
Abstract
Objective:
Angiographic embolization is an established method of treating intractable cases of posterior epistaxis. This study aimed to test the effectiveness and safety of this method in treating cases refractory to conservative methods.
Methods:
A descriptive retrospective analysis of consecutive cases referred to the department of interventional radiology with refractory epistaxis from January 2001 to December 2018 and received a selective angiographic embolization of the sphenopalatine artery was done. Only epistaxis of idiopathic origin was included in the study.
Results:
During this period, 98 embolizations were performed. The success rate reached 81.6%. Minor complications were registered in 5%, with no single major complication. The length of stay was 10.5 ± 5.6.
Conclusion:
Selective angiographic embolization is an effective, safe, and minimally invasive method in treating refractory epistaxis.
Keywords
Introduction
Epistaxis is the most frequent symptom that general practitioners meet. It has a prevalence of up to 60% of the population. However, only 6% seek a medical consultation. 1 Epistaxis has a bimodal incidence between 11–20 and 50–70 years of life. 2
The severity of nasal bleeding can be so intense that the patient requires hospital treatment or, sometimes, a surgical intervention. 3 Consequences of epistaxis could range from circulation problems, toxic shock syndrome, acute bacterial rhinosinusitis, anemia, and in very rare cases, death.4 –6
Treatment of epistaxis depends on the cause, localization, and severity of nasal bleeding. Adjusting the patient’s medication (e.g., antihypertensive drugs, anticoagulants) can be, in many cases, enough to reduce the bleeding tendency. Anatomical deviation or vascular malformation may need operative intervention (e.g., septal or sinus surgery).
Anterior epistaxis accounts for 80% of bleeding cases. 7 Bleeding from the anterior nasal cavity is mostly easy to treat conservatively through local hemostatic measures (anterior packs and/or chemical cautery). On the other hand, the management of posterior and superior epistaxis continues to be a complex problem due to less accessibility and mainly needs a surgical or endovascular intervention (Figure 1).8,9
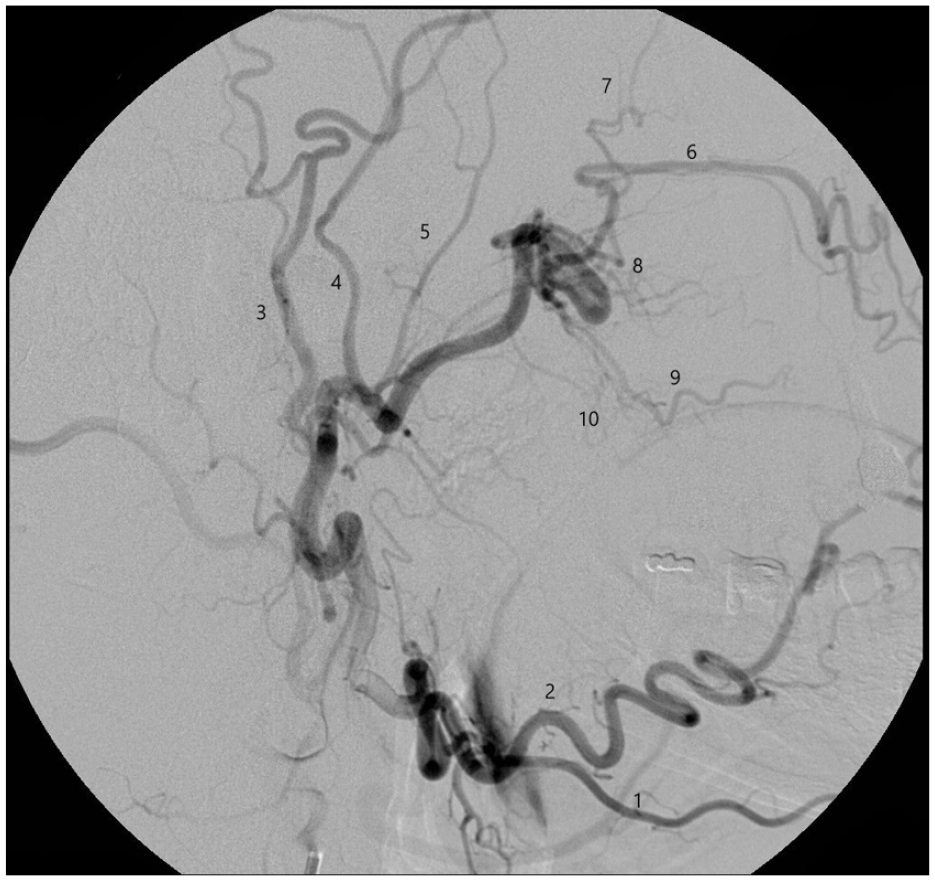
DSA showing anatomy of the maxillary artery: 1. Submental artery, 2. Facial artery, 3. Superficial temporal artery, 4. Middle meningeal artery, 5. Posterior deep temporal artery, 6. Infraorbital artery, 7. Anterior deep temporal artery, 8. Sphenopalatine artery, 9. Descending palatine artery, 10. buccal artery.
Ligating the maxillary artery through a transantral approach has been the most common surgical procedure to treat severe epistaxis (Figures 2 and 3). 10

(a) DSA showing angioma in the sphenopalatine artery in a patient suffering from Rendu-Osler-Weber-Syndrome. Anteroposterior view before embolization (arrow pointing at the angioma); (b) DSA showing angioma in the sphenopalatine artery in a patient suffering from Rendu-Osler-Weber-Syndrome. Lateral view before embolization (arrow pointing at the angioma); (c) DSA showing angioma in the sphenopalatine artery in a patient suffering from Rendu-Osler-Weber-Syndrome. Anteroposterior view after embolization; (d) DSA showing angioma in the sphenopalatine artery in a patient suffering from Rendu-Osler-Weber-Syndrome. Lateral view after embolization.

(a) DSA showing aneurysm of the sphenopalatine artery. Lateral view before embolization (arrow pointing at the aneurysm). 1. Infraorbital artery, 2. Sphenopalatine artery, 3. Descending palatine artery, 4. Posterior superior alveolar artery, 5. Buccal artery; (b) DSA showing aneurysm of the sphenopalatine artery. Anteroposterior view before embolization (arrow pointing at the aneurysm); (c) DSA showing aneurysm of the sphenopalatine artery. Anteroposterior view after embolization (arrow pointing at the sphenopalatine artery).
Embolization of the sphenopalatine artery is considered a minimally invasive method compared to surgical interventions. It is mainly performed with local anesthesia. Complications resulting after the endovascular intervention can be classified into minor and major complications. Minor complications are self-limited. Examples are local pain, numbness, swelling, hematoma, skin slough, trismus of the jaw, groin pain or bleeding, spasm of the maxillary artery, mental confusion, hypotension, transient ischemic attack, and aspiration pneumonia. Major complications include internal carotid artery injury, facial nerve paralysis, hemiplegia, skin necrosis, blindness, cerebrovascular accident, and myocardial infarction. 8
Limitations of an endovascular intervention are arteriosclerosis, anastomosis with the internal carotid artery, strongly curved arteries, allergy to contrast material, or when on the initial angiogram, involvement of the internal carotid artery (anterior and posterior ethmoidal arteries) in the epistaxis is seen.
Objectives
This study aimed to assess the effectiveness and safety of the endovascular intervention in treating episodes of epistaxis refractory to conservative treatment methods.
Materials and methods
Angiography of the common carotid artery was performed with a 5F catheter. First, the common carotid artery was probed through a transfemoral approach, and the internal and external carotid arteries were represented. Next, the internal carotid artery was explored to ensure it was not the cause of nasal bleeding and exclude the existence of anastomosis in the external carotid artery. Afterward, the external carotid artery was probed using a mechanically stable guide catheter. A microcatheter (0.018–0.028 ID) was then passed through the guide catheter to complete probing the external carotid artery to its terminal branch until the embolization was completed.
A careful analysis of the digital subtraction angiography is advisable to identify any possible connection between branches of the external carotid artery and the ophthalmic artery. In these cases, due to the risk of blindness, embolization is contraindicated. In addition, other possible anastomoses between external and internal carotid arteries also contraindicate embolization.
After evaluation of the external and internal carotid arteries, the microcatheter will be as far distally placed in the pterygopalatine segment of the maxillary artery, distal to the middle meningeal, and eventually accessory meningeal artery. Being unable to bring the microcatheter that far could result in postoperative trismus due to embolizing masticatory arteries in the pterygoid segment.
Embolization was done using polyvinyl alcohol (PVA). Only in cases of aneurysm or pseudoaneurysm micro coils or cyanoacrylate was used. 11
The mainstay of therapy by epistaxis is PVA or gelfoam.12,13 Both materials are well established and showed high safety and efficacy. 14
Embolization was performed in real-time fluoroscopy. Embolization material was mixed with a contrast medium to control the anterograde flow of the material. Embolization material will be pushed until no contrast medium is seen in the nose.
A retrospective analysis was done of all patients referred to the department of interventional radiology with refractory epistaxis from January 2001 to December 2018 and received a selective angiographic embolization of the sphenopalatine artery.
Medical history, medications, nursing records, documentation, laboratory findings, surgical reports, and medical discharge reports were collected for every patient and analyzed. Epistaxis following trauma or as a result of tumors was excluded from this study.
In this retrospective study, written informed consent was neither needed from subjects nor a legally authorized representative (in the case of minors). The ethics committee confirmed this. However, informed consent was provided by the department of interventional radiology to collect the data. Only informed consent was obtained from the interventional radiology department to use and analyze the data and angiographs.
After collecting all the necessary data, the patients were classified into one of four groups.
- Group 1: Patients underwent an endovascular intervention and showed no bleeding after removal of the nasal tamponade till their discharge.
- Group 2: Patients underwent an endovascular intervention and showed self-limited bleeding that required no surgical intervention.
- Group 3: Patients underwent an endovascular intervention and showed intense bleeding that required surgical intervention. This surgical intervention was performed within 2 weeks after embolization and was not in the territory of the sphenopalatine artery.
- Group 4: Patients underwent an endovascular intervention and showed intense bleeding that required surgical intervention in the territory of the sphenopalatine artery. This surgical intervention was performed within 2 weeks after embolization.
Patients were observed for 2 days after the intervention before they were discharged. Recall appointment 2 weeks after discharge was advised to reassess clinical findings.
Statistical analysis
A descriptive statistical analysis was done in terms of mean and standard deviation (SD) using Microsoft Excel, 2010.
Results
From January 2001 to December 2018, 107 patients were administered to our hospital suffering from severe epistaxis and referred to the department of interventional radiology for further embolization. A total of 100 endovascular interventions were performed to stop the nasal bleeding. For the remaining seven patients, the attempt at endovascular intervention had to be discontinued. Age ranged from 17 to 89 years. The mean age was 62 (59 among males and 63 among females).
The endovascular investigation for abovementioned seven patients was discontinued due to anatomical considerations. Initial angiography showed for the first patient a thromboembolic closure of the sphenopalatine artery (Figure 4). An arteriosclerotic plaque in the brachiocephalic trunk (subclavian steal phenomenon) was seen for the second patient (Figure 5). For both patients there was no arterial approach to the external carotid artery. Therefore, direct cannulation of the external carotid artery through a transbronchial approach was not done. Three patients showed severe looping, so placing a microcatheter in the sphenopalatine artery was impossible (Figures 6–8). The sixth patient showed severe arteriosclerosis of the common carotid artery. The seventh patient showed severe elongation of the arteries in the pelvic region, neck area, and the external carotid artery so that deep punctuation of the terminal branches of the external maxillary artery was not possible (Figure 9). Two out of these seven patients were not cooperative and unstable which made further catheter placement very difficult.

Thromboembolic closure of the sphenopalatine artery.

Arteriosclerotic plaque in the brachiocephalic trunk (subclavian steal phenomenon). Black arrow shows the arteriosclerotic plaque and lack of further penetration of contrast material.

Elongation of the arteries in the pelvic region, neck area and the external carotid artery so that a deep punctuation of the terminal branches of the external maxillary artery was not possible: (a) Unsubtracted angiography of pelvic region showing loop formation (black arrow), (b) unsubtracted angiography showing elongation of the supra-aortic arteries (black arrows), and (c) DSA showing loop formation in the external carotid artery (black arrows).

DSA showing 180° loop formation in the external carotid artery (black arrows).

DSA showing elongation of the brachiocephalic trunk (black arrow).

DSA showing elongation of the external maxillary artery, so that a deep insertion of the catheter in its terminal branch was not possible.
The transcatheter embolization was performed with local anesthesia. However, the intervention was performed with general anesthesia in six cases. This was decided due to the uncooperative behavior of patients, intellectual disability, or severe anxiety.
Two cases were excluded from the study. Epistaxis was a consequence of trauma in one case. A tumor was the cause of nasal bleeding in the other one. The remaining 98 patients were classified as idiopathic epistaxis and were included in the study.
Under the treated patients was a male dominance of 63%. The age of patients ranged from 17 to 89 years (mean 62 years).
Patients were observed for 48 h after embolization; the nasal tamponade was removed and then dismissed in case of stopped nasal bleeding. If there is still nasal bleeding, a new tamponade was inserted again within 24–48 h. After two failed attempts of tamponade insertion, patients were referred for further surgical intervention (ligation of the maxillary artery with or without anterior and posterior ethmoidal arteries).
The mean hospital stay among patients was 10.5 days with a maximum of 27 days and a minimum of 1 day (SD 5.6). The mean postembolization hospital stay was 3.3 days (SD 2.7). The prolonged stay was due to patient comorbidity and the need to adjust other medications. The patient who was discharged immediately after the intervention was as per his own wish and against medical advice.
The mean length of stay for patients who were merely treated with embolization and did not need further treatment (group 1) was 9.1 (SD 4.6). This group’s mean postembolization hospital stay was 4 days (SD 1.9).
Local and systemic risk factors found among patients are listed in Table 1.
Local risk factors.

We aimed to embolize only the sphenopalatine artery. However, avoiding the embolization of the infraorbital artery or the descending palatine artery was, in some cases, impossible. Embolizing the sphenopalatine artery alone was achieved in 83 Patients. Non-target embolization of the descending palatine artery was registered in five cases, in three cases, the infraorbital artery, and in four cases, both arteries besides the sphenopalatine artery. In three cases, the whole pterygoid segment of the external carotid artery was embolized.
The used embolization material was PVA particles 150–250 µm. A permanent embolic agent (Bead Block® 500–700 µm, BTG International Ltd., London, UK) was used in only one multimorbid patient showing atherosclerosis of the external carotid artery. In this patient, there was a successful endovascular intervention to stop an epistaxis episode 8 weeks earlier.
The endovascular intervention closed the sphenopalatine artery (group 1 + 2 + 3) in 93 out of 98 patients (95%). However, this led to the stop of epistaxis in only 81.6% (group 1 + 2). This means that in 13 patients, the sphenopalatine artery was not the leading/only cause of epistaxis. Therefore, surgical intervention in clipping the ethmoidal arteries was necessary for these patients to stop nasal bleeding. The surgical intervention for the remaining five patients included clipping the sphenopalatine artery together with the ethmoidal arteries.
Minor complications occurred in 5 of 98 cases (Table 2). Three patients had dysesthesia due to non-target embolization of nearby arteries. The dysesthesia was in the upper lip and cheeks (infraorbital artery). One of these three patients also had numbness in the palate (descending palatine artery). One patient had temporary disorientation, drowsiness, and weakness. Another patient suffered hypoxemia, agitation, and a personality change. This patient was monitored at the intensive care unit for 24 h till these symptoms completely disappeared. The embolization for this patient was performed with general anesthesia. Major complications did not occur in any single case.
Minor and major complications.

Discussion
The choice of which arteries to embolize is in the literature controversially discussed. It was not agreed whether the embolization of the external carotid artery on the ipsilateral side to the bleeding or both sides or in combination with the facial artery, also unilateral or bilateral, would give the best results. The type of embolizing material also differs from one study to the other.
The rich arterial blood supply to the nose makes it sometimes necessary to embolize more than one artery. Sokoloff used gel foam in his case presentation from 1974 to embolize the external carotid artery. 15 Then in 1977, the embolization of the ipsilateral facial artery together with the sphenopalatine artery using gelfoam was described. 16
Wehrli et al. 14 reported better results (74% success rate) by embolizing the ipsilateral maxillary artery using PVA. However, minor complications occurred in 50%, and major complications in 11%. Vitek suggested in 1991 the embolization of the maxillary artery, and if, after 15 min, the nasal bleeding did not stop, he advocated embolization of the facial artery on the ipsilateral side. Through this protocol, he could raise the success rate from 87% to 97%, and the complication rate was 3%. 13
Oguni et al. described in 2000 a retrospective analysis of the embolization of the facial artery on the ipsilateral side or the external carotid artery on the contralateral side if they show on the initial angiogram a collaboration in the arterial supply to the bleeding area. He reported a success rate of 94.6%. 17
Based on multiple case reports and systematic reviews, it can be concluded that the success rate can increase by the embolization of the facial artery on the ipsilateral side or the external carotid artery on the contralateral side, from 74%–84% to 88%–97%. 18 With the same technique, Tseng et al. 11 reported in 1998 similar results of immediate success of 93% and long-time success of 88%. 11
Gottumukkala et al. measured in 2012 the correlation between the number of embolized arteries and the increase in the success and complication rates. He found a direct relationship between both. 18 No minor complications occurred when only one artery was embolized, but did occur in17% in the case of embolization of two arteries, 34% in the case of three arteries, and 56% when four arteries were embolized.
In the systematic review of Smith TP 2006 (1994–2005), of a total of 736 procedures on 690 patients, the complication rate was 3%. 19
The newer systematic review by Dubel et al. 20 (1984–2012) with a total of 1033 procedures on 977 patients showed minor complications in 20% and major complications in 2.5%.
The embolization was regarded to be successful in our study when there was no bleeding after removing the nasal tamponade and till 14 days after the endovascular intervention.
Our objective was only to embolize the external carotid artery on the bleeding side. The embolization was performed on both sides due to bilateral epistaxis for only one patient. The epistaxis was treated merely by endovascular intervention in 80 out of 98 patients. The remaining 18 patients underwent surgical interventions to stop nasal bleeding.
The endovascular intervention was technically successful in 95% of cases in closing the sphenopalatine artery. This technical success led to a clinical stoppage of bleeding in 81.6%. This result is similar to the latest systematic review by Dubel et al. in 2013, with a success rate of 87%. In addition, minor complications were registered in only five patients, with no single case of major complications. This complication rate is lower than in any other study on comparable patient counts. 20
In most studies, embolization has been reserved for refractory cases where surgical interventions failed to stop epistaxis. At our clinic, the endovascular intervention was the first treatment option for severe epistaxis refractory to other conservative therapies. Elden et al. 21 also advocated this sequence of therapy in 1994.
The endoscopic surgical approach to treat refractory epistaxis was directly compared with the endovascular approach in the study of Strong et al. He found similar effectiveness of both approaches (89% for the endoscopic surgical approach versus 94% for embolization). 22
Cullen and Tami 8 compared the ligation of the maxillary artery with its embolization and reported similar success rates (73% and 79%, respectively) without significant differences in the occurrence of major complications.
Siniluoto et al. 23 reported in 1993 that a success rate of (75%) of endovascular treatment in patients with severe epistaxis failed to be stopped through a previous surgical approach. While Elahi et al. 24 reported a success rate of (86%) after failed surgical treatment. 24
Dubel et al. published a literature review for all studies involving endovascular treatment in epistaxis. It showed a success rate of 87%, a minor complication rate of 20%, and a major complication rate of 2.5%. He found these results very acceptable and concluded that the endovascular approach could be used as an alternative to usual surgical methods and not only in case of surgical failure. 20
Limitations
A reassessment of the success of embolization was performed only 14 days after the intervention. A follow-up appointment in 2 and 6 months intervals would have helped to gain results for long-term success. Unfortunately, it was impossible to gain such data in this retrospective analysis.
A sample size/power analysis size calculation was not performed at the beginning of the study.
A direct comparison between endovascular embolization and surgical intervention was not performed. Therefore, this does not allow a reliable prediction regarding invasiveness, safety, or superiority.
The endovascular approach is very technique sensitive and needs a skilled interventionalist aware of the regional anatomy and possible anastomosis. That is why results could be very different in different medical institutions.
Conclusion
Embolization is a minimally invasive treatment option in cases of refractory epistaxis. It is mainly performed under local anesthesia, making it more suitable for multimorbid patients. Although the endovascular intervention showed outstanding results in treating refractory cases of epistaxis with a very low complication rate, it is used in many institutions in case of failure of other surgical measures.
Based on our experience, we recommend endovascular intervention as an alternative to surgical procedures and not only as a reserve treatment option in case of surgical failure. Surgical interventions are important because an endovascular intervention is not always applicable, as shown in this study. Initial angiographs showing bleeding from ethmoidal arteries or anastomosis between external and internal carotid arteries contraindicate the use of this treatment method.
Footnotes
Acknowledgements
Departments of Ear, Nose, and Throat Diseases; Head, Neck, and Plastic Facial Surgery; and Communication Disorders (Hearing, Voice, and Speech Disorders), Marburg University, Campus Fulda. Clinic of Diagnostic and Interventional Radiology, Marburg University, Campus Fulda.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was waived by Ethics Committee, Institute of Pharmacology and Toxicology of Julius-Maximillian-University in Versbacher Str. 9, 97078 Würzburg because this is a retrospective study of already archived data in the Clinic. Ethics Committee waiver number: 2019070902.
Informed consent
Written informed consent was neither needed from subjects nor a legally authorized representative (in the case of minors) in this retrospective study. The ethics committee confirmed this. However, informed consent was provided by the department of interventional radiology to collect the data. Only informed consent was obtained from the interventional radiology department to use and analyze the data and angiographs.