, 1.34), respectively. The fact that the median is 1 indicates that most health facilities have acceptable levels of data quality. The upper and lower bounds of the IQR less or greater than 10% indicate unacceptable data discrepancies between reports and source documents among some health facilities included in the study (Table 4).
Median verification factor for specific vaccine, 2023.
Facilities with VF out of the range (0.9 and 1.1) were considered to have unacceptable immunization data accuracy. Accordingly, 31.9%, 43.5%, and 46.4% of the health facilities had no accurate data for penta1, penta3, and MCV1 coverage, respectively. In addition, the majority, 76.8% and 81.2% of the health facilities had no accurate data for penta1 to penta3 and penta1 to MCV1 dropout rates, respectively.
Despite the use of technologies such as mHealth and mBrana tools (a vaccine and malaria nets distribution digital tracking tool), in addition to HMIS and DHIS2, respondents mentioned the existence of immunization data quality issues. The poor practice of data recording by healthcare providers was mentioned as a major challenge for data quality issues.
It is apparent that we observe inconsistency between data sources and DHIS2 or the report. (EPI focal person from Adama town, Oromia) Some healthcare providers focus only on providing the vaccination service and ignore registering the information. As a result, the data in the source document appears different from the data reported. (EPI focal person from Bishoftu town, Oromia)
They also reported that some healthcare workers report false information with the intention to give false impressions of achievement. Furthermore, the DHIS2 by itself is a problem.
There is some issue with the DHIS2 itself. The software displays different figures than what was encoded. The data in the DHIS2 show signs of manipulation in terms of the number and order of immunization indicators. The software also doesn’t allow users to make corrections when needed. It is a national issue, and has been reported to the concerned partners for a solution. (EPI focal person from Agaro town, Oromia)
Moreover, lack of training opportunities and shortage of supplies were mentioned as challenges in ensuring immunization data quality by most of the respondents. Due to the high turnover of staff, untrained staff were assigned to the EPI program. Shortages of supplies, including electric power, internet, and registration documents, were also reported as challenges affecting immunization services.
During health facility visits, we have seen staff being overloaded. This is because health professionals are leaving health facilities in search of better-paying jobs. There is also a skill gap among newly hired professionals. This is affecting the immunization program. (EPI focal from Agaro, Oromia) We receive one registration book for almost 3 years, which is not enough. (EPI focal person from Finote Selam town, Amhara)
Report completeness and timeliness: The completeness of the immunization reports of health facilities was 85.9%, of which 91.2% and 6.0% were reported on time and late to the woreda or district health offices, respectively (Figure 3).

Report timeliness and completeness, 2023.
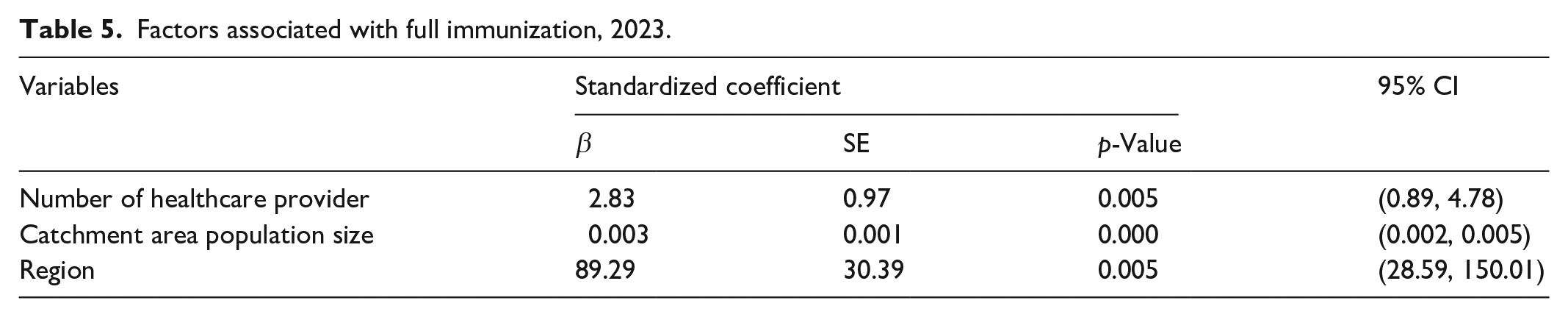
Factors associated with full immunization: Catchment area population size and region were significantly associated with full immunization (p < 0.001 and p = 0.005, respectively) (Table 5).
Factors associated with full immunization, 2023.
Discussion
This study reports on immunization coverage, data quality, and immunization program challenges in Ethiopia. Accordingly, coverage of penta1, penta3, MCV1, and full immunization were 77.4%, 70.0%, 68.1%, and 66.4%, respectively. Similarly, the penta1 to penta3 and penta1 to MCV1 dropout rates were 8.6% and 7.4%, respectively. Furthermore, 73.2% of children were PAB from neonatal tetanus.
Full immunization (66.4%) in this study is consistent with previous studies in Ethiopia.22–25 However, existing evidence doesn’t reflect post-COVID-19 and post-conflict vaccination coverage in Ethiopia. 26 Compared to prior research or national reports, this study reports a lower proportion of full immunization. For example, previous assessments in Addis Ababa and Assossa, Ethiopia, reported a higher coverage of 82.3% compared to 66.4% in this study.27,28 The disruption of the immunization service due to COVID-19, internal conflicts, and displacement may have influenced the study’s findings.
The regional distribution also showed a lower rate of full immunization for the Amhara region compared to Oromia region and Addis Ababa city administration. This is probably due to the disruption of the health care system following the conflict in the region, which affected the availability and accessibility of essential health services. The qualitative findings also revealed that internal displacement and health care disruption due to conflicts were challenges. Other studies conducted in the Amhara region also supported the claim that the conflict can significantly affect health care provision.29,30
Several challenges that have been limiting full immunization in this study are consistent with studies conducted on similar topics in Oromia and Amhara regions.11,31 These challenges include interruption of vaccine supply and problems related to basic amenities, particularly the interruption of electric power and the shortage and lack of refrigerator maintenance. The health facilities sometimes experience vaccine shortages, making it difficult for them to vaccinate children on their visits and reach out to those who have missed their schedule. A multilevel analysis of the Ethiopian Demographic and Health Survey also reported similar challenges. 32
Despite the remarkable progress made in the primary healthcare expansion and universal health coverage in Ethiopia, long waiting times for vaccination and long distances have continued to impact vaccination services, which in turn affect vaccination coverage. While women in urban areas, such as Addis Ababa, are suffering from long waiting time due to high attrition of healthcare providers and inefficient urban health extension programs, those in rural areas are challenged with long distances to access vaccination services as a result of improper functioning of nearby health posts. Several studies in sub-Saharan Africa, including Ethiopia, have also reported similar findings.33–35
Catchment area population size and region were significantly associated with full immunization. This finding is consistent with studies conducted in developing and developed countries.36–38 A higher volume of health workers in health facilities increases the availability of vaccination services over time and space, so that children are more likely to be vaccinated. 36
This study also highlighted the quality of immunization data by focusing on data accuracy, reporting completeness, and reporting timelines. Penta1, penta3, MCV1 coverage, and the penta1 to penta3 and penta1 to MCV1 dropout rate were considered key indicators. The study’s estimation of the verification factor underpins the consistency of the immunization data between the register and DHIS2. However, a considerable proportion of health facilities lack accurate data for vaccination coverage, while most of them lack accurate data for dropout rates. The poor practice of data recording by healthcare providers was mentioned as a major challenge for the data quality issues in this study. Lack of training and shortage of recording and reporting tools were also reported as challenges. Findings from several countries also showed inaccuracy of immunization data due to poor practice of recording.39,40
There is inconsistency of immunization data between DHIS2 and the source document (register). The report from DHIS2 is higher than the registers. This can be mainly due to suboptimal data quality assurance practices. The inconsistency may also be attributed to either a problem with the denominator or inadequate planning resulting from incorrect use of the conversion factor for the eligible population. Studies conducted in low and middle-income countries also found a lack of immunization data consistency due to poor data management processes.41,42 A tendency of exaggerating performance by inflating vaccination coverage and decreasing dropout rate was also reported. Similar finding was reported by another study conducted in Amhara and Oromia regions. 43 Thus, it is important to validate immunization data and monitor vaccine preventable disease epidemics against coverage data to pick issues with data quality.
Although the impact of inaccurate data and false information in Ethiopia is not widely recognized, it can have detrimental effects. Healthcare management and policymakers rely on data to make informed decisions, and inaccurate data can result in improper decision-making, reduced efficiency, and a negative impact on the reputation of the healthcare system. Poor data quality is often linked to inadequate planning and resource allocation. 43 As a result, it is essential to address the data inaccuracy problem by designing appropriate strategies to improve the performance of the immunization program and enhance vaccination coverage. Data recording and reporting can be strengthened through capacity building, supportive supervision, close monitoring, and by introducing a technology that allows offline tracking of individual immunization data.
Unlike other studies, DHIS2 by itself is a problem. The data in the DHIS2 show signs of manipulation in terms of numbers reported without the knowledge of EPI focal persons who reported the numbers. Hence, further investigation is needed to identify the source of the problem.
Timeliness and completeness of reporting are the other key attributes under the data quality dimension that were assessed in this study. The study revealed a report timeliness and completeness of 86%, of which 91% were submitted on time. This shows that most district health offices receive timely reports for evidence-based decision-making. The finding is consistent with other studies conducted in Ethiopia and Iran.44,45
Limitations of the study
The result of this study should be interpreted in light of its limitations. Most of the data used in the study were from secondary data sources, and the limitations of such data may affect the study. In addition, the survey involved health facilities, not households, which were selected from only three regions, which may introduce selection bias and is not representative of the situation at the community level. This was also a cross-sectional study design. Limitations inherent in the design also affect the study.
Despite the limitations, the findings from this study will contribute to the national, regional, and global efforts to ensure the health and survival of under-five children. The challenges identified will aid in planning interventions that can enhance the immunization program. The study also contributes to the efforts being made to realize the 2030 Sustainable Development Goal 3 46 and the 2063 African Union (AU) Agenda Goal 3. 47
Conclusion
The study revealed a lower proportion of full immunization compared to the national immunization data. The dropout rate was acceptable compared with the WHO reference (<10%). Some of the reasons for the dropout and low coverage included long waiting times, interruptions in vaccine supply, and internal displacement due to the conflict and political instability in Ethiopia. There were also disparities in vaccination coverage among different population groups. Specifically, orphaned and homeless children may be less well targeted.
Immunization data quality problems like inaccuracy and inconsistency were also observed. The most prominently mentioned reasons were lack of training, high client load, recklessness and high turnover of health care providers, and shortage of logistics. Hence, attention should be given to addressing organizational, behavioral, technical, and contextual factors influencing immunization data quality and coverage. Immunization equity must also be seriously considered.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241237115 – Supplemental material for The status of immunization program and challenges in Ethiopia: A mixed method study
Supplemental material, sj-docx-1-smo-10.1177_20503121241237115 for The status of immunization program and challenges in Ethiopia: A mixed method study by Tariku Nigatu, Loko Abraham, Herman Willems, Mesfin Tilaye, Firew Tiruneh, Fantay Gebru, Zergu Tafesse, Bezawit Getachew, Mulualem Bulcha, Sami Tewfik and Tadesse Alemu in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241237115 – Supplemental material for The status of immunization program and challenges in Ethiopia: A mixed method study
Supplemental material, sj-docx-2-smo-10.1177_20503121241237115 for The status of immunization program and challenges in Ethiopia: A mixed method study by Tariku Nigatu, Loko Abraham, Herman Willems, Mesfin Tilaye, Firew Tiruneh, Fantay Gebru, Zergu Tafesse, Bezawit Getachew, Mulualem Bulcha, Sami Tewfik and Tadesse Alemu in SAGE Open Medicine
Footnotes
Acknowledgements
We are grateful to the United States Agency for International Development (USAID) and Global Vaccine Alliance (GAVI) for funding this study. We also acknowledge staff at regional health bureaus, woreda health officials, and staff at health facilities for their cooperation during data collection, and all key informants for their willingness to participate in the study.
Authors’ contribution
TB, FT, and TA were involved in research conception and design, collection and organization of data, data analysis and interpretation, writing the report, and manuscript preparation. LA, HW, MT, FG, ZT, BG, MB, and ST were involved in data analysis and interpretation and helped in the write-up and revision of this work. All authors contributed to the article and approved the submitted version.
Accessibility of data and materials
Data supporting the findings in this research article are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the USAID and GAVI. The funders are not involved in the design, analysis, report writing, and dissemination of results of this study.
Ethical approval
Approval and ethical clearance were obtained from the John Snow, Incorporated (JIS) Institutional Review Board (IRB) (Approval number IRB #22-54E).
Informed consent
Before data collection, the study’s objective and purpose were clearly explained and written informed consent was obtained from all study subjects. They were also informed that they can decline to participate in the study at any time. The information was kept confidential, and the data was collected anonymously throughout the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.