
Abstract
Objective:
The primary aim of this study was to develop an Urdu-translated version of the Amsterdam preoperative anxiety and information scale and perform a psychometric evaluation of it. A secondary aim was to estimate the prevalence of preoperative anxiety using Urdu-translated Amsterdam preoperative anxiety and information scale in patients undergoing surgery in Karachi, Pakistan, and the factors contributing to anxiety among them.
Method:
This cross-sectional survey included 267 patients enrolled for elective surgery under general anesthesia from March 5 to November 20, 2022. In psychometric analysis, face validity, criterion validity, construct validity, and reliability of Urdu-translated Amsterdam preoperative anxiety and information scale were determined. Face validity was evaluated by performing blind-back translation and a pilot study. Criterion validity was evaluated by correlating the Amsterdam preoperative anxiety and information scale with the visual analog scale for anxiety. Exploratory factor analysis and Cronbach’s α test were used to analyze construct validity and reliability, respectively. The associate variables were identified by performing a one-sample t-test and one-way analysis of variance on SPSS 26.
Results:
Cronbach’s α test is 0.85 for the Amsterdam preoperative anxiety and information scale anxiety scale and 0.70 for the need for information. 65.3% of the total variance is explained by the Urdu version of Amsterdam preoperative anxiety and information scale items in factor analysis and the intercorrelation of all items was >0.20 (mean: 0.575). Urdu-translated Amsterdam preoperative anxiety and information scale and visual analog scale for anxiety showed a good correlation (r = 0.664, p < 0.001). The overall prevalence of preoperative anxiety among patients is 52.4% suggested by the Amsterdam preoperative anxiety and information scale cutoff score of more than 11. Females, students, and patients elected for major surgery shared significantly higher anxiety levels (p < 0.05). The commonest factors contributing to anxiety are postoperative pain in 140 (52.4%) patients, fear of death in 115 (43.1%), and financial loss in 91 (34.1%).
Conclusions:
The Urdu-translated Amsterdam preoperative anxiety and information scale is a reliable, valid, and acceptable screening tool for preoperative anxiety. The prevalence of preoperative anxiety was high. The preoperative anxiety level is significantly associated with gender, employment status, and type of surgery.
Keywords
Introduction
Exposure to surgical intervention leads to preoperative anxiety, a globally widespread problem among adult patients scheduled to undergo a surgical procedure. 1 Preoperative anxiety is defined as an unpleasant sensation of unease or stress during the preoperative period that compromises the patient’s comfort and well-being. It can potentially impact all the phases of surgery, from a preoperative visit to the postoperative recovery period.2,3 Preoperative anxiety has also been associated with developing physiological and autonomic symptoms such as tachycardia, blushing, excessive sweating, and high blood pressure. 4 These complications cause several detrimental clinical postoperative outcomes, including a prolonged recovery period, poor disease prognosis, and augmented postoperative pain.4,5 Furthermore, higher dosages of anesthetic drugs were needed to induce and maintain appropriate levels of anesthesia in anxious patients during surgery, which reportedly increased mortality in them. 6 Preoperative anxiety is not only attributed to fear of the surgical procedure itself. In fact, about 62% of the study population’s concerns and fears regarding anesthesia constituted the major source of preoperative fear, while only 15% reported fear of the surgical procedure. 7
Patients with high anxiety levels should be routinely identified during the anesthesiologist’s preoperative interview to provide adequate educational and psychological consultation to reduce preoperative fear and anxiety. 8 A brief, valid, and reliable screening tool that is suitable for preoperative interview settings can be implemented to assess anxiety levels. 2 The Amsterdam preoperative anxiety and information scale (APAIS) is a self-report questionnaire developed by Moerman et al., 9 specifically for evaluating preoperative anxiety. APAIS is distinct from other scales because of its ability to assess patients’ information requirements regarding their surgery and anesthesia, aiding in identifying and isolating those individuals whose anxiety can be mitigated through the provision of more information and focused attention. APAIS is a widely accepted anxiety screening tool that has been translated and implemented in studies in many countries, including Italy, 10 Japan, 11 Mexico, 12 Ethiopia, 13 Sri Lanka, 14 China, 15 and India. 16 All these studies reported variations in anxiety levels and their dependent variables due to the influence of cultural and ethnic differences.10–16 However, none of the studies reported from Pakistan translated APAIS into Urdu language and performed a psychometric analysis of it.
Therefore, the primary aim of this study was to provide an Urdu-translated version of APAIS for ease of use in the Pakistani population and perform a psychometric evaluation of it. A secondary aim was to estimate the prevalence of preoperative anxiety using APAIS in patients undergoing surgery in a secondary and tertiary care hospital in Karachi, Pakistan, and the factors contributing to anxiety among them.
Methods
This cross-sectional survey was conducted at Creek General Hospital, United Hospital, and Civil Hospital in Karachi from March 5 to November 20, 2022. The study was approved by the Institutional Review Board (IRB) of United Medical and Dental College, Karachi, and conducted according to the ethical principles of the Helsinki Declaration. All adult patients scheduled for any type of surgery under anesthesia within the fields of general surgery and orthopedics were invited to participate in the study. Inclusion criteria were all patients from general surgery and orthopedic wards undergoing elective surgical procedures for benign diseases with age >18 years, American Society of Anesthesiology physical status of 1–3, 17 and being able to speak and understand Urdu language. Patients with psychiatric illnesses, unable to answer the questionnaire, or unwilling to participate in the study were excluded. The surgical procedures performed on all included participants were classified into two categories: major surgery and minor surgery. Major surgery encompasses complex and invasive procedures, which are expected to result in a blood loss exceeding 500 mm, necessitating significant fluid replacement, and typically require at least one overnight hospital stay. By contrast, minor surgery includes minimally invasive procedures with blood loss of less than 500 mm, minimal fluid replacement, and often allows for same-day discharge on an ambulatory basis. Data were collected from patients immediately before entering the operating room, and filling out of consent form was mandatory for every participant in the study. A sample size of 255 was obtained by single proportion infinite sampling method using a prevalence of 62%, confidence interval of 95%, and 5% margin of error. 18 However, 270 patients were approached, and 267 filled out the questionnaire (the non-response rate was 2%). A random systematic sampling technique is utilized for the data collection process.
Study instrument
The questionnaire was composed of four sections: (1) demography, (2) APAIS, (3) VAS-A, and (4) factors contributing to anxiety. The APAIS comprises six 5-point Likert scale-type questions, which can be divided into two subscales. 9 The first subscale contains four items concerning the patient’s anxiety about anesthesia and surgery (A1, A2, A4, and A5), and the second subscale contains questions to evaluate the need for information (A3 and A6). The score ranges from 4 to 20 for the anxiety scale (A1, A2, A4, and A5), and 2–10 for the need for information component (A3 and A6). The VAS-A is a self-reported scale that consists of a 100 mm horizontal line with the left end marked as no anxiety (score: 0) and the right end as maximum anxiety (score: 100). 19 To determine different factors contributing to preoperative anxiety other than surgery, we offered a list of different causes and asked participants what are the relevant factors contributing to their anxiety.
Development, psychometric analysis, and Urdu version of APAIS
Development and face validity: The translation of APAIS was done in Urdu (i.e., the national language of Pakistan) with the use of the English version in accordance with guidelines for adaptation and validation of instruments in cross-cultural healthcare research. 20 Two physicians (proficient in both English and Urdu language) did an initial translation of the instrument, and then the blind-back translation of the initial version was performed by a bilingual surgeon to detect any semantic, lexical, morphology, and grammar errors (see Table 1). A pilot study was performed on 25 patients (9% of the total study population) to assess the face validity, comprehension, and acceptability of the final version among participants.
Urdu translated version of APAIS.

Construct and criterion validity: The construct validity was measured by exploratory factor analysis using a principal component of oblique rotation. The criterion validity was determined by comparing the APAIS scale with VAS-A using Pearson’s correlation test.
Reliability and internal consistency: The reliability of items was calculated using Cronbach’s α test. Internal consistency of an item is reported by inter-item correlation and variance of scale if an item is deleted.
Statistical analysis
The data analysis was carried out using IBM Corporation’s Statistical Package for the Social Sciences (SPSS) version 26.0, based in Armonk, NY, USA. Descriptive statistics were applied, and frequencies and percentages were calculated for all sociodemographic variables. The total score of the APAIS was presented as the mean and standard deviation. Pearson’s correlation tests were used to evaluate the relationship between the APAIS anxiety scale and the need for information. Student’s t-test (one sample t-test) was used to determine differences in the APAIS anxiety score against gender, material status, surgical discipline, and type of surgery. One-way ANOVA was used to compare anxiety scores with age, employment status, educational status, and past surgical experience. All p-values of less than 0.05 were considered statistically significant.
Results
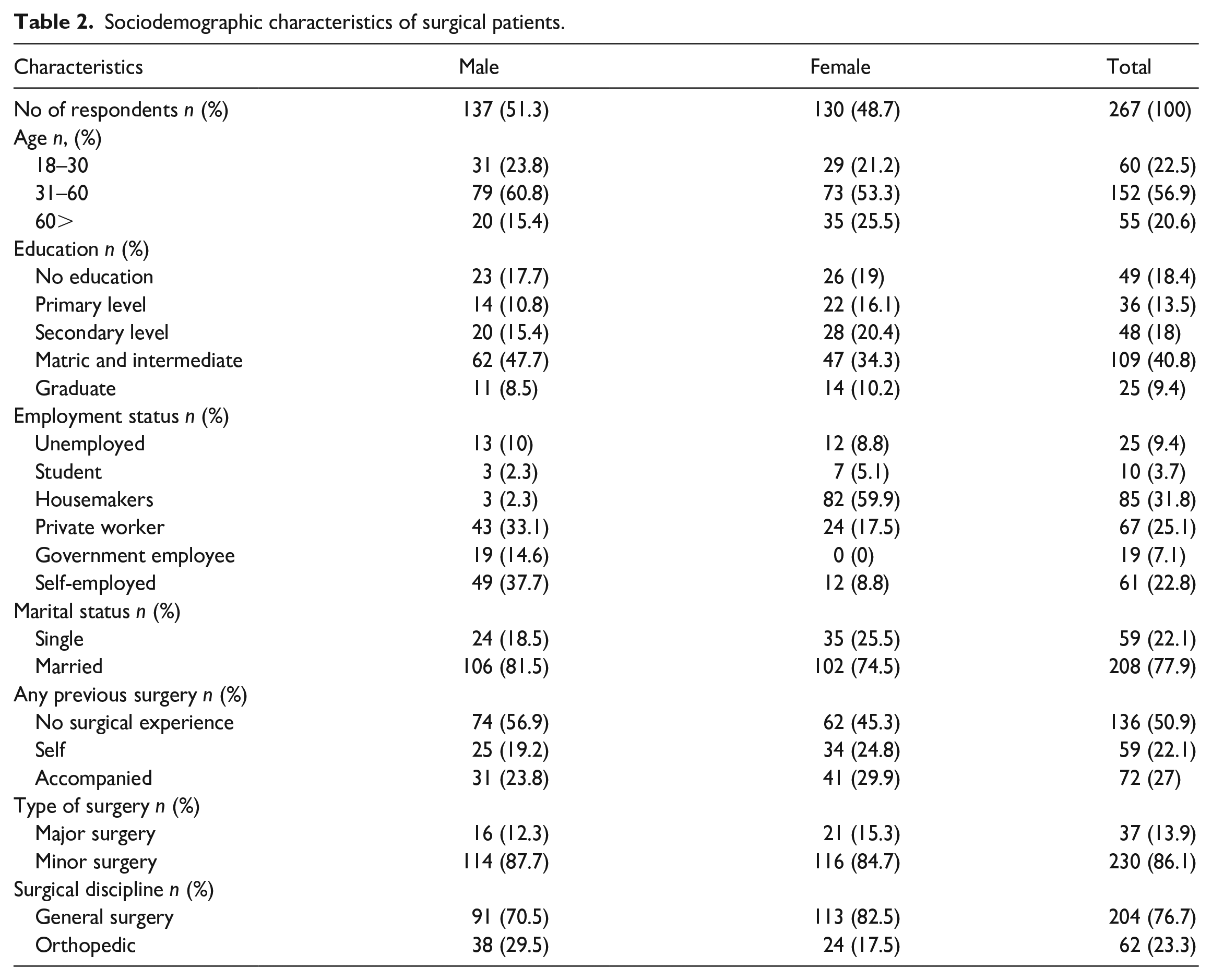
The Urdu version of APAIS is shown in Table 1. Data were collected from 267 patients, out of which 37 (13.9) were enrolled for major surgeries and 230 (86.1) for minor surgery (see Table 2). The participants were 137 (51.3%) females and 130 (48.7%) males, out of which 208 (77.9%) were married. More than half of the study participants 153 (57.3%) were between the ages of 18 and 30 years, and 109 (40.8%) participants had an educational background of Matriculation/Intermediate (Primary Education). In all, 67 (25.1%) participants were salaried individuals, 61 (22.8%) were self-employed or had a private business, and 25 (9.4%) patients were unemployed. Only 59 (22.1%) participants had a history of previous surgery, while 72 individuals (approximately 27%) had previously accompanied their close relatives to the hospital during the relatives’ surgical procedures, serving as attendees for them.
Sociodemographic characteristics of surgical patients.
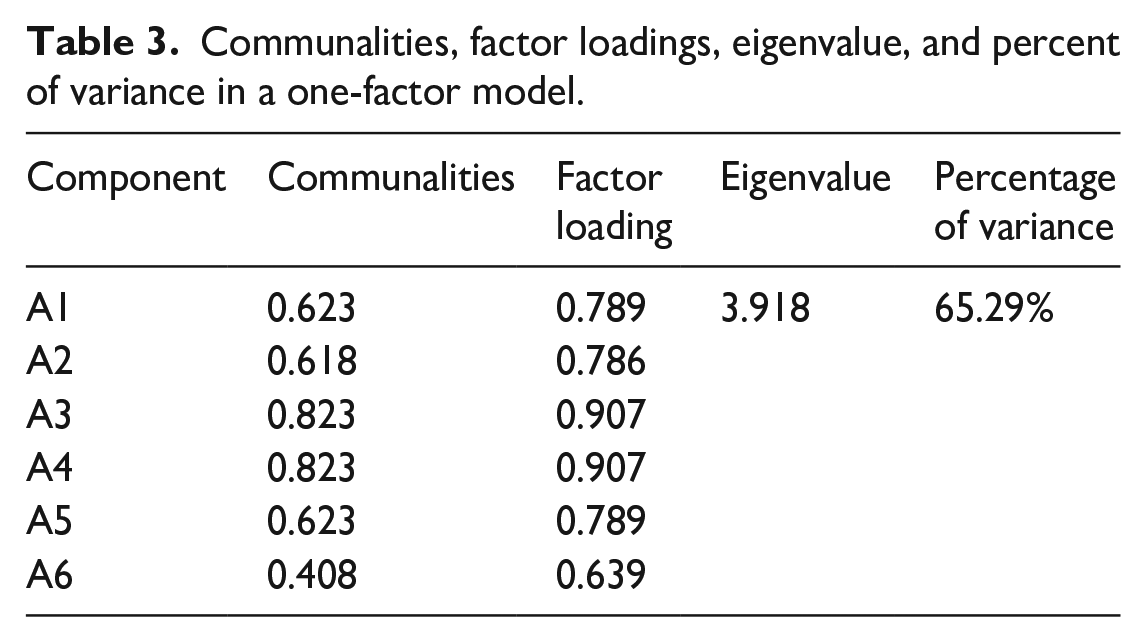
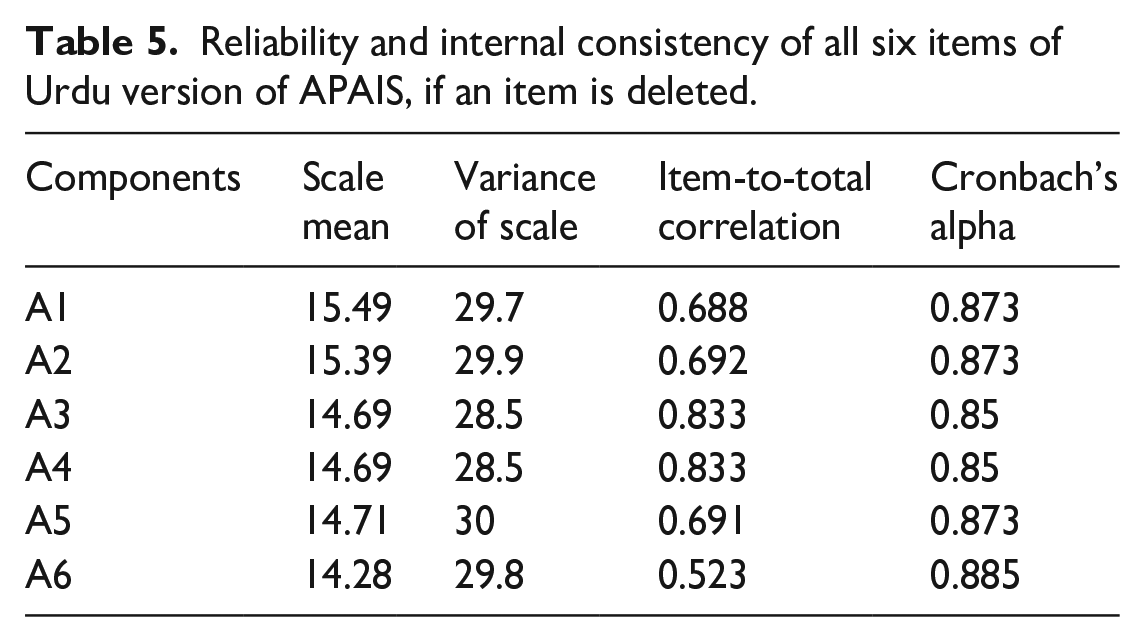
The exploratory factor analysis with an oblique rotation revealed only one factor, which explained a total variance of 65.3% for all scale items (A1–A6) with an eigenvalue of 3.918 (see Table 3). The Cronbach’s α test score for the APAIS anxiety subscale (A1, A2, A4, and A5) and the need for information subscale (A3 and A6) were 0.85 and 0.70, respectively. All items showed an inter-item correlation of >0.20 with a mean value of 0.575 (range:0.349–0.815) (see Table 4). The internal consistency and reliability of each APAIS are reported in Table 5. The mean of total APAIS and VAS-A were 17.85 (±6.47) and 5.9 (±2.7), respectively. The APAIS is strongly correlated with VAS-A (r = 0.664, p < 0.001).
Communalities, factor loadings, eigenvalue, and percent of variance in a one-factor model.
Inter-item correlation matrix.

Reliability and internal consistency of all six items of Urdu version of APAIS, if an item is deleted.
The mean APAIS surgery and anesthesia-related anxiety score was 11.12 (±4.5), and the information desire component was 6.73 (±2.3). Pearson’s correlation showed a significant relationship between APAIS surgery and anesthesia-related anxiety and information desire component (r = 0.767, p < 0.001). The female patients were more anxious as compared to males (t = 2.640, p < 0.01) (see Table 6). As regard, employment status, students, and homemakers had a significantly higher level of anxiety compared to the lowest level of anxiety among salaried individuals (F = 3.836, p < 0.05). The patients undergoing major surgery showed higher anxiety scores in comparison to those having minor operations (t = 2.105, p < 0.05). In addition, the desire for information was higher in patients scheduled for major surgical procedures (t = 2.372, p < 0.05).
Mean APAIS anxiety score, mean APAIS information desire score, and their relationship with study variables.
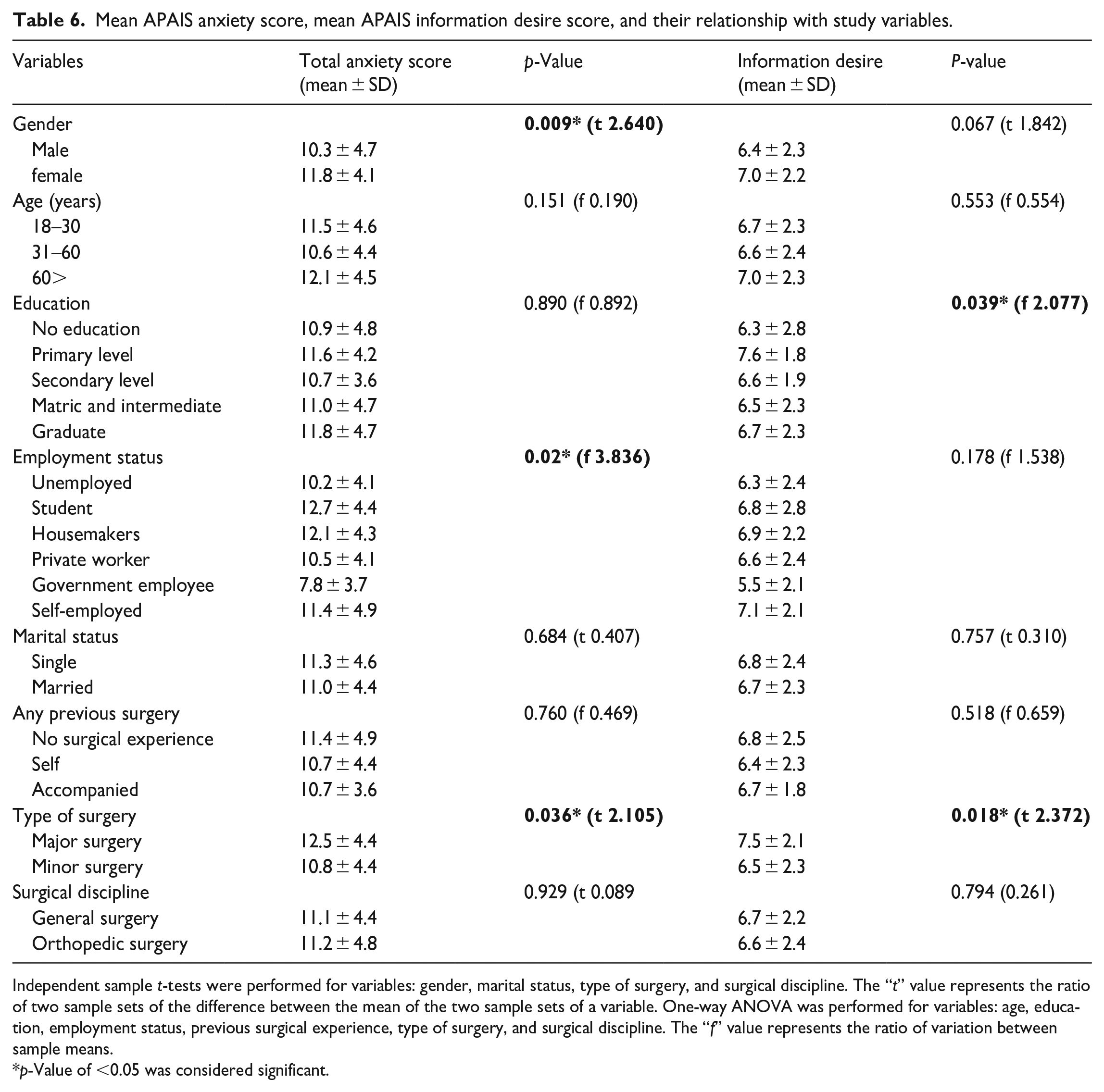
Independent sample t-tests were performed for variables: gender, marital status, type of surgery, and surgical discipline. The “t” value represents the ratio of two sample sets of the difference between the mean of the two sample sets of a variable. One-way ANOVA was performed for variables: age, education, employment status, previous surgical experience, type of surgery, and surgical discipline. The “f” value represents the ratio of variation between sample means.
p-Value of <0.05 was considered significant.
The fear of postoperative pain 140 (52.4%) was found to be the most common cause of anxiety. Reportedly, 115 (43.1%) had a fear of death, 108 (40.4%) had a fear of postoperative paralysis/loss of function, and anxiety-related financial burden was reported by 91 (34.15%) patients (see Figure 1). Only 19 (7.1%) participants were anxious because of concerns regarding the hygiene/sterility of the operation theater and instruments.

Factors contributing to preoperative anxiety among patients undergoing surgical procedures.
Discussion
In this study, we evaluated the level of preoperative anxiety among patients undergoing orthopedic or general surgery procedures using APAIS. Besides the APAIS, multiple instruments are available to measure the level of anxiety, such as State-Trait-Anxiety-Inventory (STAI), VAS-A, and Anxiety Specific to Surgery Questionnaire.19,21,22 Among them, STAI is currently taken as the gold standard for assessing anxiety levels, and the majority of preoperative anxiety studies conducted in Pakistan have used it. However, in clinical settings in a preoperative situation, such an extensive questionnaire may not be applicable.15,23 Furthermore, previous studies have shown a reasonable correlation between the anxiety outcome of STAI and the APAIS scale.15,23 Therefore, through this study, we have introduced and tested the Urdu version of the APAIS scale and performed an evaluation of its psychometric properties. The reliability and internal consistency result not only fulfilled the expected criteria but also compared to Japanese, English, Sri Lankan, and Dutch versions of APAIS.9,11,14,24 In contrast to our expectation, the exploratory factor analysis in our study yields only one factor which does not align with the result of the original study. 9 However, the Spanish version of APAIS also illustrated only one factor in the exploratory analysis. 25 According to our supposition, the high correlation between the APAIS anxiety subscale and the need for information subscale in our study may be the main reason behind obtaining only one factor in exploratory analysis. The criterion validity was assessed by correlating Urdu-APAIS with VAS-A which showed good efficacy. The main reason behind using VAS-A for comparison is that the scale is less time-consuming and reliable in reporting anxiety in a patient with low language comprehension or inability to read.15,18 Also, the unavailability of Urdu STAI is another reason. In pilot testing of the Urdu version of APAIS, all participants rated good to the clarity and acceptability of the Urdu version of APAIS.
The overall prevalence of preoperative anxiety reported in our study was 52.4% (n = 146), as suggested by the APAIS cutoff score of more than 11. 14 The findings of our study indicate that the majority of participants experienced a high level of preoperative anxiety. Similar higher frequencies have been observed in previous researches conducted in developing countries such as Mexico (76%), Ethiopia (61%), Sri Lanka (76%), and India (58.1%).12–14,16 The main factors that contribute to high anxiety levels in developing countries like Pakistan are lack of communication between doctors and patients, low levels of healthcare knowledge among patients, and minimal trust in doctors. The study conducted by Nikumb et al. 26 highlights that the establishment of effective communication channels between healthcare providers and patients, incorporating transparent discussions regarding surgical procedures, prioritizing patient satisfaction, and attentively addressing patients’ concerns and inquiries, can significantly reduce anxiety levels. 26 However, in Pakistan, due to a substantial lack of primary and secondary healthcare settings, the majority of patient bulk gets diverted toward tertiary care hospitals. 27 Doctors here have to deal with a high patient load in a limited time, and trying to provide treatment to all patients sometimes may not satisfy the concerns and queries of each individual regarding their planned procedure. Our study showed a strong association between the need for information requirements and high anxiety levels. In the study conducted by Jawaid et al. 28 in Pakistan, a comparable viewpoint was noted. Approximately half of the study population expressed the belief that acquiring more comprehensive information about their procedure would be conducive to reducing anxiety. Another factor that could contribute to higher anxiety levels in our study is a timepoint of assessment of preoperative anxiety. The anxiety level was assessed before entering the operating room in our study. According to previous studies, the level of anxiety increases in patients at different timepoints with the highest noted before entering the operating room. 29
Several sociodemographic variables contribute to anxiety among patients depending upon regional differences. In our study, generally, females were found to have higher preoperative anxiety levels, compared to males, in line with other published studies.9,13,14,30 We also observed that employment status impacts the level of anxiety which is inconsistent with the results of the majority of studies13,14,23 except in a few.9,31 The reason for this inconsistency can be attributed to the fact that the majority of our study population are laborers or self-employed earning daily wages, which results in an economic crisis due to days off work. Furthermore, due to the lack of a national health program/facility, availing of a medical facility causes a financial burden on patients. Hence, pondering about surgical expenses, days off work, and fear of losing a job are factors that induce anxiety among these patients, as our study and Jawaid et al. 28 noticed that financial loss is one of the most common shared reasons for anxiety among study participants. Furthermore, in our study, housemakers exhibit higher anxiety than any other type of occupation. Notably, this anxiety was found to be more closely associated with the gender variable rather than employment status, as a greater proportion of housemakers were women in our study. Our study showed a significant association between anxiety and the grade of surgery (minor and major), which confirms the results of the previous research.11,23,30
Most factors (education, age, marital status, and previous surgical experience) evaluated in our study had no statistically significant effect on preoperative anxiety. There is a prominent variation illustrated by different preoperative anxiety studies on the significance of these variables. Mulugeta et al., 13 Matthias et al., 14 and Homzová et al. 31 found that previous surgical experience could play a role in reducing preoperative anxiety level, whereas it contradicts the findings of Wu et al. 15 and Nigussie et al. 21 The relationship between previous surgical experience and the anxiety level among patients is partially dependent on the nature of previous surgical experience. 31 An anxiety level can be exaggerated more in patients with negative previous surgical and anesthetic experiences than the patients with positive experiences. 32 That is why the contrasting outcome of anxiety was observed among studies with respect to previous surgical experience. Similarly, inconsistent findings for the impact of age, education, type of surgery, and marital status on preoperative anxiety have been noticed in previous studies.13,14,21,23
Among factors contributing to anxiety, issues related to surgical procedures were observed prevalent in our study, such as fear of death, postoperative pain, not waking up after completion of the procedure, paralysis/loss of function, and disfigurement/cosmetic concerns. Some of these factors have also been highlighted in previous studies.13,30 Our study revealed that the self-reported Urdu-translated version of APAIS is a valid and reliable tool that can be implemented in Pakistani hospital settings in the future to assess preoperative anxiety. To overcome the preoperative anxiety problem, a fruitful strategy could be the provision of general information related to anesthesia and surgery either verbally or through informational leaflets to patients. 8 Besides interviews and communication with healthcare providers, a lot of other pharmacological and non-pharmacological interventions have been demonstrated a positive outcome in treating preoperative anxiety. Pharmacological treatments include common sedatives and anti-anxiety drugs such as Midazolam, diazepam, ketamine, and fentanyl, etc. 33 ; however, this treatment exhibits some drugs induce adverse effects such as respiratory depression, excessive sedation, and alteration in pharmacokinetics of anesthetic drugs, etc. Hence non-pharmacological interventions are commonly preferred over pharmacologic ones by healthcare professionals in both pediatric and adult anesthesia procedures to reduce anxiety. 34 The common non-pharmacological treatments are cognitive and behavioral therapies, religious or spiritual activity, music therapy, visits from relatives, acupuncture, guided imagery relaxation therapy, and massage. 34 All these therapies showed promising outcomes in terms of reducing anxiety.
Limitations
Although this study develops and evaluates the psychometric properties of the Urdu version of APAIS and assesses the prevalence of preoperative anxiety by it, there are some limitations in the study. One is that the anxiety level was assessed preoperatively immediately before entering the operating room. It is possible that preoperative anxiety varies at different instants in the timeframe from hospital admission to the operating table. Our study did not report a level of anxiety at different moments. Second, because of the unavailability of an Urdu-translated STAI scale, we are unable to correlate the Urdu version of APAIS with STAI, which may hamper the evaluation of appropriate external validity and the determination of its optimum cutoff among the Pakistani population.
Conclusions
An Urdu-translated version of APAIS is a valid and reliable tool for assessing preoperative anxiety among patients undergoing surgery in hospitals in Pakistani settings. In our study, the prevalence of preoperative anxiety was very high (52.4%). The independent variables such as gender, employment status, and type of surgery are found significantly related to preoperative anxiety. Fear of postoperative pain, death, paralysis, and financial burden were found prevalent factors contributing to preoperative anxiety.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231208264 – Supplemental material for Psychometric evaluation of Urdu-translated Amsterdam preoperative anxiety and information scale and assessment of preoperative anxiety in adult surgical patients of Karachi, Pakistan: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121231208264 for Psychometric evaluation of Urdu-translated Amsterdam preoperative anxiety and information scale and assessment of preoperative anxiety in adult surgical patients of Karachi, Pakistan: A cross-sectional study by Anoosh Farooqui, Omer Bin Khalid Jamil, Muhammad Muhib, Ayesha Shahid, Aafia Maqsood, Areeba Lari and Aqsa Ismail in SAGE Open Medicine
Footnotes
Acknowledgements
We want to acknowledge Dr Mobeen Shoaib and Amna Muhammad Ahmed for their support in the data collection process.
Author contribution
Anoosh Farooqui: Conceptualization and final draft making. Omer Bin Khalid Jamil: Oversaw the project administration and supervision conceptualization. Muhammad Muhib: Conceptualization, study instrument making, and statistical analysis. Ayesha Shahid: Discussion writing and final draft making. Aafia Maqsood: Data collection, data interpretation, and proofreading. Areeba Lari and Aqsa Ismail: data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from “The Institutional Review Board (IRB) of United Medical And Dental College, Karachi” (reference: UMDC/Ethics/2021/06/29/281) and conducted according to the ethical principles of the Helsinki Declaration.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A written informed consent was taken from every participant of the study prior to filling out the questionnaire. Filling out the consent form was mandatory for every participant. For those patients who cannot read (no education), the study investigator read out the consent form for them and explained all points of the consent form. If they agree to participate, they have to put a thumb impression on the signature column of the consent form.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.