
Abstract
Objectives:
This study aims at exploring the knowledge of women of reproductive age who underwent bariatric surgery in Jordan regarding its effect on birth outcomes.
Methods:
A cross-sectional study was conducted on 183 women (aged 15–49) who had undergone bariatric surgery at the Jordan University Hospital in Amman, Jordan, between 2016 and 2019, using telephone interviews with conveniently selected participants’ samples. The survey tool obtained data on women’s knowledge and other sociodemographic, obstetric health, and bariatric surgery information. Unfavorable birth outcomes include preterm delivery, small for gestational age, congenital abnormalities, low birth weight, and admission to the neonatal critical care unit.
Results:
More than half of the participants did not know about the possible unfavorable birth outcomes after bariatric surgery and related practice guidelines. This is shown in their median score of 3 (interquartile range: 2–4) out of a maximum possible score of 8. Women who had a good score (>4) had received counseling about unfavorable bariatric surgery outcomes from their surgeon (p < 0.013); those who had educational qualifications higher than secondary school (p < 0.001) as well as those who were employed (p < 0.008) and believed that the surgery would affect the newborn (p < 0.001). The median score was also unfavorably associated with the parity of the participants (p < 0.003).
Conclusion:
The extent of knowledge regarding the unfavorable birth outcome of bariatric surgery is low among women who underwent bariatric surgery at Jordan University Hospital in Jordan. Improving health literacy and information on bariatric surgery implications on pregnancy and birth outcomes amongst women of reproductive age is a recommendation from this study.
Introduction
Obesity has become one of the most significant public health issues and is considered one of the greatest risk factors for premature adult death, morbidity, and disability. 1 Worldwide, about 650 million adults have obesity (11% of the total male population and 15% of the total female population), and obesity affects 41 million children.1–7
Obesity during pregnancy has its own issues, including increased risk of gestational diabetes, hypertension disorders, delivery by cesarean section, delayed delivery, and fetal macrosomia. 8 On the other hand, obesity can also triple the risk of infertility.8,9 Women with morbid obesity who failed to achieve weight loss using conservative measures can undergo bariatric surgery (BS) to lose weight and improve their general well-being. 4 Studies show that women accounted for 80% of BS patients, and 50% were of reproductive age (ages 15–49)4,10 and BS surgery the role of BS as a teratogen had support.4,11 Women who become pregnant after BS have a reduced risk of obesity-related co-morbidities.12,13,14,15 There is a risk of pregnancy following BS, particularly after combined bariatric (bypass) surgery and before 12 months. Nevertheless, changes in gut anatomy and physiology with the potential for malnutrition have been identified as having an increased potential for adverse perinatal outcomes such as small for gestational age (SGA), preterm delivery, and congenital defects, which eventually lead to perinatal mortality.15,16
Reproductive-age women with a BS history should be given specialized preconception, antenatal, perinatal, and postpartum care.15,16 According to the American College of Obstetricians and Gynecologists (ACOG), pregnancy after BS should be delayed for at least 12 months, and women who wish to undergo BS should be aware of the unfavorable birth outcome and related guidelines after undergoing BS.17,18 In this instance, the phrase “unfavorable birth outcome” refers to newborns who had at least one of the following complications: preterm delivery, SGA, congenital defects, low birth weight (LBW), and admission to the neonatal intensive care unit.17,18 However, data are scarce regarding women’s knowledge regarding unfavorable birth outcomes and BS guidelines before pregnancy. Given the paucity of data, we aim to explore how women of reproductive age who undergo BS are conscious of BS’s events, that is, possible unfavorable effect on the birth outcome. The study also seeks to explore the factors associated with this knowledge, particularly the sociodemographic characteristics of women and obstetric health data and BS information. This article’s main purpose is providing recommendations to enhance counseling. We emphasize the need to decrease weight before pregnancy. However, we underline the necessity of avoiding pregnancy within 12–18 months of BS and using effective contraception throughout this time frame. This enables sufficient time to recover from the decreased nutrient absorption caused by BS. Clinicians can also consider the patient’s age while choosing a BS because malabsorptive BS is more likely than restricting BS to result in an unfavorable pregnancy outcome.
Methods
Study settings
Jordan is an upper-middle-income country with a population of 10 million.19,20 The country’s literacy rate ranks high, with 96% of Jordanian women considered literate. 21 The present study was conducted in Jordan University Hospital (JUH) as it is a teaching, semi-governmental hospital where many services, including BS, are provided for a wide variety of patients. As a result, the BS clinic is often busy, with the BS team attending to 30–60 patients per clinic. Appointments are typically booked either by direct phone contact with the hospital or via referrals from outside JUH. Generally, the patient is counseled and assessed for BS eligibility in the first visit. In this medical visit, any misconceptions regarding the procedure are clarified, and preoperative workup is started once the patient has been determined eligible for BS. Furthermore, the information the women received contained details while undergoing a BS surgery about the natural risk of having a premature birth, or neonatal death or having a baby with congenital defects. After workup is done, the surgery is typically scheduled after 6–12 months; these waiting times could be due to the restricted number of beds in the hospital department, as only 10–15 surgeries are possible per month.
Study design
A cross-sectional design was applied to explore the knowledge of women who underwent BS about its effect on birth outcomes. A cross-sectional design fits the purpose of this study since it captures a specific point in time; additionally, it is quick, easy, and cheap to perform. 22 Data was collected from the participants by telephone interview. Telephone interviews offer improved response quality and opportunities to receive more detailed information.23–27
Study population
Weight loss surgery has been increasing in Jordan since 2016, and the Jordan Medical Association developed standards to ensure the procedures follow international standards. From July 2019 to October 2019, interviews by telephone were conducted among a sample of 183 women of reproductive age who had undergone BS in Jordan, Amman. From a list of women who had had the surgery between January 1, 2016, and May 31, 2019, we identified 410 potential participants. Based on the population size of 410 participants, a margin of error of 5% with a confidence level of 90% with a response distribution of 50% resulted in the minimum sample size of 164 participants, according to the Sample Size Calculator by Raosoft. 28 The sampling technique was convenient sampling. 29 Out of these targeted patient records, 183 women agreed to participate voluntarily through verbal informed consent. The main reasons for having verbal consent in the context of Jordan were as follows:
Subjects’ names were anonymous if the agreement was verbally given and the study posed minimal danger.
In Jordan, obtaining formal consent was not suitable or practicable due to the study’s low risk.
Signing the informed consent form may have legal, social, or economic risks to the subject, for example, for illegal immigrants/refugees.
The investigator verbally described the study to the potential subject, offering all essential information (purpose, methods, risks, advantages, alternatives to participation, etc.) and allowing the subject to ask questions. After this verbal discussion, the potential subject was given a study information sheet and time to contemplate participating. “Sufficient time” varies based on how long it takes to consider procedures, risks, rewards, and alternatives. After the potential subject reviewed the research information page, the Investigator answered any questions. When the subject agreed, the researcher got verbal consent. The criteria included married, single, or separated women of all educational levels aged between 15 and 49 years who had undergone BS and agreed to participate in the study. The exclusion criteria included those women above 49 years of age.
Instrument
Using a structured questionnaire, data were collected by telephone (refer to Supplemental Appendix 1). The questionnaire was developed based on experience and literature reviews and validated by a panel of research and specialty experts from the Family and Community Medicine Department of the School of Medicine, School of Nursing at the University of Jordan, and the BS Department. In addition, the questionnaire was pilot tested on 36 participants. Adjustments were made to the questionnaire based on the pilot study findings. The instrument’s internal consistency was examined to determine the reliability of questionnaire items. To test the reliability of the questionnaire binary variables, the Kuder–Richardson formula was used, with 0 representing no reliability and 1 representing perfect reliability.24,30 The total Kuder–Richardson value was 0.709, indicating a high trustworthiness level. Only one question with a score of 0.6 was left out of the final survey.
The questionnaire covered four sections: sociodemographic status, obstetric health data, BS information, and lastly, the questionnaire examined the extent of knowledge regarding the unfavorable impact on birth outcome. The final part of the questionnaire included eight closed questions regarding information about unfavorable birth outcomes after BS to establish the women’s knowledge about these effects.
Ethical considerations
The present study’s ethical approval was granted by the Institutional Review Board (IRB) at the JUH (approval number: 2019/89). Verbal consent was obtained from all the subjects and subjects’ legally authorized representative (for minor subjects (under 18 years)) prior to the study initiation. This was approved by IRB. All the data obtained from the hospital was kept confidential. The purpose of the study was explained to the participants; their participation was voluntary, they had complete autonomy to withdraw at any time, and all participants gave verbal consent through the phone.
Data collection
After obtaining the IRB approvals from JUH, data was collected between July and October 2019 by telephone interviews. The average length of the interview was approximately 15–20 min. The telephone interviews consisted of two phases: the pre-interview phase and the interview itself. In the pre-interview phase, the researcher introduced herself, identified the study sponsors, explained the purpose and significance of the study, and assured the confidentiality of participants’ responses. The interviewer also mentioned the time needed to conduct the interview; finally, participants were asked whether they were interested in participating or not. In the second phase or the “interview phase,” the survey questions were asked in an identical manner and order during each interview. The respondents were offered to ask any question and were answered adequately by the researcher. When closing off the questionnaire, participants were thanked for their cooperation. After each interview, data was immediately prepared for analysis and was saved in an Excel sheet.
Statistical analysis
The statistical analysis of data was performed using the SPSS 21. Descriptive and inferential analyses were applied to answer the research questions. A scoring system was applied to explore the extent of the women’s knowledge, in which yes responses scored 1 and no responses scored 0. The total knowledge score ranged from 0 to 8 and finally the overall extent of knowledge was measured by the median and the interquartile range (IQR) of the knowledge score. Through a descriptive analysis, the sociodemographic variables, obstetric health data, BS information, and the dependent variable (Knowledge) were interpreted; t-test and analysis of variance (ANOVA) tests were considered for the analysis. However, the dependent variable (Knowledge) was not normally distributed so nonparametric tests were executed. Normality for the knowledge score variable was measured using the Kolmogorov–Smirnov test. 24 Frequency distribution of knowledge items was calculated about the unfavorable birth outcome and breastfeeding after undergoing BS and the related clinical guidelines—followed by the analysis using Kruskal–Wallis test and Mann–Whitney test on the association between knowledge score and main sociodemographic variables and BS variables. The Kruskal–Wallis H test is a nonparametric rank-based test used to compare two or more groups of an independent variable on a continuous or ordinal dependent variable. 31 Occasionally, this test is called “one-way ANOVA on ranks.” It’s a nonparametric alternative to one-way ANOVA that extends the Mann–Whitney U test to more than two groups. The Mann–Whitney test (analogous to Student’s t-test) was also performed to assess the differences in the knowledge score among variables with two independent groups. 25 Kruskal–Wallis’s test (analogous to ANOVA test) was implemented to test the differences in the knowledge score among variables with more than two independent groups. 26 In addition, Spearman correlation27,29 was applied to determine the relationship between the knowledge score and the quantitative variables (obstetric health variables and age).
Results
Knowledge regarding the unfavorable birth outcome after undergoing BS and the related clinical guidelines among participants
After undergoing BS, the participants were asked questions to determine their knowledge score of unfavorable birth outcomes. Table 1 displays the women’s answers reported to the questions assessing such awareness. The median score of women’s knowledge of unfavorable birth outcomes and related clinical guidelines after BS was 3 (IQR: 2–4) of a maximum possible score of 8. Most patients (n = 176, 96%) did not know neonatal death is possible after BS. Only 16 % (n = 30) knew there is an increased risk of preterm birth after surgery. Moreover, only 40% (n = 74) of the respondents recognized increased risk of congenital anomalies after having BS due to the development of nutritional deficiencies, and only 20% (n = 36) said that there is an increased risk of transferring newborns to the Neonatal Intensive Care Unit (NICU) after having BS. The increased risk of delivering SGA infants was judged correctly by only 52% (n = 95). Furthermore, only 26% (n = 47) knew that micronutrient supplements should be taken during breastfeeding after BS. However, most of the women (n = 170, 93%) believed that following the instruction of the surgeon, the obstetrician, and the dietitian decreases the unfavorable outcomes on newborns after surgery, and 83% (n = 152) of the women understood that pregnancy should be postponed for a period ranging from 12 to 24 months after BS.
Frequency distribution of knowledge items about the unfavorable birth outcome and breastfeeding after undergoing BS and the related clinical guidelines (N = 183).

BS: bariatric surgery; BF: breast feeding.
The association between knowledge score and main sociodemographic variables and BS information variables
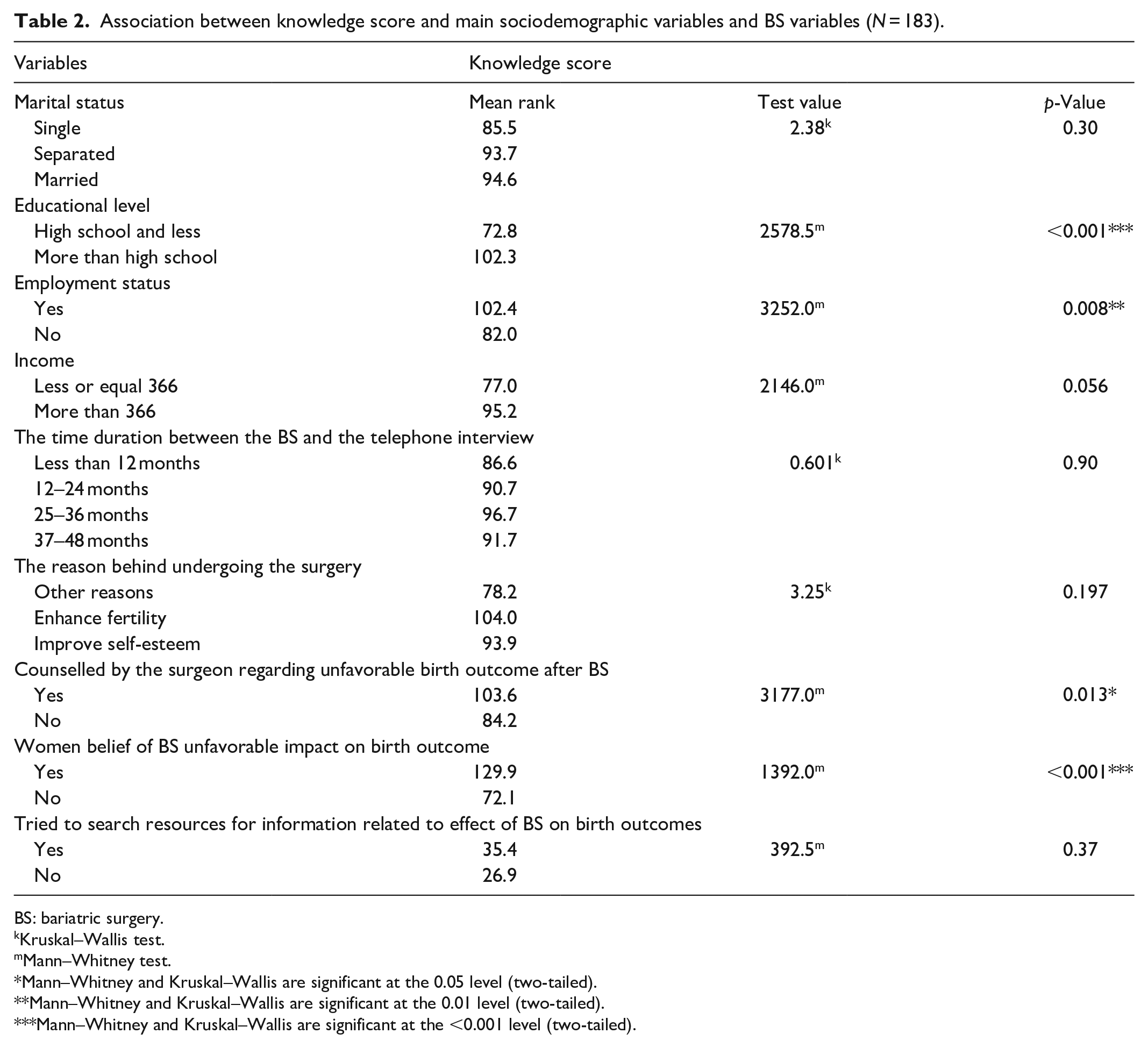
The median of knowledge score was 3 (IQR: 2–4), with a minimum score of zero and a maximum score of eight. The Mann–Whitney test was applied for the dichotomous variables to test the differences in the knowledge score among the variables with two groups. The Kruskal–Wallis test was applied for the variables with three groups or more. In Table 2, a statistically significant difference in the knowledge score was found among women based on their educational level (U = 2578.5, p < 0.001), as indicated by the mean rank of women who had an educational level more than high school scored higher than women who had an educational level of high school and below. Similarly, a statistically significant difference in the knowledge score was found among women based on their employment status (U = 3252.0, p = 0.008) in favor of the working women since they scored higher in the mean rank. Statistically significant differences were also relative to whether the women had received counselling from their surgeons or not. Women who had received such counselling were more aware of unfavorable BS outcomes (U = 3177.0, p = 0.013) and were relative to women who believed that the surgery would affect the newborn (U = 1392.0, p < 0.001). On the contrary, women who reported that the surgeon did not inform them about the risks of the surgery on the newborn did not believe that the surgery would affect the baby. No statistically significant differences were found in the knowledge score based on the marital status, income, the time between the operation from the telephone interview, reason behind undergoing surgery, and the own attempt to search for information related to the effect of BS on birth outcomes.
Association between knowledge score and main sociodemographic variables and BS variables (N = 183).
BS: bariatric surgery.
Kruskal–Wallis test.
Mann–Whitney test.
Mann–Whitney and Kruskal–Wallis are significant at the 0.05 level (two-tailed).
Mann–Whitney and Kruskal–Wallis are significant at the 0.01 level (two-tailed).
Mann–Whitney and Kruskal–Wallis are significant at the <0.001 level (two-tailed).
The correlation between knowledge, age, and related obstetric variables
Despite being small, Spearman rank correlation revealed a significant negative relationship between parity and knowledge (rs(183) = −0.256, p = 0.003). The relationship between age and knowledge (rs(183) = −.048, p = 0.38), gravidity and knowledge (rs(183) = −0.139, p = 0.10), and history of abortion and knowledge (rs(183) = −0.056, p = 0.68) revealed no statically significant relationship. As shown in Table 3. The following categories were applied to the correlation result: little relationship (0.00–0-.25), low (0.26–0.49), moderate (0.50–0.69), high (0.70–0.89), and very high (0.90–1.00). 27
Spearman correlation coefficients between knowledge and age, parity, gravidity, and history of abortion (N = 183).

Correlation is significant at the 0.01 level (two-tailed).
Discussion
Globally, one of the leading maternal and child health parameters is neonatal mortality, which has been recognized as an indicator that directly reflects the quality of prenatal, intrapartum, and neonatal care. According to the United Nations Children Fund (UNICEF), LBW, congenital anomalies, and preterm birth are recognized as potential risks of neonatal morbidity and mortality and hence infant mortality. 19
In Jordan, the neonatal mortality rate has been a priority public health issue for decades. Since the 1990s, the country has implemented essential initiatives to reduce mortality among newborn infants. 6 The results of seven Jordan Population and Family Health surveys conducted between 1990 and 2018 show that the trend in neonatal mortality rate has declined by one-half over that period, from 21 to 11 deaths per 1000 live births. 6
To maintain this achievement, one should look for increasing contributors to the mortality rate, such as BS among women with morbid obesity as potential mothers and mothers of reproductive age. Jordanian women who underwent BS should be made aware of the unfavorable birth outcomes after BS and should be educated about the appropriate time for pregnancy after BS, and the importance of preconception counseling by a multidisciplinary healthcare team after BS.
Women’s extent of knowledge regarding BS effects on unfavorable birth outcome
This study showed that most of the participants (60%) believed that BS does not increase the risk of congenital anomalies. This is consistent with Alqahtani et al.’s study 32 that assessed the awareness and knowledge of the women about the obstetric impact of BS, where their study found that 19% of participants believed that BS did not result in neonatal congenital anomalies and the majority (76%) did not know whether BS had any effect on the nutrition of the fetus. This study also addressed the increased risk of delivering SGA babies after BS. The results indicate that the respondents were not informed about the effect of BS on birthweight, as approximately half (48%) of the participants answered No. A similar pattern of results was obtained in Alqahtani et al.’s study, where most of participants (90%) did not know about the effects of BS on birth weight which agrees with the current study findings. 32 BS and pregnancy are risky for the developing fetus due to weight loss. A small retrospective study found no difference in birth weight between babies born within 1 year of BS and those born more than a year later. 33 Menstrual cycle and hormonal changes occur immediately after BS, leading to spontaneous pregnancy in infertile women. 33 After surgery, there is an increase in SHBG, a decrease in androgens, and an increase in FSH 33 . In a 3-year prospective study involving 29 pregnant women with obesity, Legro et al. found that gastric bypass surgery shortens the follicular phase. 34
Moreover, this study also addressed the knowledge regarding preterm delivery, neonatal mortality, and NICU admission. In this study, most participants did not know that BS can increase the risk of preterm delivery and neonatal mortality (84%, 96%), respectively. Furthermore, 80% of the participants also did not know that maternal BS increases the admission rate of newborns to NICU. According to UNICEF, preterm birth is the leading risk factor for infant morbidity and mortality. 19 The reviewed literature did not reveal studies examining women’s knowledge about the increased risk of neonatal mortality, NICU admission after preterm birth, and BS.
In this study, women were also asked about their knowledge of related practice guidelines about pregnancy and breastfeeding after BS. Women were asked whether consulting healthcare providers could optimize a healthy pregnancy, reduce the unfavorable effects of BS on birth outcomes, and optimize a healthy pregnancy outcome. Most of the participants in this study (93%) believed that the healthcare provider’s consultation could reduce birth outcome complications. This result ties well with previous studies wherein Kallies’ study that assessed patients’ judgments of their primary healthcare providers’ opinion, support, as well as education of BS and changes over time, in 2009 and 2015, a survey was mailed to patients who had undergone Roux-en-Y Gastric Bypass at Gundersen La Crosse medical center, USA. 35 The survey was completed by 319 patients in 2009 and 387 patients in 2015. Patients that completed both surveys were excluded from the study. Kallies’ study results demonstrated that 29% of patients in 2009 and 40% in 2015 considered their primary care physicians as very knowledgeable (p-value = 0.02). 35 In addition to Kallies’ study, Alqahtani et al.’s study also assessed the level of patient adherence to the nutritionist’s guidelines, asking patients about the need of pregnant females to consult a nutritionist after BS; more than half answered that they were encouraged to see a nutritionist. 32 Therefore, it seems that these study findings agree with the literature in so far as health providers being considered a trusted source of information.
In this study, women were also asked the appropriate time of getting pregnant after BS, with 83% of the participants being aware that pregnancy should be avoided for 12–24 months after BS. However, there were 17% were not aware of this. As indicated by both the ACOG and the Jordanian Society of Obesity Surgery (JSOS) guidelines, women should postpone pregnancy for 12–24 months after BS to avoid unfavorable consequences on birth outcomes, which can occur due to rapid weight loss.17,36 In Alqahtani et al.’s study, around 33% of the participants believed that a period of 12–18 months after BS would be appropriate before getting pregnant, while 0.7% thought that getting pregnant in the first year would carry no risks; 66.1% revealed that they did not know the appropriate period. 32 If women who undergo BS were counseled correctly with regards to the practice guidelines, one may reduce the 17% of women who didn’t know about this practice guideline in the current study.
In this study, women were also asked about the importance of micronutrient supplements during the lactation phase to avoid breastfeeding problems after BS, three-fourths of the participants (74%) were not aware that they should take micronutrient supplements while breastfeeding after BS. Breastfeeding after BS is highly recommended and has several benefits for the mother and the baby. 9 World Health Organization guidelines encourage breastfeeding for the first 6 months of a baby’s life, even for mothers who had BS. 9 However, nutrients and trace elements in both the mother and the baby should be monitored, and additional supplements are recommended. 37
It may be concluded that the extent of knowledge regarding unfavorable birth outcomes after BS was low among women in the current study as it was in Alqahtani et al.’s study although knowledge about related practice guidelines was higher among the women in the former. The differences between the findings of this research and those reported by the literature might be due to the surgeon’s proper consultation or related to the order of the questions in the questionnaire, which could have made the participants think logically about these guidelines.
Association between knowledge and sociodemographic characteristics
Regarding the association between sociodemographic characteristics and knowledge score in this study, a statistically significant relationship was found between the knowledge score and educational level (U = 2578.5, p < 0.001) and employment status (U = 3252.0, p = 0.008). In contrast, the association between knowledge and age, marital status, and income was statistically insignificant.
Contrary to the findings of this study, Alqurashi conducted a study to evaluate the knowledge and beliefs about the safety and effectiveness of BS among adults in the Kingdom of Saudi Arabia, and their study revealed that educational levels do not affect the level of knowledge of BS, which conflicts with the current study findings. However, Alqurashi et al. found no relationship between age and knowledge, which agrees with the recent study’s results. 38
Furthermore, a study was also conducted in Saudi Arabia by Abouhamda et al.’s that examined the safety, effectiveness, consequences, and management of BS among the public. The study resulted in showing that there is an association between age and knowledge; however, no association was found between the level of knowledge about BS and income, educational level, and marital status. 39 This is an agreement with our study, except for the results on educational level and age. Abouhamda et al.’s study found that beliefs about BS were not influenced by educational level. 39 Nevertheless, their results showed that the oldest respondents (38.84 years) had the highest knowledge score which is a statistically significant difference (p < 0.05); in contrast to our study, where the results revealed that the age and knowledge relationship was not statistically significant. 39
In addition to Abouhamada et al.’s study and Altaf & Abbas conducted a survey about the public perception of BS in Saudi Arabia among 1129 adult Saudi residents. 40 They concluded that there was a significant correlation between the educational level and knowledge concerning the definition of BS (−0.185, p < 0.001), which concurs with this study’s results. 40
Finally, a study conducted in the Kingdom of Saudi Arabia by Alamri et al. examined the awareness of the complications of BS among the general population. 41 The results of their study showed a significant association between occupational groups and degrees of awareness (p = 0.007), as healthcare providers had the highest level of awareness among the occupational groups, which somehow agrees with this study; whereas, employed women had a better knowledge score than unemployed women. 41 This association is likely due to women sharing their knowledge and experience in their common workplace. Furthermore, employed women are more likely to be more educated and exposed to various sources of information.
Association between knowledge and BS information
A statistically significant relationship was found between the quality of consultation by the surgeon regarding unfavorable birth outcomes after BS (U = 3177.0, p = 0.013) and women’s belief about unfavorable birth outcomes after BS (U = 1392.0, p < 0.001). However, nonsignificant associations were found between other BS information variables (the time duration between the BS and the telephone interview, the reason behind undergoing BS, and the attempt to search resources for information related to the effect of BS on birth outcomes).
In this study, most of the surgeons who performed BS did not inform the patients about the unfavorable birth outcomes of the surgery: 60% of the participants answered No to this question. Therefore, the results of this study show that the surgeons who perform BS do not appear to educate patients comprehensively. On the other hand, surgeons cannot be solely held accountable; according to JSOS guidelines for BS, patients must go through different counseling phases with a multidisciplinary specialist team, including a physician or nurse specializing in weight management and certified nutritionist and psychologist. 36 During this evaluation period, the patient should be instructed about the unfavorable impact of surgery, including pregnancy-related complications. 36 Unfortunately, this is not the case in JUH; here, the patients often refuse to go through the long counseling process and prefer to move forward to the last phase of the process, which is the BS clinic. Another reason for this could be the high volume of patients per clinic (30 to 60 patients).
Although healthcare providers usually assume that the explanations and instructions provided to patients and families about health are willingly and fully understood, these spoken and written instructions have insufficient clarity and quality. 42 The communication skills of healthcare providers have been associated with health outcomes resulting in significant errors. Studies show that patients need clarification and definition of terms, demonstration, a touched or sensed example, narratives, and reminder cues. 43 In Alqahtani et al.’s study, 32 most of the participants (73%) had poor knowledge about the obstetric and gynecological impact of BS. Here the authors found that women who consulted with a physician had good knowledge (p < 0.001). 32 Such results agree with the current study, where a statistically significant difference in the knowledge score was found among women who reported that the physician informed them about the risks to the newborn associated with the surgery (U = 3177.0, p = 0.013). 32
Association between knowledge and women’s parity
A significant negative relationship was found between the participant’s parity and knowledge (rs(183) = −0.256, p = 0.003). Obstetric health data was collected in this study to investigate whether the extent of knowledge of women with a previous pregnancy or delivery would differ from those who had not been pregnant, had an abortion, or women with no children. Unfortunately, as far as we know, no studies examined the relationship between obstetric health data and the extent of BS knowledge.
Many factors are associated with an individual’s knowledge of BS. One of the main elements related to knowledge was the physician’s consultation, according to Alqahtani et al.’s study 32 and the results from the current study. Furthermore, educational level was not a significant factor in the previous studies38,39,41 which disagree with the current research. BS is a safe and effective treatment for moderate to severe obesity, supporting other public health initiatives to promote health and reduce disease burden.41,44 In summary, this study could help identify the most susceptible individuals with a low level of knowledge so they can be specifically targeted to be educated in the future.
Limitations and strengths
Pregnant women who have had BS should have a multidisciplinary follow-up to ensure the best outcome for both mother and child. Informed consent should be obtained from patients prior to surgery. 33 As with most observational studies, this study has limitations, firstly and mainly, the location of the study, as the experiences that the females face can change based on the hospital setting, geography, or even country. No information was gathered on individuals who got pregnant following BS; thus, only a few, such as those who became pregnant, may have had more specific indications. The questionnaire was given to women of reproductive age. The study did not evaluate the positive aspects of BS on pregnancy. This evaluation could have given a more comprehensive view of women’s knowledge about BS. Furthermore, there is no correlation between the type of surgery and knowledge of adverse events. Another drawback that should be considered is the recall bias, as approximately half of the patients (41%) had undergone BS 12–24 months before the telephone interview, which might subject the participants to such a tendency. Therefore, due to the limitations, the results of this study should be interpreted with caution. Still, this study appears to be the first known study in Jordan to assess the knowledge of women concerning potentially unfavorable birth outcomes after BS. Another strength of this research is the validation of the questionnaire and the pilot testing before the initiation of the study.
Conclusion
This study suggests limited knowledge regarding the potentially unfavorable birth outcome after BS, as shown by the sample of JUH patients. In this study, the main reasons behind this lack of knowledge were the little information received by the patients about the risk of birth outcome complications after BS by the surgeon, as well as the low perceived threat by the patients, who did not believe in the negative impacts of BS on birth outcomes. Furthermore, the study findings confirmed that employment status and educational level significantly affected the risk-awareness score. Finally, the results revealed a significant inverse relationship between parity and knowledge regarding unfavorable birth outcomes after BS, where women with no children had greater understanding than women who already had children. This study addressed several areas that need further research. We recommend more studies conducted in Jordan regarding BS from different perspectives as no research on BS and pregnancy outcomes has currently been published.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231158017 – Supplemental material for Knowledge of Jordanian women of reproductive age who underwent bariatric surgery and its effect on birth outcomes: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121231158017 for Knowledge of Jordanian women of reproductive age who underwent bariatric surgery and its effect on birth outcomes: A cross-sectional study by Zainah Assaf, Hana Taha, Immanuel Azaad Moonesar, Firas Obeidat, Eman F Badran, Mazen Al-Nabelsi and Raeda Al Qutob in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231158017 – Supplemental material for Knowledge of Jordanian women of reproductive age who underwent bariatric surgery and its effect on birth outcomes: A cross-sectional study
Supplemental material, sj-docx-2-smo-10.1177_20503121231158017 for Knowledge of Jordanian women of reproductive age who underwent bariatric surgery and its effect on birth outcomes: A cross-sectional study by Zainah Assaf, Hana Taha, Immanuel Azaad Moonesar, Firas Obeidat, Eman F Badran, Mazen Al-Nabelsi and Raeda Al Qutob in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank the Institutional Review Board of the University of Jordan for giving us the opportunity to use information from the University of Jordan Hospital Database.
Author contributions
RJQ conceived the presented idea and supervised the project. FWO gave technical support and EFB contributed conceptual advice. HT contributed to the drafting of the final manuscript. MA-N was involved in the data collection. ZGA and IAM carried out the project, and acquired, analyzed, interpreted the data, and drafted the manuscript. All authors contributed to the writing of the manuscript, provided critical feedback, participated in the research and analysis, and edited and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclose receipt of the following financial support for the authorship, research, and/or publication of this article: The authors would like to acknowledge Mohammed Bin Rashid School of Government, Dubai, UAE, and the Alliance for Health Policy and Systems Research at the World Health Organization for financial support as part of the Knowledge to Policy Center Mentorship Program [BIRD Project].
Ethics approval
The present study’s ethical approval was granted by the Institutional Review Board at the JUH (approval number: 2019/89).
Informed consent
Verbal consent was obtained from all the subjects and subject’s legally authorized representative [for minor subjects (under 18 years) prior to the study initiation. This was approved by Institutional Review Board (IRB). The main reasons for having verbal consent in the context of Jordan are as follows:
The subjects’ identities have been completely anonymous if the consent form was not signed, but provided verbally and minimal risk involved in the study. In the context of Jordan, obtaining signed consent was not appropriate or feasible according to the cultural standards of the population being studied, and there is minimal risk involved in the study. There is a possible legal, social, or economic risk to the subject entailed in signing the consent form, for example, for immigrants who might be identified as being illegal aliens/ refugees.
Based on the approved IRB, the Investigator explained the study to the potential subject verbally, providing all pertinent information (purpose, procedures, risks, benefits, alternatives to participation, etc.), and allowed the potential subject ample opportunity to ask questions. Following this verbal explanation, the potential subject was also provided with a study information sheet and was afforded sufficient time to consider whether to participate in the research. “Sufficient time” can range from minutes to hours, dependent on how long it reasonably takes to evaluate the procedures, risks, potential benefits, and potential alternatives. After allowing the potential subject time to read the study information sheet, the Investigator answered any additional questions the potential subject may had. When the subject was satisfied, the investigator obtained verbal agreement to participate in the research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.