
Abstract
Introduction:
Healthcare facilities produce a variety of trash that, if handled improperly, could endanger the environment, the health of patients and clients, healthcare personnel, and the general public. Health staff have been given training on infection control and healthcare waste management. It is not apparent whether similar initiatives are taken for sanitary personnel, though. By evaluating sanitary workers’ knowledge, attitudes, and practices about healthcare waste treatment in the Dodoma region of Tanzania, this study sought to clarify the situation.
Methods:
From March to August 2022 in Dodoma, Tanzania, a descriptive cross-sectional study using a quantitative methodology was conducted on 156 randomly chosen sanitary workers. The primary data collection instruments were structured questionnaires that were conducted by interviewers and a trash checklist that the research team created. Statistical Package for Social Sciences computer software was used to conduct a descriptive analysis of the data with a 95% confidence level and a 5% level of significance.
Results:
The average age was 28 ± 6.2 years, and there were 74.4% females. Of all of the health institutions under study, 78.4% of the generated medical waste was non-infectious, whereas 21.6% of it was infectious. The share of non-infectious and infectious healthcare waste created by regional referral hospitals was 43.5% and 13.2%, respectively. While 67.8% of sanitary workers believed that handling healthcare waste was not their problem and 63.6% of sanitary workers actually displayed subpar practices of handling healthcare waste, 74.4% of sanitary workers had low understanding about handling healthcare waste. Their procedures for handling medical waste were substantially influenced by the kind of healthcare facility, sex, education, job experience, knowledge, and attitude (p < 0.05).
Conclusion:
Sanitary staff members had limited understanding and thought they were less concerned with gathering, moving, and storing medical waste. To provide the highest level of health safety, national health policy and facility-based interventions must support and fund participatory waste management training that is tailored to the sociodemographic profiles of sanitary employees.
Keywords
Introduction
Due to its potential harmful health impacts on the environment and people, healthcare waste generation, collection, transportation, storage, treatment, and disposal have recently become a trending concern in public health. 1 Health facilities, laboratories, chemical businesses, pharmaceutical stores/units, mortuary and autopsy centers, animal research and laboratories, blood banks and collection centers, and nursing homes are the main sources of healthcare waste. 2 As stated by Ranjbari et al., 3 5.9 tons of the total 1.47 billion tons of solid waste produced worldwide are thought to be produced in hospitals. Also, the World Health Organization claims 4 and Chisholm et al. 5 estimates, rich countries produce up to 0.5 kg more infectious healthcare waste per hospital bed per day than developing nations do.
Healthcare facilities produce a variety of trash that, if handled improperly, could endanger the safety and health of healthcare professionals, patients/clients, and the general public.6,7 Healthcare facilities include hospitals, clinics, doctor’s offices, dentist’s offices, blood banks, and veterinary hospitals. They also include medical research institutions, but also laboratories. 8 Used needles/sharps, contaminated gloves, masks, caps, aprons, bandages, diapers, and/or human body fluids are among the waste items that might be classified as infectious (15%). The majority (75%–90%) of healthcare waste is non-infectious and may include, but is not limited to, papers (writing pads, toilet paper, and tissue paper), green waste (flowers, tree branches, etc.), used linens, food remnants, wooden materials, syringes, plastic/metal bags, bottles, tubing/catheters, chemical substances, expired drugs/substances, and/or non-functioning medical equipment.5,9
A number of epidemiological and environmental issues, including unpleasant odors, unattractive debris and human body parts, pollution, fire risks, and/or the release of toxic compounds, have been associated with improper handling of healthcare waste. 6 Injuries and the spread of infectious illnesses that affect people, animals, and plants, such as typhoid, diarrhea, cholera, malaria, schistosomiasis, and skin diseases, to name a few, are examples of health-related epidemiological concerns. 10 It appears that the situation calls for high priority and attention to ensure adequate waste creation, segregation, transportation, storage, treatment, and disposal given the infectious nature of incorrect handling of healthcare waste to the environment, humans, animals, and plants. But in developing nations, where evidence suggests that over 80% of created healthcare waste is combined with general waste, the situation is different. 11
The management of healthcare waste generation, treatment, storage, and disposal involves administrative agencies, managers, contractors in healthcare waste handling firms, and other stakeholders close to healthcare institutions.12–14 The national health policy of Tanzania, for instance, has shown that sanitation difficulties have persisted as a public problem of concern that needs to be addressed appropriately despite innovative initiatives against environmental pollution and deforestation. 15 Managers, contractors, or bosses must carry out tasks like hiring sanitary health staff, buying equipment for handling healthcare waste, fostering a healthy and welcoming work environment, acquiring personal protective equipment, and guaranteeing and processing payments to their employers in order for healthcare waste handling to be effective.
Literature2,9,10,16 has shown that using sustainable waste handling techniques can help minimize the negative effects inappropriate healthcare waste treatment would have on the environment and human health. For both public health safety and environmental hygiene, sustainable solutions that advocate and promote, for example, the practices and process of renewing healthcare waste are highly encouraged worldwide.17,18 The strategies, however, appear to vary significantly between nations around the world, and it has been reported that these strategies are much more advanced in developed nations than in developing ones, where it is very difficult to separate waste into infectious and non-infectious materials on your own.19–21 Healthcare waste disposal appears to be a bigger problem in poor countries than it is in the developed world due to disparities in health systems and organizational structures.5,22
Due to the high turnover of healthcare workers in Tanzania’s healthcare system, health facilities are currently hiring auxiliary health workers, community-based units, and/or independent non-governmental organizations/groups to collect healthcare waste and transport it to disposal sites, in this case, dumping/burning sites and/or incinerators located on the premises of health facilities.9,23,24 Given the contract with the healthcare institution, the hired sanitary organizations or community-based organizations are responsible for hiring sanitary personnel in accordance with the predetermined recruitment criteria and developing a healthcare waste handling plan for prompt waste disposal. 25 Sanitary personnel gather and move medical waste from the source to disposal locations or incinerators using tools including wheelbarrows, wheel buckets, crates, and/or plastic bags. 14 Depending on the pace of healthcare waste generation and timetable, the processes may be performed daily or weekly. 26
Sanitary employees have gotten close to problems including the gathering, transportation, storage, treatment, and disposal of solid waste from sources including healthcare facilities despite being removed from the generation of healthcare waste. 25 Cleaning, maintaining, running, or emptying the machinery at any stage of the sanitation chain is the responsibility of sanitation employees, who are integral to health activities in healthcare institutions. 27 In developed nations, it may become more evident to see sanitation workers take classes and/or short courses on how to properly dispose of medical waste as a tactic to equip them with the knowledge, attitude, and skills necessary to protect themselves, other healthcare workers, patients/clients, and the community at large from health risks and compromised safety.25,28 Tanzania is one of the poor nations where efforts have been made to train healthcare professionals in infection prevention and control techniques as well as related activities, but the situation there remains mute. 29
During their formal education, seminars, professional conferences, and on-the-job training, healthcare professionals receive formal instruction in infection prevention and control measures. 30 Clinical real-world experiences show that healthcare professionals perform better when waste segregation processes are their main responsibility for the process of infection prevention and control.31,32 Yet, because of problems with an increased rate of retirement, turnover, and/or academic career progression, it has been difficult to train and keep them in healthcare facilities. 33 Due to the circumstances, a task-shifting technique has been used, and other auxiliary health workers, such as sanitary workers, are now responsible for tasks including transporting, storing, processing, and disposing of medical waste. 25 It is unclear in the country whether auxiliary healthcare workers, such as sanitary workers, are trained on infection prevention and control strategies in their working stations for healthcare waste handling knowledge, attitude, and practice, despite the fact that they are responsible for handling healthcare waste in healthcare facilities.
It raises questions about whether sanitation staff are knowledgeable of and have a positive attitude toward using healthcare waste properly. A number of academic papers31,34–36 have concentrated on and disseminated empirical data on the generation, collection, transport, and storage of healthcare waste among healthcare professionals. Also, some literature14,37,38 has shown that auxiliary healthcare employees, such as sanitary workers, labor under inadequate conditions in situations where the management of healthcare waste has not received the attention and importance it requires. This includes Tanzania. Yet, according to earlier scholarly studies, sanitary employees lack the skills, disposition, and experience required for managing medical waste at their workstations.28,36,39
In Tanzania, for instance, sanitary personnel’ knowledge, attitudes, and practices about handling healthcare waste are not explicitly and empirically documented despite the aforementioned efforts by governmental and non-governmental groups to do so.40,41 If the issue is not addressed fully and cooperatively, the nation’s sanitation workers risk continuing to operate in contaminated settings under pressure from a variety of sources, notably in healthcare facilities, which could harm both their own and other people’s health. 42 However, if the current trend continues, sanitary workers may continue to manage healthcare waste in the best way they are currently capable of, which could highlight their lack of adequate knowledge while also causing the greatest amount of harm to the environment, other people, healthcare professionals, patients/clients, and the entire community. 10
To fill this gap, the study at hand used a descriptive cross-sectional study design to describe healthcare waste and evaluate sanitary workers’ knowledge, attitude, and practice in handling healthcare waste in the Dodoma region, the country’s central, fastest-growing city, and center of politics and academia. Such a study would reveal the undiscovered trend regarding sanitary workers’ knowledge, attitude, and practice in handling healthcare waste. It would also provide a potential means for authors to contribute their intellectual work to the body of knowledge and advance the movement toward empowering sanitary workers with healthcare waste handling knowledge, attitude, and practice as well.
Methods and materials
The University of Dodoma’s institutional guidelines and research ethics and standards for undergraduate and graduate programs, which provide a framework for conducting research by adhering to ethical issues to meet national and international research standards, were used to guide the conduct of this study. 43
Study setting
The study was carried out in six of the seven districts that were available in the Dodoma region, as illustrated in Figure 1. The dispensary, which provides community health services, maternity and child health services, and outpatient primary healthcare as the first level within its catchment area, is the lowest category of healthcare institution according to Tanzania’s health system. The health center is the initial referral center for dispensaries in its catchment area and provides both outpatients and in-patients (at least 24 beds), including maternity and child health services, obstetric theatre, diagnostic services, morgue, and surf-burner.

A map of the Dodoma region showing the districts where the study was conducted.
The district hospital acts as the main point of contact for pharmacies and health clinics. It has seven wards, providing both outpatients and in-patients (at least 100–175 beds), obstetric theatre, diagnostic services, mortuary, surf-burner, and is the first referral center for dispensaries in its catchment region. It also has outreach services for maternity and child health and mental health. The final point of referral at the local level is a regional referral hospital. It has nine or more wards, 176–450 beds, the main pharmacy, casualty, physiotherapy, laboratory, kitchen, laundry, morgue, store, operating room, administration, in-patient, and outpatients, among other departments. In addition, it provides clinics and specialized health services. 45
The Dodoma Municipal Council was able to access a regional referral hospital (colored yellow), three district hospitals (colored green), from the Chamwino, Chemba, and Kongwa districts, respectively, two health centers (colored red), and one dispensary (colored red) from the Mpwapwa district (colored light blue).
Study design and approach
To identify healthcare waste and investigate sanitary employees’ knowledge, attitude, and behavior on treating healthcare waste in the Dodoma area, the central portion of Tanzania, from March to August 2022, a descriptive cross-sectional study based in a health facility was used. Due to immigration, the region is continuing to be densely inhabited and a political, academic, and business hub, which results in a high demand for health services from various levels of health facilities.
Study population
Considering the advice of earlier researchers, 46 the following steps were taken to use Cochran’s formula from 1977 to establish the study’s minimal sample size. 47

where n = a minimum sample size of the study
p = the population proportion from previous studies (89.6%) 38
z2 = z-value (1.96) at reliability level (95%) or significance level (5%)
e2 = acceptable sampling error (e = 0.05)

The study needed at least n = 165 participants due to the non-response rate of 10% (n = 15). However, as depicted in Figure 2, only 156 of them were subjected to analysis since 9 individuals withdrew for a variety of reasons, including health issues (n = 4), a lack of willingness to engage in the study (n = 2), and failing to meet the inclusion requirements (n = 3).

Flow pattern of sample size determination and recruitment.
Inclusion and exclusion criteria
Consented sanitation workers at healthcare institutions, no more than 6 months of work experience, and fluency in English or Swahili were the requirements for inclusion.
Exclusion standards: the inability to hear, speak, or understand due to illness; part-timers.
Sampling procedures
A random sample of 156 out of 220 sanitation employees was taken from six of the seven health facilities in the Dodoma region. The sample was then distributed according to the number of facilities that were available and their level/type, which were stratified into dispensaries (n = 1: in one district), health centers (n = 2: in one district), district hospitals (n = 3: in one district), and regional referral hospitals (n = 1). The study comprised public health institutions, and consenting sanitation employees who were mentally sound, lived in the Dodoma region, could converse in Swahili, were not stupid or deaf, and could read and write took part. Written informed consent was obtained from all subjects and from the legally authorized representatives of the subjects who were not able to read and write (Table 1).
Proportional distributions of sanitary workers per the type of health facilities.

Source: Study plan (2022).
Data collection procedures
To evaluate the knowledge, attitude, and perceived practices of sanitary workers, the principal investigator worked with trained research assistants to collect data using interviewer-administered structured questionnaires. A structured healthcare waste checklist was also used to identify the generated healthcare waste.
Assessment of sanitary workers’ knowledge, attitude, and perceived practices of healthcare waste handling
To provide privacy, separate, empty rooms that were accessible on the grounds of the individual healthcare center were used. To reduce sharing, copying, and pasting of comments from one another, participants were sat in separate chairs. Before completing the questionnaires, the respondents received brief instructions, and the research staff was on hand to oversee, answer questions, collect completed questionnaires, and safeguard them appropriately. To ensure confidentiality, participant names were replaced by codes in the questionnaires. The completion of the surveys took, on average, between 30 and 45 min. The lead investigator and helpers examined the generated and stored medical waste to describe them in detail based on the items in the sampled sanitary workers’ reports the checklist for observation.
Identification of healthcare waste
Instead of actually counting the waste, sanitary personnel utilized their firsthand knowledge of the often collected, transported, and stored waste as a starting point to identify it. The structured checklist that was provided by the interviewer was used to investigate the forms of medical waste that sanitary employees believed they had once collected, transported, or stored at their workstations based on their personal experiences. The research team gave the sanitary workers a list of potential medical waste, and each worker was asked to choose or check the waste they believed was being collected, transported, or kept at his or her working station. For all types of sampled healthcare facilities, the list of likely medical waste was the same. The list was applied to all varieties of healthcare institutions, but regional referral hospital was utilized as a benchmark to assess the kind of healthcare waste produced in healthcare facilities. The lead researcher carried out the procedure with assistance from the qualified research assistants. The approximate time needed to finish filling out the checklist was 15–30 min.
Data collection tool and variable measurements
The study use data gathering tool from previous researches5,9,38 and pre-tested by the lead researcher, and examined by statisticians and professional peers. It included respondents’ sociodemographic characteristics profiles (n = 8 questions), knowledge of healthcare waste (n = 10 items), attitudes toward healthcare waste (n = 9 items), and perceptions of practices for treating healthcare waste (n = 9 things) (eight items). The factors in this study were measured using information from earlier investigations. Knowledge items had “Yes,” “No,” and “Don’t know” responses. A weight of “1” point was given to the “Yes” response, indicating that the participant answered the question correctly (correct response), and “0” points to the “No” or “Don’t know” responses, indicating that the participant did not know the answer at all or got it wrong (incorrect response). The greatest knowledge scores were determined as good knowledge (having good knowledge about treating medical waste); otherwise, not (having poor knowledge about healthcare waste handling). The five-point Likert scale used for the attitude components ranged from “1” for strongly disagree to “5” for strongly agree.
The Likert scale has been defined by scholars48,49 as a psychometric response, which is typically employed in questionnaires to ascertain participants’ preferences or levels of agreement with a statement or group of statements, in this case, the level of agreement of sanitation personnel on procedures for handling medical waste. Responses to the items were analytically converted into quartile measurements with “Agree,” “Neutral,” and “Disagree” categories for the descriptive purpose. The highest scores were classified as “positive attitude” (agreed that handling medical waste was a responsibility at their workstations), the median score was “neutral” (did confirm whether they agreed or disagreed with the statements about handling medical waste), and the lowest scores were classified as “negative attitude on handling medical waste” (not in agreement that healthcare waste handling was part of their responsibilities in their working stations).
A point of “1” was assigned for each action a sanitary worker would take, whereas a point of “0” was assigned for each ineffective or nonexistent activity. These actions included collection, transport, and storage of healthcare waste. Three elements made up the checklist for sanitary personnel to identify their perceptions of healthcare waste, with “Yes” denoting the existence of a certain waste (one point) and “No” denoting its absence (zero points). The purpose of the checklist was to determine whether sanitation personnel had ever seen or seen the pre-identified and shortlisted healthcare waste during collection, transport, or storage by the lead investigator.
Validity and reliability
Validity: In this study, content validity was chosen, and it was ensured by creating pertinent and useful research instruments, which were then shared with statisticians and expert colleagues for comments on the content suitability, sentence structure, language, and organization. The responses required research tools to be translated into Swahili to match the literacy level of the study respondents and improve the clarity, understanding, accuracy, and completeness of the information. Other factors, such as content appropriateness, sentence structure, and item organization, remained unaltered. They received the tools again for their final proof, for which no more inputs needed to be changed.
Reliability: To avoid information tampering, the principal investigator pre-tested the research instruments on a sample of 10% (n = 16) respondents in a place independent of the sampled study settings. Indicators including the items’ applicability, the language’s appropriateness, the clarity, and how long it would take to complete the surveys. The relevance of the issues was rated among 10 contacted independent reviewers using the inter-observer rating method. A pre-test observation showed that all topics were pertinent, scoring between 8 and 10, the wording was acceptable and understandable, and the surveys would be filled out and finished in between 30 and 60 min. The results of the pre-test were then subjected to a scale analysis to ascertain the reliability of the instruments, which revealed that items that measured knowledge demonstrated a Cronbach = 0.81, 0.79 for attitude scale, and 0.73 for practices and therefore, as advised by previous academics.50–52 The equipment was thought to be trustworthy for the real field data collecting.
Statistical analysis
Data were cleaned and descriptively analyzed using the Statistical Package for Social Sciences computer software program version 25 that is available in the institution. The survey respondents’ sociodemographic profiles and the determination of healthcare waste were examined, quantified, and given in frequencies and percentages. The association between the variables was established using the chi-square test and cross-tabulation analysis, with a 95% confidence level and a 5% level of significance.
Results
The research’s findings are presented in this section. The results are presented in accordance with the objectives, starting with the sociodemographic characteristics of sanitation workers, percentages of healthcare waste, identification of healthcare waste, and proportional distribution of knowledge, attitude, and perceived practice of handling healthcare waste.
Social demographic characteristics profiles of the study respondents
The study showed a 100% response rate. In Table 2, district names are denoted by the letters “A,” “B,” “C,” “D,” “E,” and “F.” To ensure confidentiality, the genuine names of districts are bracketed using letters. The results show that the average age of the study participants was 28.6 years, ranging from 18 to 52 years, and that 74.4% of them (n = 116) were female. Between the ages of 25 and 34, there was the greatest amount of dominance (50.0%). Of 156 study participants, 72.4% (n = 73) lived in district “F” and 76.3% (n = 119) worked in regional referral hospitals with less than a year of experience (63.5%). Also, in Table 2, findings show that 54.5% (n = 85) of sanitary employees had only completed their primary school, followed by 36.4% (n = 57) of them who had completed their secondary education, and 9.0% of them had never received any kind of formal education. For more information, see Table 2.
Social demographic characteristics profiles of the study respondents (n = 156).

Source: Field data (2022).
Proportional distributions of healthcare waste generated in health facilities based on sanitary workers’ responses
According to replies from sanitation workers about the types of medical waste that were produced most frequently at their workstations (Figure 3), 78.4% (n = 122) of the trash generated was non-infected, whereas 21.6% (n = 34) was infectious. For a more visual representation of the proportional distributions of the various categories of medical waste produced in the sampled medical facilities, see Figure 3.

Proportional distributions of healthcare waste generated in health facilities based on sanitary workers’ responses.
Proportional contributions of the generated infectious and non-infectious healthcare waste per the types of health facility
To determine the proportional contributions of the generated infectious and non-infectious healthcare waste per the levels of health facility, descriptive analysis was performed on the reported responses from sanitary workers about the healthcare waste generated in the sampled health facilities. Findings in Figure 4 show that of the 21.6% of infectious medical waste created in all studied health institutions, regional referral hospitals contributed 13.2%, followed by district hospitals (4.7%), health centers (2.9%), and dispensaries (0.8%). Also, of the 78.4% non-infectious medical waste, 43.5% was produced in district hospitals, followed by 20.3% in regional referral hospitals, 11.1% in health clinics, and 3.7% in dispensaries. See the image for a figurative representation of the contribution made by the sampled healthcare facilities in terms of the generation of waste.

Proportional distribution of perceived healthcare waste collected, transported, and stored based on the type of health facilities sampled in this study.
Healthcare waste collected, transported, and stored in the sampled health facilities
The findings in Figure 5 highlight the healthcare waste that sanitary staff in healthcare institutions collect, transport, and store. The results are not based on an actual count of medical waste; rather, they are based on sanitary workers’ reported first-hand experiences, which were then compared to the percentage of responses they gave regarding the types of medical waste they believed were most frequently collected, transported, and stored at their workstations. According to research on non-infectious healthcare waste, paper waste was collected, transported, and kept in greater quantities than plastic bags or plastic/metal bottles (17.0%) and paper garbage (21.2%). Additional non-infectious medical waste comprised food trash (13.1%), timber materials (8.2%), broken medical equipment (8.2%), drug/medicine waste (5.0%), tubing/catheter (6.1%), and chemical waste (2.3%).
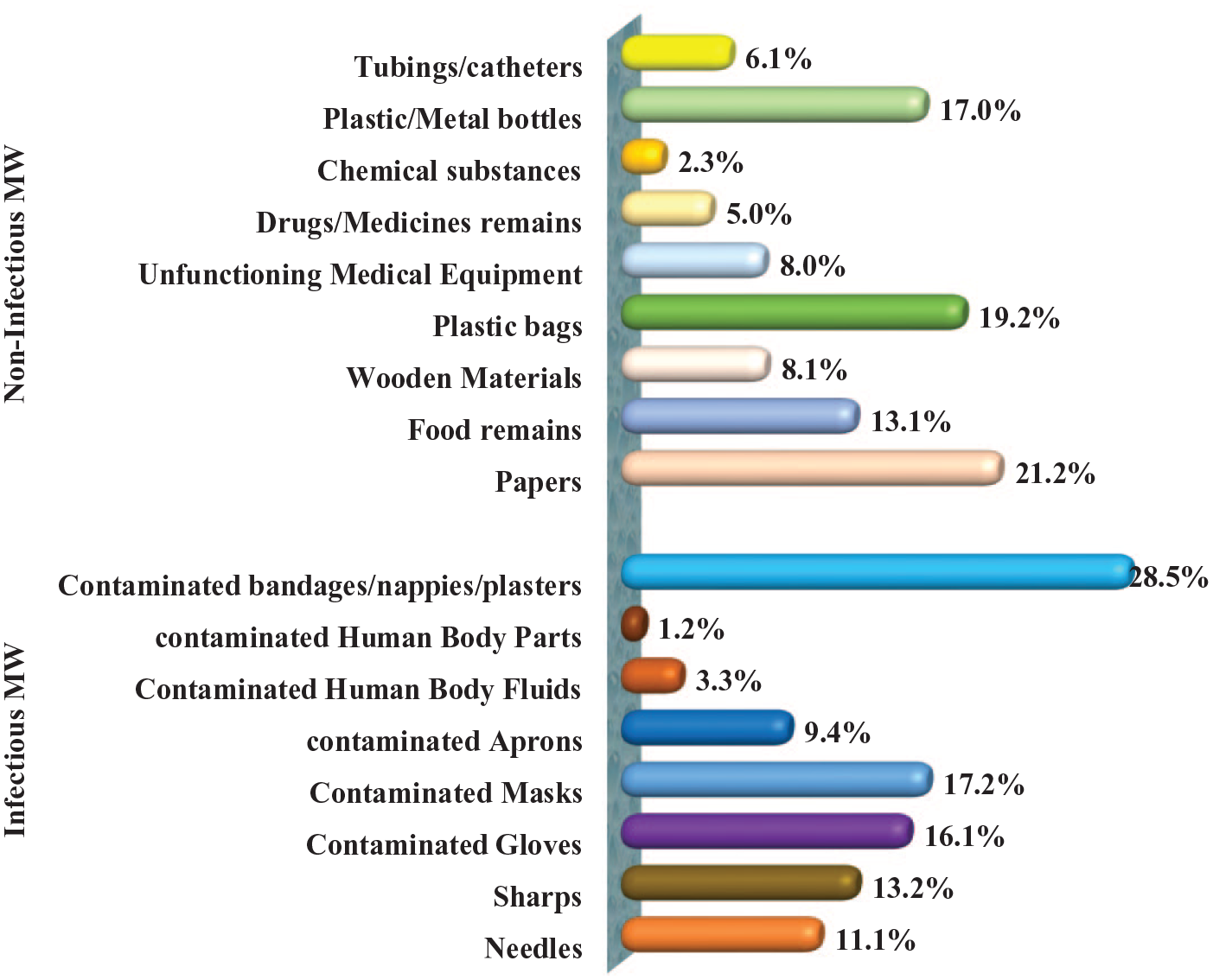
Healthcare waste generated in the sampled health facilities.
On the other hand, contaminated bandages/nappies/plasters (28.5%), infected masks (17.2%), and contaminated gloves (16.1%) were among the infectious healthcare waste that sanitary staff collected, transported, and stored at all healthcare institutions. Sharps (13.2%), needles (11.1%), contaminated aprons (9.4%), polluted human body fluids (3.3%), and contaminated human body parts (1.2%) were among the other infectious healthcare waste. Refer to the figure for a more illustrative depiction of the percentage distribution of the healthcare waste that sanitary staff in the sampled healthcare facilities collected, moved, and stored.
Knowledge of sanitary workers on healthcare waste handling
In Figure 6, it was discovered that the majority of sanitary personnel (74.4%) lacked adequate knowledge of how to handle medical waste. The remainder of them (25.6%) had solid expertise of handling medical waste. For a representation of the proportional distribution of knowledge regarding the handling of medical waste, see Figure 6.

Knowledge of sanitary workers on healthcare waste handling.
Attitude toward healthcare waste handling among sanitary workers
The attitude results of Figure 7 show that 67.8% (n = 106) of sanitary personnel had a negative attitude, 19.9% (n = 31) had a positive attitude, and 12.3% (n = 19) had a neutral attitude toward the handling of medical waste in hospitals in the Dodoma region of Tanzania. For more information on the distribution of sanitary personnel’ views regarding handling medical waste, please see Figure 7.
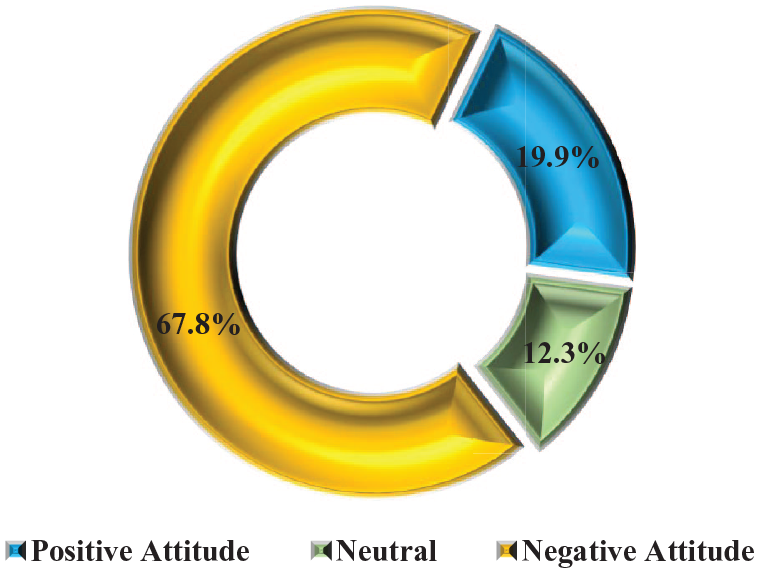
Attitude of sanitary workers on healthcare waste handling in Dodoma region, Tanzania.
Perceived practice on healthcare waste handling among sanitary workers
According to descriptive data in Figure 8, a higher percentage of sanitary employees (63.6%) than their counterparts with good procedures were found to have unsatisfactory perceptions of how to handle healthcare waste. On the other side, 36.4% of sanitary workers viewed the way medical waste was handled at their workstations as being satisfactory. For a representation of the perceived distributions of medical handling procedures among sanitation personnel, see Figure 8.

Perceived practice on healthcare waste handling among sanitary workers in Dodoma region, Tanzania.
Proportional distributions of the most commonly used personal protective gear among sanitary workers working in health facilities
Figure 9 displays the proportional distribution of the most popular personal protection equipment used in health institutions in the Dodoma region of Tanzania, as reported by sanitation workers. The percentage of companies (employers) offering official uniforms was 41.3%, followed by rubberized boots (20.1%) and rubberized gloves (12.3%). Masks (9.4%), rubberized aprons (6.4%), sanitary coats (4.9%), sanitary caps (3.6%), and eye protection (2.0%) made up the rest of the wearable safety equipment. None of the sanitation workers wore reflector-equipped overalls (0.0%) or jackets (0.0%). Refer to the illustration for a representation of the proportional distribution of the personal protective equipment worn by sanitary personnel during the handling of medical waste at their workstations.
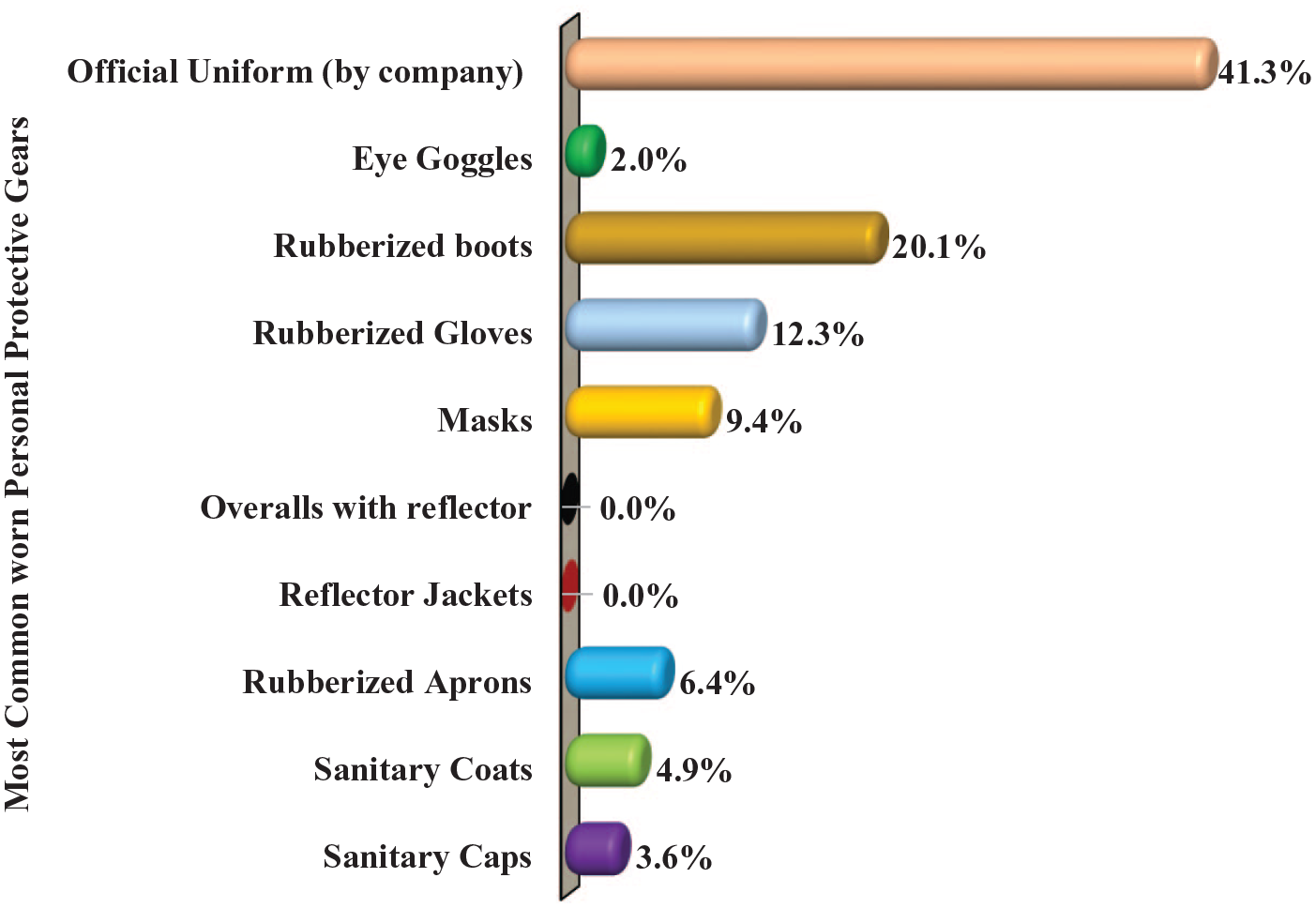
Proportional distributions of the most commonly used personal protective gear among sanitary workers working in health facilities.
Proportional distributions of the most commonly used equipment by sanitary workers for transporting healthcare waste from the health facility’s units to the dumping sites/incinerators
To show how responsible each organization/institution was in obtaining, securing, and providing them in the sanitary employees’ working stations, this study evaluates the availability and use of various equipment for the collection, transportation, and storage of healthcare waste. The findings in Figure 10 show that for collecting, moving, and storing medical waste, sanitary personnel at health facilities in the Dodoma region most frequently utilized plastic bags (31.3%), buckets with lids (27.9%), and boxes (12.6%). Wheelie bins (9.1%), wheelbarrows (8.8%), dustbin trolleys (7.3%), and plastic dustbins (3.0%) made up the other equipment. Refer to the illustration for a representation of the proportional distribution of the tools used by sanitary staff to manage medical waste at their workstations.

Proportional distributions of the most commonly used equipment by sanitary workers for transporting healthcare waste from the health facility’s units to the incinerators within Dodoma region, Tanzania.
Factors related to sanitary workers’ knowledge, attitude, and perceived practices of healthcare waste
According to Table 3, the type of healthcare facilities sanitary workers were employed in, their ages, sexes, levels of education, and time spent working were all significantly related to their perceptions of the knowledge, attitudes, and practices surrounding the handling of medical waste at their workstations (significance 0.05). Nonetheless, sanitary employees’ reported practices regarding the handling of medical waste were strongly correlated with their knowledge and attitude levels (p = 0.05). Contrarily, there was no statistically significant correlation between the sanitary employees’ knowledge, attitude, and perceived practice regarding the handling of medical waste (p > 0.05) and the location of the health facilities, their marital status, or their religion.
Factors related to knowledge, attitude, and perceived practices of sanitary workers on healthcare waste handling (n = 156).

Source: Field data (2022).
Discussion
The study showed a 100% response rate, with the majority of respondents working in district and regional referral hospitals rather than lower tiers of healthcare facilities in the area. The results of this study revealed impressive efforts by healthcare facilities and private organizations in hiring sanitary organizations for proper and timely healthcare waste management. These efforts support the situation of water, sanitation, hygiene, and food services as stressed in the Tanzanian national health policy. At all levels of the tested health facilities, women were also employed and engaged in sanitary labor activities. This study has the necessary value since it responds to the warning stated in the nation’s national health policy on the occurrence and spread of infections and infectious diseases. The study is also very significant because it addressed a crucial issue in healthcare waste handling, which is supported by Sustainable Development Goal 3’s target 3.9, which emphasizes reducing the number of infectious disease deaths and illnesses caused by infectious chemical pollution and contamination of the air, water, and soil by 2030. 53
According to the findings of this study, sanitary employees lacked proper expertise and had unfavorable attitudes about handling medical waste. The results of this study may serve as the foundation for promotional interventions that may concentrate on equipping sanitary workers with healthcare waste handling knowledge, attitude, and practice for their safety as well as the health safety of close family members based on the national health policy and health strategic plans that advocate infection prevention and control. According to research, many sanitary workers were unaware of the rules that must be followed when handling healthcare waste, despite some of them demonstrating good knowledge of the concept, types, and advantages of handling healthcare waste, such as the prevention of disease transmission and environmental pollution in their places of employment.
Such findings could be attributed to the variety of healthcare facilities, where working in higher-level healthcare facilities would provide sanitary workers with some opportunities to be exposed to training, long-term mentoring, and close supportive supervision of healthcare waste handling than working in low-level healthcare facilities like dispensaries and health centers. Nonetheless, there were differences in the educational backgrounds of sanitary personnel, and the majority of those with more education were located in district and regional hospitals rather than health clinics and dispensaries. This study came to the conclusion that education is highly recommended because it may be associated with one’s capacity to comprehend and exhibit a favorable interest in a particular phenomenon or activity.
Sanitary staff members employed by regional referral and district hospitals would be more knowledgeable about handling medical waste than their counterparts employed by health centers and dispensaries, respectively. The results, on the other hand, showed that knowledge and attitude toward handling medical waste were substantially related to the working experiences of sanitary personnel. Long-term exposure to a certain task can help people grasp it and create attentiveness habits toward it. This could mean that as one gains experience in a certain area, knowledge, positive concern, and ultimately mastery of that area—in this example, hospital waste handling—increase.
Notwithstanding the differences in the study group, the findings of this study begin to resemble those of Nosheen et al., 28 and Thirunavukkarasu et al., 37 who investigated related factors discovered that 64.6% and 62.9% of the participants in the study were unaware of the idea of handling healthcare waste or its significance at their working stations, respectively. According to Khalid et al., 39 that inadequate procedures for treating medical waste have been used in healthcare facilities, which is likely due to the lack of training and unfavorable attitudes of the staff. Furthermore, according to Olaifa et al.,’s 13 research conducted in South Africa, healthcare workers still struggle with a lack of understanding of how to manage waste in the industry. But in their research, Basavaraj et al., 54 in India, it was found that, in contrast to healthcare professionals who showed high knowledge of handling healthcare waste, other auxiliary workers fell short by lacking an understanding of the significance of and procedures for managing healthcare waste at healthcare facilities.
Yet, according to research by Deress et al., 55 similar circumstances to those in this study were revealed in Ethiopia, where many healthcare personnel used their knowledge of dealing medical waste in the course of their employment. The results of this study on knowledge, however, diverge from those noted by Abalkhail et al., 29 and Uloma et al., 31 discovered that many healthcare professionals in hospitals showed high understanding of healthcare waste. Likewise, Letho et al.,’s 32 research showed that the majority of healthcare professionals were aware of the dangers associated with managing medical waste. It is claimed that the variances from the study at hand are caused by variations in the study population, timing of the study, sample size, and/or geographic locations.
In this study, the attitudes of sanitary workers toward handling medical waste were also evaluated, and the results showed that most of them did not view handling medical waste at their workstations as a full-fledged responsibility. The majority of them held the opinion that handling medical trash was unnecessary because it was none of their business and was already waste that only needed to be dumped out of sight of people. Others showed a conviction that the administrative departments of the relevant healthcare facilities were the most appropriate and accountable organs to manage healthcare waste and not anybody else. When it came to their duties handling medical waste, sanitary staff who worked in regional referral and district hospitals displayed a more positive attitude than those who worked in different medical clinics and drug stores.
The results may suggest that their disparate attitudes can be attributable to disparities in how healthcare waste is generally understood and in the job descriptions they were given as part of their employment agreements depending on the levels of health facilities they were working in. Also, sanitary personnel may have received different treatment depending on the degree of the health facilities they were employed in, according to the findings on attitude. To feel less concerned about healthcare waste collection, transportation, and storage, the majority of sanitary personnel in health facilities and dispensaries would represent themselves as having a small contribution to the handling duties. A person’s perception of their own importance in relation to a certain phenomenon would be correlated with how much their own and other people’s safety and health were at risk from the contagious medical waste. Yet, this study’s results suggest that sanitary workers’ negative attitudes regarding healthcare waste management may have been influenced by unfavorable or hostile working conditions as well as inadequately recognized advantages of working in health facilities as a sanitary worker.
Demotivation is the primary cause of sanitary employees’ unfavorable attitudes regarding handling medical waste, according to research. Starovoytova and Namago, 56 who also obtained findings similar to those of this study, found the majority of healthcare personnel showed hostility against the disposal of medical waste in their workplaces. The majority of sanitary personnel displayed bad perceived behaviors when it came to treating medical waste, according to their perceptions. The majority of them (73%) claimed to have never used any method of handling medical waste and occasionally did not wear personal protective equipment while at their workstations. Despite being the most crucial personal protection equipment given the nature of sanitary work, very few sanitary personnel handled medical waste at their workstations while wearing rubberized gloves and boots, for example. This study has identified a trend whereby sanitary workers’ work was occasionally extremely dangerous when handling healthcare waste. This was likely caused by inadequate knowledge and misconceptions that healthcare waste was not harmful to their health, the health of others, or environmental pollution.
Sanitary employees were in charge of gathering, transporting, and storing medical waste before it was discarded or burned at the appropriate locations and/or incinerators, according to the appropriate parties. Results showed that the most frequently used personal protection equipment while at work stations was official clothes provided by the company, boots, and gloves. The most common items used for gathering, moving, and storing medical waste before it is sent to the appropriate incinerators or waste-burning locations on the grounds of the healthcare facility were discovered to be plastic bags, buckets with lids, and boxes. The levels of health facilities sanitary personnel were working in may be related to the development of subpar healthcare waste handling methods, perhaps because the greater level of the health facility would be linked with the appropriate amount of procedures for handling medical waste.
According to the Tanzanian health system, higher-level medical facilities may occasionally be classified as strategic medical facilities to provide people with high-quality, cost-effective care, and as a result, they may be subject to frequent unannounced visits by higher authorities. The situation would undoubtedly prompt sanitary staff to assume full responsibility and put in extra effort while treating medical waste at their workstations. In addition, it may not be taken as a guarantee, but it appears that the way sanitary workers handled medical waste was related to both their education and attitude, with the idea being that the more educated someone was, the more likely it was that they would act ethically and have a positive attitude toward their duties. Also, it was discovered that work experience was strongly associated with hygienic employee perceptions of healthcare waste handling procedures.
According to the findings of this study, continuous exposure to a task and engagement with it provide a person a better chance of mastering its procedural details than when someone else would not. According to the outcomes of this investigation, Alqathani et al. 30 noted that despite the fact that many healthcare professionals were educated about bio-healthcare waste, there was still room for improvement in the way they handled it on a daily basis in their workplaces. Nonetheless, research by Dalui et al. 57 are opposed to this study since it showed that controlling healthcare waste in healthcare facilities was a task that most healthcare workers performed better when they had more understanding of. Moreover, Jalal et al., 58 in Saudi Arabia discovered that many healthcare personnel adhered to and performed bio-healthcare waste disposal more appropriately, according to their findings. The variations in results between researches may have been influenced by study demographic, methodological techniques, scheduling, and/or sample size.
Notwithstanding the study’s positives, numerous research-based weaknesses were found that might need to be taken into account when interpreting the results. One of the drawbacks was the lack of appreciable variations in the data collection methods based on the levels of healthcare facilities where sanitary staff were working to identify appreciable variations in their knowledge, attitude, and practices regarding healthcare waste treatment. If you do not, it could be very challenging to compare them. Further operational studies may be required on the practices and attitudes of sanitary workers toward handling medical waste, especially with regard to the risks they face, the steps involved in handling waste that fell within their scope of expertise, and the protective gear required for each task they performed. The current study, however, was restricted to examining the management of medical waste with biosecurity or not moving too much weight without regard to the type of equipment or vehicle, which is an important issue that needs to be thoroughly examined by further studies.
The study was carried out in a fairly small area, so its conclusions might not apply to sanitary workers in other parts of Tanzania or abroad who do not live in the Dodoma region, the country’s central region. The results of this study need to be carefully evaluated because they came from a relatively small sample and did not establish a causal link between the variables being investigated. Also, the discussion section’s citations and references give studies on healthcare personnel rather than auxiliary staff members like sanitary employees; thus, a comparison of the findings may need to be done carefully and attentively. In addition, the study did not employ a triangulation method to data collecting, and as a result, it is possible that dependability, transferability, and/or confirmability rigor were not taken into consideration in this investigation. The results of this study should still be evaluated carefully, though, as the caregivers may have had trouble recalling and discussing their prior feeding practices. The ability to rate oneself is challenged since it can lead someone to under- or overrate themselves or the habits/information they reported as caregivers who took part in the study. Consequently, care must be taken while interpreting this study’s conclusions.
Conclusion
Tanzanian healthcare personnel are performing better when it comes to waste segregation practices, which is their main responsibility in handling healthcare waste and preventing and controlling infection. Other auxiliary health employees, such as sanitary workers, are responsible for the delivery, storage, treatment, and disposal of medical waste at landfills or incinerators. It was unclear across the nation whether or not sanitary employees have the same training, attitude, and practice about handling medical waste. The circumstance raises unresolved questions about whether sanitation staff are knowledgeable about proper healthcare waste treatment in healthcare institutions and whether they have a positive attitude about it.
This study discovered that sanitary workers regularly come into touch with infectious healthcare waste at their workstations, despite the fact that non-infectious healthcare waste is produced in huge quantities. The majority of sanitary employees did not understand how to handle healthcare waste, despite being the closest person to the collection, transport, and storage of healthcare waste. Also, sanitation employees believed that processing medical waste was outside of their purview and as a result, judged themselves to be incompetent to follow the necessary procedural norms.
The study’s conclusion is based on the notion that different educational backgrounds, hospital types, and occupational experiences serve as different motivators for good medical waste management procedures. Due to their unfavorable attitudes, the sanitation workers’ shown a tendency to disregard the value of personal protection equipment for their own safety, the safety of others, the environment, plants, animals, other healthcare professionals, patients/clients, and the general public. This study discovered that sanitary employees use plastic bags, buckets with lids, and boxes as quick and convenient equipment to them for gathering and carrying the created medical waste to burning sites or incinerators, which is related to the aforementioned issue.
The analysis of other studies has revealed both similar and divergent conclusions from this study, the majority of which focus on healthcare professionals rather than auxiliary staff like sanitary workers. This may mean that, rather than empowering other healthcare teams or employees, including sanitary staff, the majority of interventions from those studies have concentrated on enabling healthcare workers and professionals for the proper treatment of healthcare waste in healthcare facilities. Lack of consideration and involvement of auxiliary health staff in educational programs could undermine safety and increase health risks for them and others. Hence, participatory waste handling teaching programs designed using sociodemographic characteristics profiles of sanitation employees may enable them to protect themselves from endangering safety and health risks from incorrect healthcare waste treatment.
Recommendation
As suggested by previous scholars,17,28 the results of this study show that there is a need for contemporary, innovative techniques that support equipping sanitary employees with skills in handling healthcare waste, particularly those that emphasize ways to make the wastes renewable. Policymakers, administrative agencies, managers, bosses, and training institutions can use the findings from this study to develop innovative strategies that involve and empower sanitary workers and other related auxiliary health staff with knowledge, attitude, and skills for appropriate practices of handling healthcare waste in their working stations, even though such innovative ways may take some time to be installed and implemented in health facilities within Tanzania.
The results of this study may also show that Tanzania’s healthcare systems need to work together across disciplines to manage healthcare waste according to the available policies, guidelines, and standards. Typhoid fever, diarrheal disorders, malaria, skin diseases, respiratory tract infections, and cholera, to name a few, are just a few examples of health-related concerns that may require sanitary employees to be trained in handling medical waste. The results of this study will offer a useful base of data and information regarding knowledge, attitude, and the perceived behaviors of sanitary employees on healthcare waste treatment for large-scale interventions or future research, if they are published in various scientific journals.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231174735 – Supplemental material for Knowledge, attitude, and perceived practice of sanitary workers on healthcare waste management: A descriptive cross-sectional study in Dodoma region,Tanzania
Supplemental material, sj-docx-1-smo-10.1177_20503121231174735 for Knowledge, attitude, and perceived practice of sanitary workers on healthcare waste management: A descriptive cross-sectional study in Dodoma region,Tanzania by Walter C Millanzi, Patricia Z Herman and Samweli A Mtangi in SAGE Open Medicine
Footnotes
Acknowledgements
It is an honor to praise God for giving us the power and life to do this task. Thank you for your readiness and support in providing ethical clearances, University of Dodoma and administrative bodies of health facilities in the Dodoma region. We thank the sanitary workers who agreed to participate in the study and offered their full cooperation by freely sharing their opinions on healthcare waste handling throughout the entire process. The aforementioned organs and/or individuals made significant contributions to the work’s results.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This was not an interventional or trial study that involved experiments on live vertebrates and/or higher vertebrates. The study adhered to the University of Dodoma institution’s guidelines and the Institutional Research Review Committee (IRRC) approved it with an approval letter referenced DJ.232/238/0-28.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects and from the legally authorized representatives of the subjects who were not able to read and write.
Submission declaration and verification
This work has not been published or submitted under consideration elsewhere and if accepted and published in this journal it will not be re-submitted for publication elsewhere in the same form.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.