
Abstract
The global refugee community, including those forced to flee due to persecution, conflict, or violence, faces significant challenges in accessing healthcare, resulting in a higher prevalence of surgical disease. These challenges have a profound impact on morbidity and mortality rates, particularly in low- and middle-income countries where many immigrants seek refuge. Limited availability of medical facilities, an inadequate surgical workforce, financial constraints and linguistic and cultural barriers all contribute to reduced access to healthcare. Limited access to competent healthcare leads to poor health outcomes, increased morbidity and mortality rates and suboptimal surgical results for refugees. To address these challenges, a multifaceted approach is necessary. This includes increased funding for healthcare initiatives, workforce recruitment and training and improved coordination between aid organisations and local healthcare systems. Strategies for managing surgical conditions in the global refugee community encompass the development of targeted public health programmes, removing legal barriers, establishing healthcare facilities to enhance surgical access and prioritising disease prevention among refugees.
Introduction
Driven by the imminent threats of violence, conflict and persecution, the global refugee population represents one of the most vulnerable communities in the world. 1 Despite ongoing diplomatic and global efforts for conflict resolution, the number of refugees continues to rise daily. According to the most recent United Nations High Commissioner for Refugees (UNHCR) data, the total number of refugees worldwide is anticipated to be 35.3 million. 2 The journey of refugees is often marked by danger, hardship and uncertainty. In addition to the emotional and psychological impact of displacement, refugees face a multitude of challenges as they navigate their displacement. These challenges encompass inadequate access to healthcare, substandard living conditions and limited resources.3,4 Such circumstances contribute to a higher prevalence of surgical disorders among the refugee populace, exacerbating their already vulnerable health status.5–7
Surgical diseases pose a significant burden on global morbidity and mortality, with a pronounced impact in low- and middle-income countries (LMICs), where many refugees seek asylum. 8 The existing challenges faced by refugees in accessing adequate surgical care are further compounded by the limited availability of prompt emergency interventions, limited interaction with qualified healthcare professionals and a multitude of legal barriers.5–8 Additionally, various barriers comprising language and cultural barriers, financial limitations, a scarcity of healthcare institutions and discriminatory practices further impede and restrict surgical healthcare access.5–10 The experience of displacement also gives rise to a unique set of health issues, including traumatic injuries and an elevated risk of infectious diseases.
Consequently, addressing the healthcare needs of refugees and improving surgical care in refugee settings requires a multifaceted approach. This approach involves increasing funding for healthcare programmes, improving training and retention of healthcare workers and fostering coordination between humanitarian organisations and local healthcare systems.11,12 By addressing these challenges, it becomes possible to alleviate the burden of surgical diseases and improve the overall health outcomes of the global refugee population. Thus, this review aims to explore the impact of various factors on the burden of surgical diseases among refugees and identify potential strategies for improvement.
The refugee crisis and unmet surgical needs
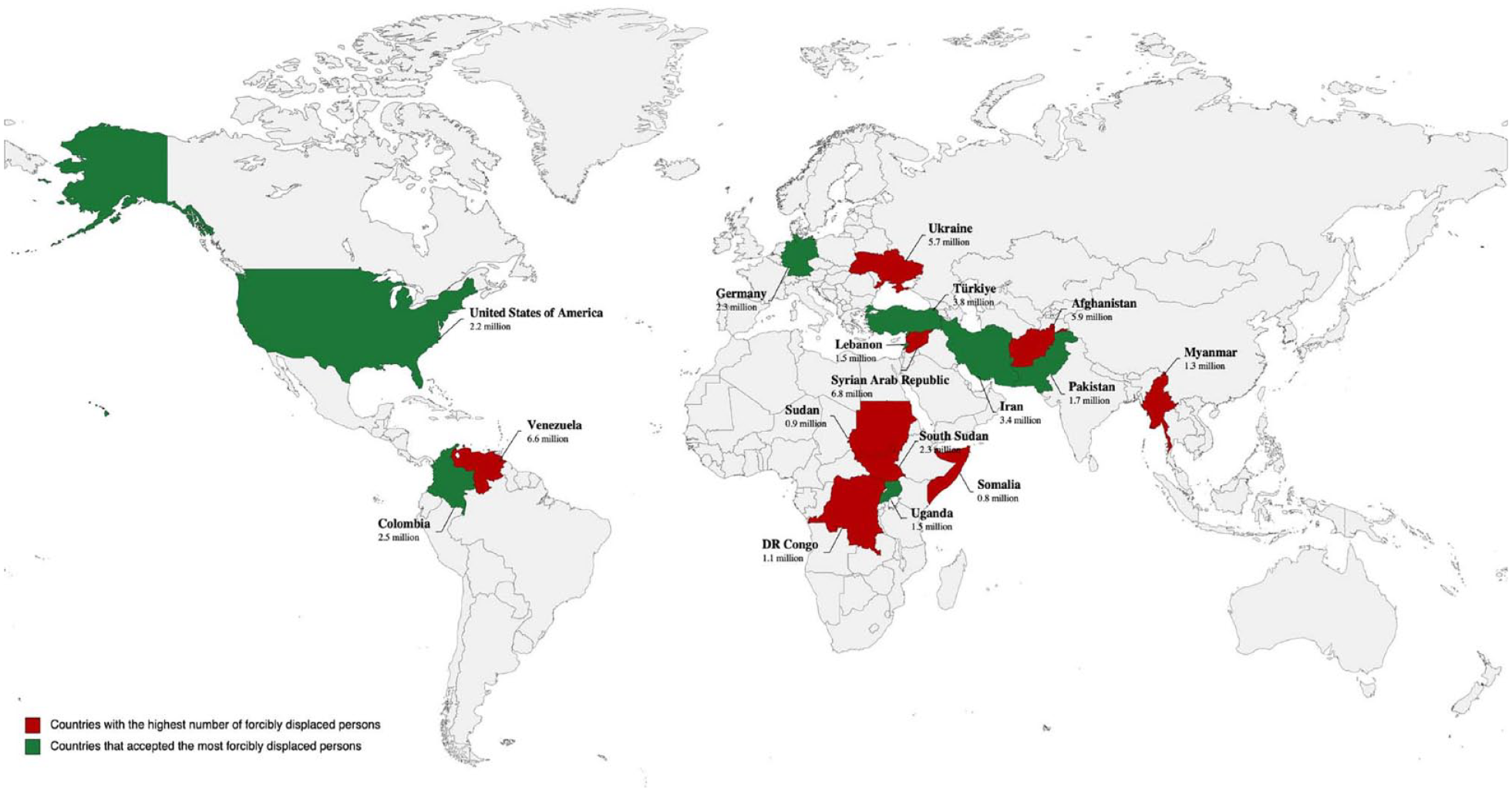
According to the UNHCR, the top three sources of refugees under the global mandate for international protection include the Syrian Arab Republic (6.8 million), Venezuela (6.6 million) and Afghanistan (5.7 million). 2 These nations contribute significantly to the total number of refugees worldwide. Refugees predominantly seek shelter in neighbouring countries. Accordingly, the primary hosts for refugees are Turkey (3.8 million), the Islamic Republic of Iran (3.4 million) and Colombia (2.5 million). 2 These nations hold a substantial portion of the global refugee population. Lebanon distinguishes itself by hosting the most substantial number of refugees per capita and per square kilometre globally. 13 The government’s estimate approximates 1.5 million Syrian refugees and an additional 13,715 refugees from other nationalities. 13
For a comprehensive view of the countries from which refugees originate and their corresponding host nations, refer to Figure 1.
The concerns and challenges faced by different refugee populations are influenced by various factors intrinsic to their circumstances. Factors, such as the cause and duration of displacement, the legal policies of host countries and individual circumstances, contribute to distinct sets of concerns among varying refugee groups. However, several challenges persist, including a lack of basic necessities, limited access to education and employment opportunities, mental health issues, discrimination and stigmatisation. 14 Other shared difficulties encompass family separation, obstacles in accessing legal protection and documentation, limited employment rights and constrained prospects for long-term solutions, including resettlement and integration. 14 These challenges emerge from experiences of displacement, inadequate living standards and restricted access to healthcare. 3 Moreover, children of refugees and those born in refugee camps face increased risks of physical, behavioural and developmental health issues. 15
For refugees, receiving surgical care is typically onerous due to a variety of institutional concerns, logistical challenges and budgetary constraints. Refugees face approximately double the surgical disease burden compared to non-refugee populations, underscoring a glaring health inequity. 8 In contexts of prolonged displacement, the health needs of refugees gradually converge with those of the non-refugee populations in their host countries. 16 This gradual transition reflects an underlying shift in the health profiles of refugees over time.
Contrary to common perception, the increased surgical burden among refugee populations is not solely attributable to trauma-related conditions. While trauma care is undoubtedly a critical component, refugees’ surgical needs encompass a diverse array of health concerns. These include infectious diseases, non-communicable diseases, obstetric complications and neglected tropical diseases such as hydrocele and elephantiasis.16–18
This dynamic health profile underscores the intricacy of healthcare provision for refugees and accentuates the necessity for flexible, context-specific interventions. Such interventions must account for the evolving surgical requirements of these populations to effectively address their multifaceted healthcare needs.
Obstetric complications
Refugee women and children face unique healthcare challenges, including limited access to reproductive healthcare services. This lack of access can give rise to complications during pregnancy and childbirth, such as obstructed labour or uterine rupture, which may require emergency surgical interventions. Additionally, refugee women may require surgical procedures to address reproductive health issues, including unsafe abortions or obstetric fistulas.16,17
Several studies have underscored the unmet obstetric surgical needs among forcibly displaced individuals.10,19 Estimates indicate approximately 196,000 emergency obstetric procedures were potentially required for forcibly displaced women of reproductive age. 20 Similarly, obstetric complications, such as caesarean deliveries for maternal indications, postpartum haemorrhage and ectopic pregnancies, accounted for approximately 10% of the total minimum surgical need among this population, all of which remained unaddressed (Figure 2). 20 The lack of access to family planning and antenatal care services prior to and during displacement further exacerbates the burden of obstetric care in this population.17,18,21 Furthermore, due to underreporting, these factors likely contribute to an even greater unmet need for obstetric surgical procedures.

Challenges of unmet surgical needs in refugee populations.
Furthermore, resettled refugee women face significant disparities in maternal and perinatal outcomes compared to non-displaced women.22,23 These discrepancies encompass elevated rates of preterm birth, low birth-weight infants, stillbirths and maternal mortality. Studies on East African and Somali refugees in Europe show notably higher rates of obstetric complications, leading to an increased demand for emergency caesarean sections.24,25 Moreover, these adverse effects have enduring ramifications on newborn health and development into adulthood. 26 Impaired maternal care due to fleeing conflict zones results in congenital defects like congenital heart disease, adding to the burden of surgical interventions. 26 Tragically, a substantial number of refugee women lack adequate surgical obstetric care, leading to fatal consequences, with increased rates of maternal mortality among Afghan and Burundian refugees.27,28
Trauma-caused morbidity and mortality
Refugees are disproportionately affected by trauma-related injuries, resulting in substantial unmet surgical needs.8,19,21 This vulnerable population often faces an elevated risk of sustaining severe injuries, including gunshot wounds, shrapnel injuries, burns, fractures, amputations and soft tissue injuries (Figure 2). 19
Recent studies have demonstrated the extent of unmet surgical needs among trauma patients in refugee populations. For instance, a study conducted in a camp of refugees in Lebanon elucidated that many trauma patients required surgical intervention. Surprisingly, only 75% of these patients obtained the necessary surgical care, despite the high demand. Seven similar findings were observed in a study performed in a camp for Sudanese refugees: more than 25% of patients in need of surgery did not receive adequate treatment. 19
Refugees frequently assume precarious employment in high-risk sectors with inadequate safety measures. 29 This places them at higher risk of experiencing physical injuries and trauma, consequently increasing the demand for surgical healthcare services. 29 For instance, a study focusing on Syrian refugees in Lebanon found that a significant 31.4% of refugee workers reported work-related injuries. Among these, approximately one in five injuries (19.8%) required immediate surgical attention. 30 A comparable trend of occupational injuries was observed in studies conducted in Canada, where refugees demonstrated a higher incidence of work-related musculoskeletal injuries and illnesses compared to their Canadian-born counterparts. 31 This reiterates the pervasive trend of higher health risks among the refugee workforce due to occupational hazards.
Furthermore, literature has demonstrated a higher prevalence of surgical needs among refugees compared to the general population, often due to the trauma and injuries experienced during conflict and displacement. 21 The susceptibility of refugees to injuries has been substantiated by a recent study examining trauma-related injuries in both local residents and refugees, revealing a significant proportion of these injuries occurring among refugees. 32 A further finding that highlights the unmet surgical needs despite the surge in demand for trauma-related operations is that migrants are more likely to suffer from post-traumatic impairment. 32 Collectively, the existing body of research consistently supports the notion that refugees have a higher prevalence of unmet surgical needs compared to the general population.
Infectious diseases
Addressing the surgical needs of refugees in the context of infectious diseases presents a pressing challenge. The high prevalence of diseases including human immunodeficiency virus, hepatitis B, hepatitis C and tuberculosis (TB) among populations of refugees poses a major concern (Figure 2).4,33 These infectious diseases usually have adverse sequelae that require surgical treatment. Moreover, the current state of unmet surgical needs among refugees exacerbates an already challenging situation.34,35
TB serves as an example of an infectious disease requiring surgical intervention. Refugee populations, residing in overcrowded and unsanitary conditions, face increased susceptibility to TB contraction.4,33 Inadequate and delayed medical attention may precipitate severe complications, including lung abscesses or tuberculous empyema.4,33 Consequently, surgical interventions, conducted by specialised personnel and multidisciplinary teams (MDTs), play a critical role in management. However, persistent scarcity of essential resources and qualified personnel hinders the capacity to address these vital surgical needs.8,20,36 Multiple studies have underscored the existence of unmet surgical needs among vulnerable refugees afflicted by infectious diseases.11,37 The lack of surgical resources perpetuates a cycle of vulnerability, with refugees enduring the devastating impacts of infectious diseases such as septic shock, poor wound healing, prolonged hospital admission and higher rates of morbidity and mortality.8,36
Challenges in managing surgical diseases in global refugee populations
Limited healthcare facilities and specialised surgical centres
Many governments do not value the health of refugees; hence, there are few or no healthcare facilities and services dedicated to this population. According to Kaya et al. 38 and Tayfur et al., 39 the few hospitals and healthcare facilities in refugee-hosting areas occasionally observe equipment, skilled personnel, medical supplies and pharmaceutical shortages (Figure 3). The inability to consistently access energy and water owing to inadequate distribution centres makes it difficult to achieve the required degree of hygiene and sterilisation. 7

Challenges in managing surgical diseases in global refugee populations.
While managing medical conditions is crucial, it is also essential to prioritise surgical diseases, as they often require prompt treatment to significantly improve patient outcomes. Patients who do not receive timely surgical interventions for their conditions experience severe disability and a diminished quality of life. Furthermore, untreated surgical conditions can result in increased healthcare costs and financial burdens on individuals and society as a whole (Figure 3).5,40 An example of the consequences of inadequate surgical facilities is observed among Rohingya refugees from Myanmar in Bangladesh, where a lack of proper surgical care has led to preventable deaths and disabilities. 5 Similar challenges are faced in Lebanon, where the healthcare system is fragmented and inequitable. 40
Access to specialised healthcare for refugees largely depends on their location and healthcare infrastructure. 8 Referral healthcare, necessitating travel to remote medical facilities, commonly presents significant obstacles for refugee populations. These include financial burdens, safety concerns and fragmented continuity of care. 41 Additionally, cultural and linguistic obstacles experienced at these referral points further compound the intricacy of this situation. The absence of standardised referral protocols can potentially result in protracted delays or outright denials of care, thereby exacerbating health disparities. 41 A comprehensive understanding of these impediments is indispensable for the enhancement of health outcomes among refugee populations. The assessment of these challenges provides the foundation for the development of tailored healthcare strategies and interventions.
Financial constraints, security issues and reliability limitations are among the obstacles faced. Crossing borders and navigating through conflict zones pose significant risks to the safety of refugee populations. 42 The length of time refugees stay in camps varies greatly depending on resource availability, resettlement opportunities, political stability and the duration of the conflict in their home country, with some refugees staying for several decades. Prolonged stays in camps may lead to a decline in overall well-being because of the poor living conditions and limited opportunities for gainful economic activity. This makes it difficult for refugees to support themselves financially and seek relocation elsewhere. Moreover, the lack of healthcare facilities in camps presents challenges for maintaining accurate medical records and providing adequate follow-up treatment (Figure 3).
Inadequate surgical workforce
Successful surgical interventions rely on the collaboration of MDTs, which comprise a range of healthcare professionals who collaborate to establish comprehensive management plans for patients. 43 A surgical MDT typically encompasses specialised nurses, anaesthesiologists, surgical technologists, radiologists, pathologists, psychiatrists and social workers. Each member of the team contributes their unique expertise to address various aspects of patient health, such as pain management, infection control and post-operative rehabilitation. 43 The involvement of such experts is crucial for ensuring the best possible surgical outcomes.
The International Red Cross Organisation is a prominent organisation with highly experienced staff, ample resources and modern facilities dedicated to providing surgical care for vulnerable refugee populations. 37 However, refugee camps continue to face the issue of a severe shortage of healthcare workers (Figure 3). 12 A 2016 study conducted by the Johns Hopkins Bloomberg School of Public Health estimated that 59.5 million displaced individuals globally required 2.78 million surgical procedures. 20 However, a sizable portion of these urgent surgical needs have not been met as a result of several issues, including a surgeon shortage.
Refugee camps, often constrained by their limited size, frequently operate with minimal staff and basic equipment, resulting in a chronic shortage of qualified physicians and surgeons (Kushner et al. 37 ). Moreso, several studies have reported a significant dearth in the healthcare workforce, particularly in refugee camps.44,45 Consequently, delivering a standardised quality of care becomes an insurmountable challenge, leaving refugees without access to the level of medical attention available to their counterparts in host countries (Figure 3). 37
Notably, this situation predominantly afflicts LMICs, such as Colombia and Pakistan, both among the top host nations for refugees, harbouring millions of displaced individuals. 2
Financial constraints, both from the health system and the refugee populations
Access to healthcare poses significant financial challenges in many regions worldwide, with operating theatre expenses ranging from $7 to $113 hourly. 46 The majority of refugees and asylum seekers are unable to afford complex surgical procedures and post-operative treatment due to the healthcare system’s budgetary constraints, which also impede the provision of essential medical supplies and equipment. Financial constraints in the healthcare systems of the host nations additionally limit the availability of discounts and subsidies for populations of refugees and prohibit timely access to surgical operations (Figure 3). Furthermore, healthcare disparities exist between migrants, especially refugees, and host communities, resulting in reduced healthcare opportunities for refugees. 6 This may exacerbate health conditions and precipitate a long-term financial burden. Governmental assistance is often inadequate, leaving charitable and non-profit organisations as the primary source of support in refugee camps (Figure 3). However, despite the presence of organisations such as the International Rescue Committee and Médecins Sans Frontières, their capacity to meet the complex healthcare needs of refugees remains limited. These organisations primarily rely on funding from individuals, corporations and foundations, which is often volatile, situational and insufficient. Notably, in 2016, humanitarian appeals coordinated by the United Nations faced a 40% funding gap. 47
Access to public health insurance is restricted by legal regulations for refugees who are unable to afford healthcare expenses (Figure 3). 48 This poses significant challenges as health policies, including legally established health rights, play a fundamental role in determining medical insurance coverage and access to healthcare. However, there has been limited progress in analysing health policies for migrant populations, leaving refugees with inadequate insurance coverage. 49 In countries like France, refugees often remain uninsured due to administrative barriers and economic burdens, rendering them responsible for bearing the full cost of medical procedures. 48 The limited coverage, high deductibles and co-payments add to the financial burden that migrants must shoulder. As a result, migrants usually have to pay for their medical procedures out of pocket. The economic challenges faced by refugees are further compounded by differences in currency rates and the hidden costs associated with currency conversions, particularly when refugees originate from economically deprived regions. 48 These factors create barriers to affording necessary healthcare services. In the context of surgical care, costs are often not transparent and encompass various additional and hidden expenses, thereby intensifying the financial strain on refugees. Furthermore, these financial burdens may exacerbate pre-existing economic disparities among refugee populations. 49
Access to healthcare services, particularly tertiary care, is a multifaceted challenge for refugees, exacerbating existing healthcare disparities and intertwining with socio-economic challenges. Although refugees can avail themselves of healthcare provisions in host nations, equitable access to these services frequently remains elusive. 50 In Jordan, for instance, a $9 consultation fee for tertiary services is imposed on refugees subsisting at or below the poverty line with a daily income of $3, precipitating a disproportionate financial burden. 51 Such burdens, compounded by restricted labour market access, intensify the fiscal strain of healthcare costs. Despite the emphasis on primary care in refugee health policies, funding for tertiary care is often insufficient. 50 Cases like Tanzania highlight the challenges: refugees are frequently excluded from national healthcare schemes, thereby limiting their access to critical referral services. 52 These financial constraints, coupled with logistical and geopolitical obstacles, impede refugees’ access to comprehensive healthcare referrals. Therefore, the overarching issue of equitable healthcare access persists, requiring attention and action in policy planning and execution.
Consequently, migrants grapple with untenable choices, such as resorting to unregulated and potentially hazardous informal care, or postponing crucial surgeries, thereby potentially worsening their existing health conditions. This conundrum is exemplified by the situation of Syrian refugees in Lebanon, where substantial economic barriers have obstructed their access to surgical care. The Lebanese healthcare system’s strain further amplifies Syrian refugees’ financial constraints. 53
In some nations, the hindrance to healthcare access is not solely due to resource scarcity but is significantly influenced by the constraints inherent in the services provided by the UNHCR. 40 For instance, Lebanon accommodates a considerable refugee population and features several hospitals and skilled surgeons proximal to the refugee settlements. However, the cost associated with the healthcare services provided frequently exceeds the financial capacity of the refugee populace. This imbalance precipitates catastrophic health expenditures and perpetuates economic strain.54,55 The ongoing economic crisis in Lebanon and globally exacerbates these challenges by further limiting refugees’ affordability of and accessibility to healthcare services. This adversity also instigates tension with the local inhabitants, who similarly grapple with the crisis but without the benefit of international aid.
The financial and healthcare challenges faced by Syrian refugees in Lebanon highlight the urgent need for policy interventions. According to a study conducted on the Thai–Myanmar border, the establishment of an in-house general surgical service may provide a cost-effective solution to mitigate these burdens. 11 Nonetheless, the geographical limitations and regional concentration of these facilities emphasise the complexities and limitations of the current system. The findings from Kaafarani et al. 54 and Al-Hajj et al. 55 offer valuable insight into the health systems in regions with high refugee populations and underscore the financial challenges faced by refugees. Thus, financial constraints, both from the health system and refugee populations, continue to pose significant barriers to adequate healthcare access, necessitating immediate and efficient interventions.
Cultural and language barriers
Language barriers often pertain in these environments, posing significant challenges to the provision of care, often compounded by cultural differences, including political, religious and cultural nuances. These differences may facilitate disagreements and conflicts between refugees and healthcare workers, weakening trust and cultivating an atmosphere of scorn and distrust, further harming patient compliance with therapies and healthcare delivery (Figure 3). Poor post-surgical outcomes have allegedly been linked to poor patient–physician communication, particularly in cases of orthopaedic trauma. 10 Cultural barriers may also contribute to stigmatisation and discrimination, leading to a reluctance among refugees to seek medical care (Figure 3). Additionally, there is a shortage of interpreters and translators available to assist these refugee populations (Figure 3). 10
Refugees may find it challenging to understand preventative health measures and the management of chronic diseases due to their restricted access to health education resources and information in their home country. It might be arduous for refugees to comprehend how healthcare is provided in the host nation due to language barriers (Figure 3). 56 For example, in Romania, language and legal barriers make it challenging for refugees to understand healthcare-related legal documentation, leading to delays in the registration process for receiving healthcare services. 57 The social acceptance of refugees poses a significant challenge, as native populations may perceive their own members as being neglected in favour of providing shelter and assistance to refugees. This perception may lead to emotions of threat and unease among the native population. 58
The implications of surgical management gaps in refugee populations
Poorer health outcomes: Reduced quality of life, increased morbidity and mortality rates
Insufficient availability of surgical care among refugee populations has profound and far-reaching consequences for their health outcomes. The lack of access to timely and adequate surgical interventions not only leads to increased rates of illness but also escalates the risk of mortality.8,59 The implications of delayed treatment extend beyond immediate health concerns, as they hinder the prospects of long-term recovery and may even render it unattainable.
Due to a shortage of resources, it is challenging to administer urgently needed surgical treatment as the highest priority, lengthening hospital admissions and predisposing refugees to inadequate surgical care.8,36,59 Consequently, unnecessary complications such as deep vein thrombosis, air embolisms and falls arise.8,36,59
The gravity of the situation becomes evident when considering the mortality rates associated with inadequate surgical care. For instance, research indicates a staggering 17% mortality rate among Syrian refugee patients with heart disease, with half losing their lives while awaiting surgical intervention. 60 These numbers highlight the consequences of limited access to surgical interventions in refugee populations.
Poor surgical outcomes: Surgical complications, infections and mortality rates
The scarcity of specialised care within refugee camps significantly hampers the chances of successful surgical interventions, resulting in suboptimal surgical outcomes. A major concern in these settings is the high incidence of surgical site infections (SSIs), which account for significant proportions of hospital-acquired and nosocomial infections among surgical cohorts.33,60 Several factors contribute to the increased prevalence of SSIs in refugee camp settings, including ineffective sterilisation of instruments, improper operation theatre ventilation and suboptimal surgical techniques.4,33 These deficiencies in infection control measures compromise the safety and effectiveness of surgical procedures, leading to a higher risk of complications and adverse outcomes.
The results of intraoperative surgical procedures are also influenced by structured variables such as case volume, time spent in the operating room and blood transfusions. Surgery is challenging since not enough competent medical personnel exist and refugee camps sometimes exhibit high infection rates.4,33 Hence, poor intraoperative and post-operative outcomes result.
Late diagnosis of surgical conditions among refugee populations poses a significant threat, as it can have fatal consequences and contribute to increased morbidity and mortality rates. The delayed identification and management of surgical conditions hinder prompt interventions and compromise the probability of successful treatment and recovery.
Moreover, the impact of surgical management gaps extends beyond general surgical care. Orthopaedic trauma surgery, dialysis provision for patients with end-stage kidney disease and maternal and neonatal health are all adversely affected by the limited access to surgical interventions.8,19 These diverse areas of healthcare highlight the multifaceted nature of poor surgical outcomes in refugee populations.
Economic consequences of surgical management gaps
Limited access to surgical care in refugee populations has significant economic implications. Prolonged disability resulting from untreated surgical conditions facilitates increased healthcare costs.19,59 Patients not receiving timely surgical intervention are more likely to experience complications, requiring additional medical resources and interventions, thereby exponentiating healthcare expenditure.8,20,61 The costs associated with managing these complications, such as extended hospital admissions, medication and rehabilitative services, further strain healthcare systems and increase financial burden.
In addition, unaddressed surgical needs among refugees may have a detrimental impact on workforce participation.8,59 When individuals are unable to receive the necessary surgical intervention, their ability to engage in productive employment is compromised. This not only affects their personal income but also leads to reduced overall economic output for the host communities.8,11 The loss of productivity and workforce potential exacerbates the economic burden on both the affected individuals and the host communities.
The long-term prospects for refugees and host communities are also affected financially. The possibility for patients to restore their full functional capability might be limited by subpar surgical treatment and the ensuing health issues.8,11 The affected and their supporting communities are continually under financial duress as a result of their need for healthcare services and social support networks.
The economic ramifications also include indirect costs, such as the impact on maternal and neonatal health. Studies have shown that refugee mothers experience higher rates of complications during childbirth, including an increased likelihood of caesarean sections, higher rates of anaemia and lower neonatal birth weights. 61 These complications require additional healthcare resources and may have long-term implications for the health and development of the newborns, potentially resulting in increased healthcare costs and reduced economic opportunities in the future.
Management strategies for surgical diseases in the global refugee populations
As previously elucidated, a plethora of factors, including the inadequate availability of healthcare within refugee accommodation centres, the inadequate availability of a surgical workforce, financial constraints and cultural and language barriers, act as detriments, preventing the uptake of surgical treatment amongst this vulnerable cohort of individuals. Consequently, any strategy proposed to tackle refugee health inequities must not only be multidisciplinary, taking into cognizance all of the above-mentioned detriments, but must also be meticulously devised and suited to tackle the needs of a vast population of refugees in line with current trends.
Devising an appropriate public health strategy
Firstly, any attempt to improve surgical health outcomes for refugees should stem from a firm political resolve combined with a meticulously devised strategy. Fostering political resolve can help to catalyse action, drive policy change and secure the necessary resources and funding for surgical interventions. 62 However, a carefully planned strategy might guarantee that efforts taken to improve refugee health outcomes are evidence-based, situation-specific and sustainable. Political resolve can help to catalyse action, drive policy change and secure the necessary resources and funding for surgical interventions (Figure 4). 63 This may help guarantee that the target population receives the care and assistance required to overcome the many obstacles they face.

Management strategies for surgical diseases in the global refugee population.
The first step to devising an apt public health strategy to improve surgical outcomes is conducting a comprehensive ‘needs assessment’ of unmet surgical needs among refugees (Figure 4). This collaborative effort often involves central governments, public health officers, non-governmental organisations, healthcare providers and international humanitarian organisations. The assessment should examine the prevalence and burden of surgical diseases within the refugee population, as well as the availability and accessibility of surgical health services. Furthermore, it should also evaluate public health risks, including the outbreak of communicable diseases, the nutritional status of refugees, immediate health requirements and social barriers to healthcare use. These assessments serve multiple purposes, ensuring that surgical care is evidence-based, tailored to population needs and sensitive to social norms. 64
Following the needs assessment, the next step is to engage in a comprehensive discussion involving all relevant stakeholders. 64 These stakeholders may include representatives of refugee organisations, non-governmental bodies, charities, public health departments, healthcare providers and government officials. Such discussions enable diverse perspectives and allow each party to express their concerns, viewpoints and priorities regarding the situation. By fostering a shared understanding of the context and realities, these discussions ensure that the strategies and interventions developed are responsive to the specific needs and challenges faced by refugees. Engaging a wide range of stakeholders not only promotes effective coordination and implementation but also facilitates consensus and support for the recommended techniques and actions.
Widening access to health and surgical care
Access to healthcare is widely regarded as a fundamental right. However, in many nations, the political setup and framework of law mean that refugees and asylum seekers are not entitled to the same benefits as citizens and residents with legal status domiciled in the nation. Even in countries that do provide healthcare provisions, numerous obstacles persist, impeding access to life-saving surgical treatment. These include language and cultural obstacles, a lack of access to healthcare facilities and professionals, financial constraints, transportation issues, a lack of understanding of available healthcare services and a fear of discrimination or persecution. Consequently, refugees experience delays, inadequate treatment, increased health concerns and a lower quality of life. As a result, governments and related stakeholders must address these challenges and implement policies and programmes that foster equitable access to surgical treatment for refugees.
Removing legal barriers to surgical healthcare
At the governmental and central levels, a major step towards improving surgical outcomes for refugees is the removal of restrictions, barriers and other impediments that prevent their access to surgical treatment. Many nations incorporate policies that not only limit refugees’ access to healthcare, including surgical care, but also aim to discourage refugee inflow and relieve strain on already overburdened healthcare systems. 8 Such approaches, however, are counterproductive and fail to address refugees’ urgent and long-term health requirements (Figure 4). To ensure equitable access to surgical treatments, governments and stakeholders must collaborate to remove these barriers and develop regulations that allow refugees to receive treatment without fear of prejudice or persecution. Laws must be implemented to guarantee refugees’ access to expertise and surgical care. Civil society organisations and concerned parties must actively advocate, persuade and encourage governments to amend their laws and allocate funding to ensure that refugees have access to medical treatments, particularly in the field of surgery. Working with legislators to establish and implement policies that address refugee health and surgical needs, while also engaging with local communities to raise awareness and foster acceptance of refugees and their healthcare requirements, are important steps towards achieving this goal.
Targeted healthcare interventions and the setting up of healthcare institutions
Following a needs assessment, targeted surgical health interventions tailored to the specific needs of the refugee population can significantly improve their health outcomes. An apt example of such an intervention is the establishment of mobile surgical units. 65 These self-sufficient units are equipped with advanced technology, instruments and skilled staff with surgical expertise. Their mobility allows for easy relocation and the provision of a wide range of surgical services, including emergency caesarean sections, hernia repairs, fracture treatments and trauma surgeries. Another effective targeted intervention is the training and deployment of community health workers (CHWs). 66 In densely populated refugee camps and a broader surgical context, CHWs play a crucial role in providing first aid, triaging patients and identifying those requiring urgent referral and surgical interventions. In addition, CHWs can conduct public health education programmes to promote basic health practices, hygiene awareness and preventative measures, thereby reducing the overall incidence of disease (Figure 4). In all such endeavours, the use of interpreters should be encouraged to overcome language barriers.
The establishment of healthcare centres within refugee camps offers a significant improvement in refugees’ access to surgical care. By constructing healthcare facilities within refugee camps, refugees are able to receive timely and adequate surgical care without the need to travel long distances. This is particularly beneficial for refugees with limited mobility or financial resources, as it removes barriers to accessing healthcare outside of the refugee camps. Additionally, healthcare institutions within refugee accommodations can employ healthcare professionals who are specifically trained to work with refugees and are familiar with the population’s cultural and linguistic needs. This promotes better communication and understanding between healthcare providers and the refugee population. Furthermore, healthcare facilities within refugee accommodations can adopt a holistic approach to healthcare by addressing the social and economic determinants of health. Alongside surgical interventions, these institutions can educate refugees on lifestyle choices, nutrition and hygiene practices while also providing mental health support to help them cope with the trauma of displacement and other problems they may face.
Prioritising disease prevention among global refugee populations
Finally, prioritising public health preventative measures is crucial for significantly improving surgical health outcomes for refugees. Empirical evidence over the past two decades has highlighted several instances of epidemic outbreaks in refugee populations and settlements. For instance, a retrospective study analysing the outbreak of infectious disease in refugee populations revealed that between 2009 and 2017, a total of 364 disease outbreak instances were noted in 21 countries. 67 Therefore, disease prevention measures are essential to overcome health inequities in refugee cohorts.
One key preventive measure is immunisation, as many refugees come from countries where vector-borne diseases are prevalent and access to vaccines is limited. 68 Ensuring comprehensive immunisation campaigns targeted at specific age groups and countries of origin can provide protection against diseases such as measles and tetanus, potentially reducing the need for future surgical interventions (Figure 4).
Additionally, sanitation and hygiene measures play a vital role in preventing outbreaks of diseases like cholera, dysentery and typhoid fever. 69 Supplying health and hygiene products and facilitating access to clean sanitation facilities are essential components of these efforts (Figure 4).
However, the delivery of interventions alone is insufficient without effective public health education and awareness campaigns. Raising awareness among refugees about available interventions and surgical treatments within the refugee accommodation sites is crucial for encouraging treatment uptake and improving health outcomes. Moreover, broader refugee awareness campaigns aimed at the general public can help combat stigmatisation and discrimination against refugees.
Furthermore, involving the refugee community and its leaders in the planning and execution of healthcare interventions is critical. This engagement facilitates a better understanding of the unique healthcare needs influenced by cultural and language factors. By incorporating cultural relevance and respect for individual views and values, healthcare solutions can be more effective and yield improved outcomes.
Limitations of study
It is important to acknowledge the limitations of this narrative review. The heterogeneity of refugee populations, stemming from a variety of backgrounds and circumstances, could potentially limit the generalisability of our findings due to their significantly varied healthcare requirements. The constantly evolving nature of refugee situations, marked by changing displacement dynamics and inconsistent healthcare access, further complicates the inclusivity of relevant studies.
Despite our efforts to include a representative selection of studies, the scope of our review might not have encompassed all interventional strategies or policy recommendations that address the complex surgical needs of global refugee populations. Moreover, the ethical dilemmas associated with delivering surgical care in refugee settings may require a more thorough examination.
Furthermore, the findings presented here may not comprehensively cover the entire domain under scrutiny, warranting caution in the interpretation and formulation of interventions or policy recommendations. The absence of standardised data could introduce bias and obstruct a comprehensive understanding of the surgical needs of refugees worldwide. While we acknowledge the presence of cultural and language barriers, a more in-depth analysis of their impact on disparities would be beneficial. Additionally, the incorporation of non-surgical healthcare requirements could potentially obscure the specific challenges related to surgical care among refugees.
Conclusion
The prevalence of surgical illnesses among global refugee populations is high, and their treatment is impeded by various barriers. Inadequate healthcare facilities, a lack of specialised surgical centres, a shortage of skilled surgical professionals, financial constraints and cultural and language barriers all contribute to the complexities of addressing surgical needs in this vulnerable community. However, addressing these challenges is not only a matter of humanitarian concern but also a critical public health imperative. Timely and adequate surgical therapy may prevent long-term disability, reduce healthcare costs and improve overall health and well-being. To address these issues, it is imperative to increase the availability of healthcare facilities and establish surgical centres that cater to the unique needs of refugee populations.
Collaboration between local and international healthcare organisations, community engagement and education are vital to resolving cultural and language issues in providing surgical care for global refugee populations. Addressing their surgical needs and striving for equitable and comprehensive healthcare for all individuals, regardless of origin or condition, is of utmost importance.
Footnotes
Acknowledgements
We acknowledge ICORMed Research Collaborative and Toufik’s World Medical Association for their support in data collection and research facilitation.
Author contributions
All authors contributed to the study conception and design. The study was conceptualised and supervised by WAA. Material preparation, data collection and analysis were performed by WAA, FTA, TF, SA, HRB, AAA, JW, MRZ, HK, AK, TA-R and AI. The first draft of the manuscript was written by WAA, FTA, TF, SA, HRB, AAA, JW, MRZ, HK, AK, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.