
Abstract
Objectives:
Intoxication with pesticides is a well-known public health problem. We aimed to describe the demographic and toxico-clinical characteristics and outcomes of patients with pesticide poisoning.
Methods:
This retrospective cross-sectional study was performed in Khorshid Hospital affiliated with Isfahan University of Medical Sciences, Isfahan, Iran. All patients with pesticide poisoning (insecticides, herbicides, fungicides, rodenticides, and acaricides) were evaluated. The patients’ demographic, toxicological, clinical, and laboratory findings from March 2016 until March 2021 were collected and analyzed.
Results:
During the study period, 25,659 patients with acute poisoning were admitted, of which, 1567 (6.1% of the total poisoning) with pesticide poisoning were included. The mean ± SD age of the patients was 31.34 ± 13.7 years and 55.3% were men (male/female ratio = 1.23). In approximately 75% of the patients, poisoning occurred by suicidal attempts, while in 14.3% (n = 224), it was accidental. Insecticides caused about 51.30% of the poisonings. However, rodenticides were most commonly used in completed suicide attempts (79.9%). The frequency of previously attempted suicide, and self-harming was different among the patients with respect to the type of pesticide poisoning (p < 0.05). Previous suicidal attempts (35.3%) and self-harming (17.3%) were reported more in patients poisoned with the combination of pesticides. Half of the patients were employed. Nausea and vomiting (56.7%, n = 889) were the most common clinical manifestations; 8.3% (n = 130) of the patients died, 64 of whom had rodenticide poisoning.
Conclusion:
The prevalence of pesticide poisoning was relatively low; most were insecticide poisoning. Poisoning occurred most through attempted suicide. Rodenticides and herbicides had higher mortality rates than other pesticides. Patients with previously attempted suicide and self-harming behavior may use a combination of pesticides.
Introduction
Pesticides have been used by farmers to control agricultural weeds and eliminate rats and vectors such as mosquitos. They include a wide range of products, such as insecticides, herbicides, fungicides, and rodenticides. 1 There has been a steady increase in pesticides marketed for agricultural use worldwide.2,3 Despite the benefits of pesticide use in increasing agricultural production, there have been growing concerns over the adverse effects of unsafe and inappropriate handling of pesticides on human health. 4
In many developing countries, intoxication with pesticides is a well-known public health obstacle.5–7 Indeed, the incidence of pesticide poisoning is estimated to be higher in low- and middle-income countries than in developed countries because of inadequate regulations in purchase and sale, absence of monitoring systems for increasing the general public’s knowledge, low enforcement, lack of training for farmers, insufficient availability of information systems, lack of personal protective equipment, and large agricultural-based populations.8,9 About 1 million cases of unintentional poisoning with pesticides occur annually with severe manifestations, leading to about 20,000 deaths. 10 Moreover, more than 168,000 people die from pesticide self-poisoning every year and the problem is more severe in rural communities. 6 Unintentional poisoning has been observed in more than 4.8 million people per year in the healthy population, of which pesticides comprised a noteworthy percentage. 5 However, the number of nonfatal cases of pesticide poisoning is anticipated to be much higher because of underreported cases. 11 One-seventh of the total number of suicides worldwide was related to pesticide self-poisoning. Among the low- and middle-income countries, the suicide rate due to pesticide self-poisoning is high in agricultural areas, contributing to 30% of the world suicide rate.12,13 Suicide by pesticide is most prevalent in South Asia, South East Asia, and China. 11 On the other hand, death due to unintentional pesticide poisoning is covered mostly by three countries in Southern Asia (India, Iran, Maldives) with 70% of the population in these areas. 10
In Iran, there are more than 500 different pesticide compounds available for agricultural uses. 14 Pesticides were the third most common cause of poisoning and the main cause of poisoning-related mortality in Iran. 14 Dehghani et al. 15 described that Tehran and Isfahan consumed 32.2% of the pesticides in the country. Poisoning with some pesticides has been common in our poisoning referral center including paraquat and phosphides with high mortality.16,17
Despite advanced medical treatment and awareness, deaths due to poisoning are increasing. The knowledge of the general pattern of poisoning in a particular region may lead to early diagnosis and control of poisoning crises, thereby decreasing morbidity and mortality rates. 18 Therefore, we aimed to determine the demographic, toxico-clinical characteristics, and outcomes of admitted patients with pesticide poisoning during 2016–2021 in the referral Poisoning Emergency Center in Isfahan Province, Central Iran.
Methods
Study design and setting
This retrospective cross-sectional study was performed in Khorshid Hospital affiliated to Isfahan University of Medical Sciences, Isfahan, Iran. The Poisoning Emergency Department of Khorshid Hospital is a main referral center for poisoning cases in Isfahan, Central Iran. It is specifically staffed and designed exclusively for the management of poisoned patients. Patients were admitted from both primary health-care facilities as well as direct admissions. Both adult and pediatric poisoning cases admitted to the Poisoning Emergency Center. Approximately 600 patients are admitted monthly, and their initial care is managed under the supervision of a medical toxicologist and the involvement of anesthesiology, intensive care, and forensic medicine specialists. Khorshid Hospital has about 280 beds including different units such as intensive care unit, as well as medical toxicology, internal medicine (gastrointestinal, kidney, pulmonary, rheumatology), urology, cardiovascular, and psychiatry subdivisions.
The sample size for estimating incidence of pesticide poisoning was determined based on the following formula: by considering the pesticide poisoning incidence rate from previous studies as p = 0.04, type one error rate α = 0.05 (Z = 1.96) and precision d = 0.01 resulted 1474 samples. We finally analyzed data from 1567 people.19,20

Inclusion and exclusion criteria
All patients (adult and children) with pesticide poisoning (insecticides, herbicides, fungicides, rodenticides, and acaricides) admitted to the Poisoning Emergency Center of Khorshid Hospital between March 2016 and March 2021 were included. The exclusion criteria were discharge against medical advice and incomplete medical records.
Data collection
Patients were managed under the supervision of medical toxicologists in the hospital. The medical files of the patients who met the inclusion criteria were extracted based on ICD-10 codes for pesticide poisoning. Data were collected in the data spreadsheet from medical records by medically trained staff and medical research assistants. Patients’ information including age, sex, occupation, type of exposure (intentional, homicidal, accidental including occupational, unaware (patients who were poisoned by another person without homicidal purposes), unknown (do not know the substance’s name)), history of addiction, type of addiction (alcohol, cigarettes, methadone), medical history related to psychiatric illness, history of medical problems (diabetes mellitus, hypertension, cardiovascular disease), clinical manifestations (sign and symptoms) on admission including vital signs (blood pressure, temperature, respiratory rate, pulse rate), laboratory findings, the length of hospital stay, and outcome were included in the data collection form. All kinds of cardiovascular complications (bradycardia, tachycardia, QT interval changes, PR changes, and arrhythmias obtained by referring to the ECG recorded in the patient file) were defined as abnormal cardiovascular manifestations. Also, physical chest examination including inspection, palpation, percussion, and auscultation as well as bradypnea, tachypnea, and apnea were considered as abnormal respiratory manifestations. Pesticides were categorized as insecticides, herbicides, fungicides, rodenticides, acaricides, combination pesticides (more than one pesticide), and unknown pesticides (history of pesticide contact through ingestion, skin, injection, and eye without knowing its name). The outcome was defined as survival or death. Pesticide poisoning had been confirmed by the patient’s history, the container containing the poison, clinical manifestations, serological and toxicological tests (determination of serum cholinesterase activity for organophosphate poisoning 21 and urine sodium dithionite test 22 for paraquat poisoning), and bedside urine toxicology screening test 23 were recorded if available.
Ethical considerations
The study protocol was approved by the Ethical Research Committee of Isfahan University of Medical Sciences (Code: IR.MUI.MED.REC.1397.292). Written informed consent was obtained from the patients (or their parent or legally authorized representative in the case of children under 18 years of age). Written informed consent from a legally authorized representative (LAR) of deceased subjects was not taken, as it is not a rule in our hospital to get a written consent from LAR for deceased subjects and also this was approved by the Ethics Committee.
Statistical analysis
Data were analyzed using SPSS software, version 15 (SPSS Inc., Chicago, IL, USA). Results were presented as frequency (%) or mean (standard deviation (SD)) and median (minimum, maximum). Categorical data were compared using Fisher’s exact and Chi-square tests where appropriated The means of variables were compared using two-way repeated-measure analysis of variance (ANOVA) or independent t-test. p < 0.05 was considered as statistically significant.
Results
During the study period, 25,659 patients with acute poisoning were admitted, including 1567 (6.1% of total) patients with pesticide poisoning who were included in our study. Of all our cases, 91.7% survived and 8.3% died. The toxicology and demographic variables of the studied population based on pesticide types is shown in Table 1. Poisoning with insecticides was the most common type of poisoning (51.30%). A significant difference was seen among the patients based on type of pesticide in different age groups (p = 0.002)
Demographic information related to pesticide poisoning patients.

Frequency distribution was analyzed with Fisher’s exact* or Chi-square tests where appropriate. The ANOVA test was used for mean comparison. The p-value less than 0.05 was considered statistically significant.
The mean ± SD age of the patients was 31.34 ± 13.7 years of whom 55.3% were men (male/female ratio = 1.23, range: 1–97 years). Most patients were married (n = 1065, 68%). Regarding the season in which poisoning has occurred, summer and spring accounted for 26.9% and 26.5% of the cases, respectively. Most of the patients had an education level of diploma or under diploma (26.1%); 50% of the patients were employed and 2.7% were farmers. The most and least common route of exposure was ingestion and injection (95.3% and 0.6%, respectively); 74.4% (n = 1171) of the poisonings occurred by suicidal attempt, while 14.3% (n = 224) were accidental. Rodenticides were most commonly used in suicidal attempts (79.9% of cases). According to our results, pesticide intoxications mainly happened at home (56%, n = 877); 22.5% had an addiction history and 33.9% were addicted to cigarette smoking. Patients with a history of psychiatric problems accounted for 17.4% (n =272 ) of the cases while 17% (n = 267) reported previous suicidal attempts. Information regarding the route of exposure, clinical information, and outcome of pesticide poisoning are shown Table 2. The most common clinical symptoms were nausea and vomiting (56.7%, n = 889). The frequency of endotracheal intubation, pupil size, and abnormal respiratory system in patients were significantly different among different types of pesticides.
Route of exposure, clinical information, and outcome in pesticide poisoning patients.
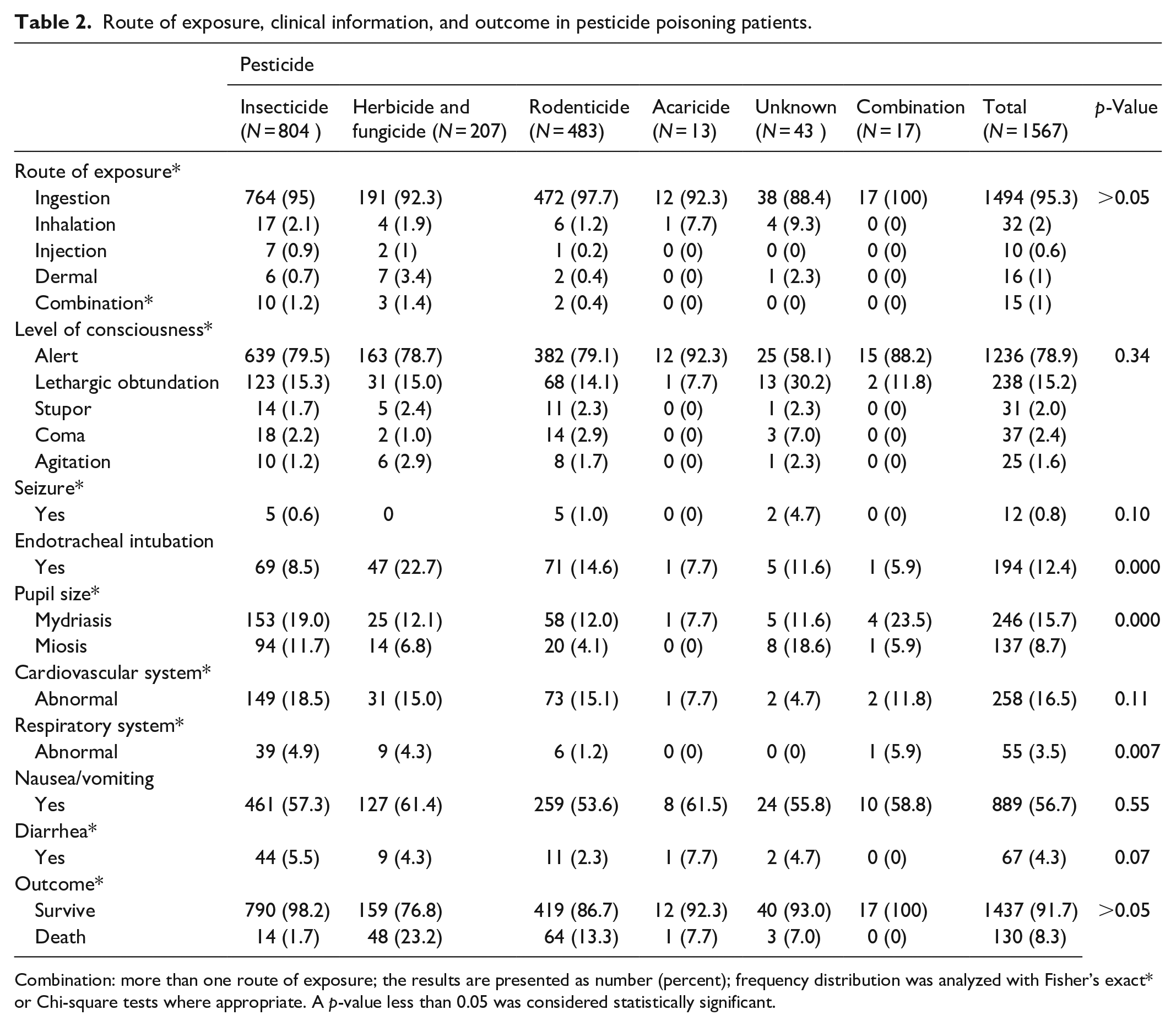
Combination: more than one route of exposure; the results are presented as number (percent); frequency distribution was analyzed with Fisher’s exact* or Chi-square tests where appropriate. A p-value less than 0.05 was considered statistically significant.
Mostly due to rodenticide poisoning (n = 64), 8.3% (n = 130) of the patients died. However, with respect to mortality based on the kind of pesticide, mortality was higher in patients with herbicide poisoning (about 23.2% patients, Table 2).
The distribution of pesticide poisoning cases over the 5-year period is shown in Figure 1. The frequency of pesticide poisoning had decreased during the study period. Most poisonings occurred in 2016. The frequency of addiction, previous suicidal attempts, and self-harming was different with respect to the type of pesticide poisoning (p < 0.05). Previous attempted suicide (35.3%) and self-harming (17.3%) were reported more in patients who were poisoned with a combination of pesticides. However, there was no relationship between the kind of addiction (including alcohol) and self-harm (p > 0.05). In addition, job status had a strong association with pesticide poisoning (p < 0.000). Most of the patients were employees (50%).
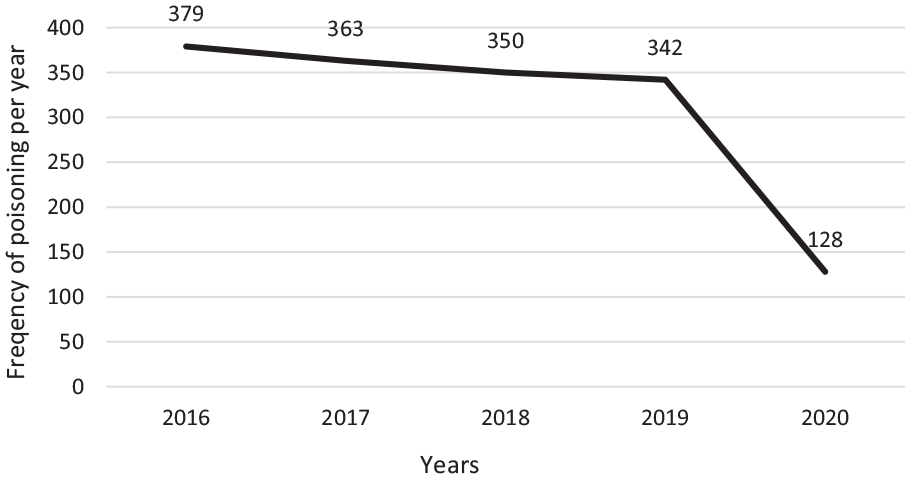
Number of pesticide poisoning cases per year.
Most of the patients were alert (78.87%) with normal respiratory (96.5%) and cardiovascular manifestations (83.67%) upon admission; 0.76% of the patients had seizures on presentation. Figure 2 shows the distribution of clinical signs among the patients. The most frequent sign was abnormal pupil size (24.4%, n = 383); 194 (12.4%) patients were endotracheally intubated; 81(41.7%) of patients were intubated upon admission. Regarding treatment, 63.62% and 73.13% of the patients underwent gastric lavage and received activated charcoal, respectively.

Distribution of clinical signs among pesticide poisoning patients.
Discussion
In this study, we recorded 1567 pesticide-poisoned patients during 2016–2021. The total number of acute poisonings was high during the study period. Generally, the ongoing increase in the incidence of poisoning in different countries can be explained by the change in lifestyle, socioeconomic status, cultural factors, and religious beliefs in the society, as well as by the easy access to highly toxic agents, such as pesticides, therapeutic drugs, and other chemicals. 11 Our results showed a dramatic decline in the number of pesticide-poisoned patients in 2020 when compared with number of patients in 2016–2019. This is due to the general increase in the use of pesticides in agriculture, therefore making them more accessible in the market before the COVID-19 outbreak. Studies from Peru, Serbia, and Turkey suggest a decrease in the number of patients presenting with self-harm to hospitals and suicide deaths during COVID-19. Also, the increase in social integration during nationwide disasters such as COVID-19 outbreak may result in a reduced incidence of self-poisoning.24–26
Of all our cases, 8.3% died. Pesticides are more lethal than other agents commonly used for self-poisoning such as analgesics and sedatives. 27 The fatality rate due to pesticide poisoning was 5.5% in China during 2007–2016. Reportedly, developing countries have a high mortality rate with respect to pesticide poisoning, which may be attributed to the high toxicity of locally available poisons, the significant delay in transferring patients to the hospital, insufficient number of health-care providers, and the lack of facilities and antidotes. The prevalence of pesticide poisoning varies among different regions. 1
Despite the efforts to improve the safety of pesticide use, acute pesticide poisoning remains a major global health problem. 10 In our study, suicide attempts accounted for 74.4% of such poisonings. This rate is high compared with previous reports,28,29 but it is similar to other estimations reported from Iran. In 2017, during a 7-year study in Gorgan, Shokrzadeh et al. 30 reported 89.7% of pesticide poisoning cases that occurred following suicidal attempts. Studies have shown that globally, less than 800,000 people die because of suicide per year. 31 Suicide is a common cause of emergency hospitalization. 32 The suicidal rate varies between different regions of Iran, from 16.8 in the south to 117.8 (per 100,000) in the north. 33 Also, pesticides are a common method of suicide in a large number of developing countries.4,6 These data are consistent with reports from the World Health Organization (WHO) which found pesticides to be the major method of suicide, especially in Asia. 13
In some countries, the fatality of self-poisoning with pesticides is decreasing, which may be attributed to the introduction of laws that had forbidden the use of highly toxic pesticides in agriculture, the measure which also proved efficient in other countries.34,35 However, the high rate of self-poisoning may be related to different reasons such as the increase in unemployment, urbanization, the breakup of the family support system, and economic problems.36,37 It could also be explained by some recent changes in culture and beliefs, especially among youth. 38
The male predominance in our study is corroborated by previous pesticide poisoning research.12,39–42 This trend may be attributed to the greater stress, occupational hazards, and the better accessibility of poisons for men.12,43–45 Most of the agricultural and other occupational activities are done by men in our country, therefore, more pesticide poisoning in men may be because of higher occupational pesticide exposure. 40 Some studies showed female predominance 4 and some others did not find a significant association between sex and pesticide poisoning.34,46 On the other hand, men may have a higher mortality rate compared with women which is consistent with the literature. 47 These results are not far from mind in Iran where most agricultural activities are done by men, thus enabling more vulnerability to pesticide poisoning. 11 Another reason for this difference is that suicidal acts are more lethal in men than in women. 48
This study revealed that employees and homemakers accounted for a higher percentage of patients, and occupational poisoning was due to agricultural activities comprising only a tiny proportion of the cases, which is consistent with previous reports. In a study done by Islambulchilar et al., 36 homemakers constituted the largest proportion of poisoned patients. According to Table 1, few farmers were poisoned, although farmers are more vulnerable to toxic chemicals. It may be due to strict regulations, regularly monitoring systems, educational programs, and increased farmers’ awareness of pesticides’ toxicity. Gyenwali et al. 4 also reported that occupational pesticide poisoning made up only a tiny number of poisoning patients.
Based on our results, history of previous attempted suicide, and self-harming had a significant association with pesticide poisoning. 17.4% of our patients had a history of psychiatric problems. Substance use disorder is a risk factor for suicide behavior.49,50 Also, patients with depression or people who face negative perceptions of life, are in danger of committing suicide. 11 It was reported that depression was observed to be associated with poisoning. 43 Others reported that the risk of poisoning and suicidal attempts was higher in patients who were taking or were recently prescribed antidepressants. 51 Based on WHO recommendations, early recognition and treatment of mental illnesses are one of the most important strategies for the prevention of poisoning and suicidal attempts. Mental problems are found less frequently in Asia compared with Western countries. One explanation for this difference is that a more significant proportion of deaths in Asia result from the use of highly lethal pesticides in impulsive acts of self-harm. Nevertheless, mental disorders are found in a great proportion of Asian suicides. Hence, it is thought to play an important role in suicidal behaviors, underlining the role of psychiatrists and other mental health workers in these settings. 12
In our study, most clinical manifestations were related to the gastrointestinal system and ocular signs. In another study, the most common manifestations among workers with pesticide poisoning were respiratory, ocular, gastrointestinal, and dermal. 52 In a cohort study in Spain, the frequencies of abdominal, ocular, and skin signs were significantly higher in pesticide-poisoned farmers compared with the control group. 53 In a study in Singapore, 60% of acute organophosphate-poisoned patients developed cardiac complications. 54 The difference among these studies may be related to the difference in the kind of pesticides, time from exposure to admission, and toxicity severity, as well as the studies’ sample sizes.
As shown in Figure 2, the most common clinical manifestations were nausea and vomiting. In one study, all patients had vomited before being admitted to the hospital and 32% of the patients had abdominal pain. In a study in Jamaica, the most common symptoms reported by pesticide-poisoned farmers were headaches (12%), itching eyes (11%), blurred vision (11%), dry throat (9%), twitching eyelids (7%), and muscle cramps. 41 Ncube et al. 41 also reported burning skin as the most common symptom among pesticide-poisoned farmers. Different type of pesticides, different routes of exposure, and toxicity severity may be the reason for these differences.
In this study, most expired cases were due to rodenticides poisoning. Aluminum phosphide and zinc phosphide are the most important toxic rodenticides. 17 The mortality rate following the ingestion of metal phosphide is estimated to be between 31% and 77%, related to the dose of ingested toxin. 17 Higher availability because of low cost might be the reason for the rate of poisoning. In addition, there is no antidote for treating phosphine gas poisoning. The general treatment principles include supportive management. 55 Although most deceased were from patients poisoned with rodenticides, the mortality according to the type of pesticide was higher among patients poisoned with herbicides, so that 23.3% of patients died. Paraquat poisoning was the most common herbicide poisoning in our center with high mortality. Paraquat poisoning is one of the most serious public health problems in our society. All body systems are damaged in paraquat poisoning due to accumulation of free radicals and apoptosis pathway. There is also no definite treatment for paraquat poisoning.16,56
This study has some limitations. It was a single referral center study and results cannot be generalized to the whole country. Multicenter studies are needed. Also, data quality might have been an issue in the area in our study. We could not overcome this limitation as the nature of the study was retrospective and we had no role in data and quality measurement. In addition, we did not evaluate the impact of the socioeconomic and psychological factors that are important for understanding this type of poisoning. Finally, both adult and children were included in the study. The toxicity severity and the clinical manifestations as well as the outcome may be different in these two groups. Therefore, more studies on different pesticides separating adults and children are suggested. Our results may be useful for developing programs for reducing poisoning fatalities. However, intentional poisoning is preventable by increasing people’s awareness about mental problems and educating them to use pesticides safely.
Conclusion
Self-poisoning with pesticides was relatively low in our province. Insecticides and rodenticides poisoning were the most frequent. Pesticide poisoning was more common in male patients, employees, and homemakers, with previous attempted suicide, self-harming, and addiction. Gastrointestinal complication was the most common clinical manifestation in the patients. Most of the patients survived. Mortality rates in rodenticides and herbicides was higher than other pesticides.
Supplemental Material
sj-xlsx-1-smo-10.1177_20503121221147352 – Supplemental material for Acute pesticide poisoning in the central part of Iran: A 4-year cross-sectional study
Supplemental material, sj-xlsx-1-smo-10.1177_20503121221147352 for Acute pesticide poisoning in the central part of Iran: A 4-year cross-sectional study by Nastaran Eizadi-Mood, Razieh Mahvari, Mahsa Akafzadeh Savari, Ehsan Mohammadbeigi, Awat Feizi, Parisa Mirmoghtadaei, Ramin Sami and Rokhsareh Meamar in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank the colleagues and personnel of the Clinical Toxicology Department and archive staff of Khorshid Hospital for their valuable technical help and general support.
Author contributions
Conception and design: NEM and RM; Data collection: RMa, MS, and RS; Data analysis: AF and NEM; Data interpretation: NEM and PM; Writing the original draft: RM, RMa, NEM, PM, EB, and MS. All authors approved the final version of the article prior to submission. They have agreed to be personally accountable for the author’s own contributions and ensure that questions related to the accuracy or integrity of any part of the work, even the ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to the nature of patients who attempted suicide but are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and informed consent
This research has been performed in accordance with the Declaration of Helsinki and has been approved by the Ethics Committee of Isfahan University of Medical Sciences (Ethical number: (Ethics code: IR.MUI.MED.REC.1397.292)). Written informed consent was obtained from the patients (or their parent or legally authorized representative in the case of children under 18 years of age) “Written Informed Consent from LAR of deceased subjects were not taken, as it is not a rule in our hospital to get a written consent from LAR for deceased subjects and also this was approved by the Ethics Committee.”
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported financially by the Isfahan University of Medical Sciences for the design of the study and collection, analysis, and interpretation of data (Research project number: 297151).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.