
Abstract
Objective:
This study assessed the antimicrobial use-related drug therapy problems (DTPs) among patients admitted to the medical ward of Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital (WCUNEMMCSH), Southwest Ethiopia.
Methods:
A hospital-based prospective observational study design was used to assess antimicrobial use-related DTPs among patients admitted to the medical ward of WCUNEMMCSH from June to August 2021. Data were collected using a structured data abstraction format.
Results:
In all, 128 patients admitted to the medical ward were enrolled. Among the study participants, at least one form of antimicrobial DTP occurred in 98 (76.6%) of them. The most prevalent DTPs were unnecessary drug treatment in 42 (32.8%), the need for additional drug treatment in 36 (28.1%), and non-adherence in 30 (23.4%) of the patients. There were a total of 288 antimicrobial drug orders. Ceftriaxone 120 (41.7%) and azithromycin 69 (24.0%) were the most commonly prescribed antimicrobial drugs. In multivariate logistic analysis, the length of hospital stay (adjusted odds ratio (AOR) = 2.97, 95% confidence interval (CI): 1.06–8.32; p = 0.04) and the number of diagnosed diseases (AOR = 3.10, 95% CI: 1.12–8.15, p = 0.02) were predictors of antimicrobial use-related DTPs.
Conclusion:
Antimicrobial use-related DTPs are common among patients admitted to the medical ward of WCUNEMMCSH. Health professionals should work together to reduce the high prevalence of DTPs among medical ward admitted patients in this hospital.
Introduction
Drug therapy, which is a crucial part of providing healthcare, is extremely important for the diagnosis, treatment, and management of diseases. 1 However, using medications improperly could cause issues with drug therapy problems (DTPs). DTPs, which are undesirable events experienced by patients related to drug treatment, interfere with achieving the desired goals of the pharmacological intervention and require professional and expert decision-making to resolve. 2 Hospitalization, emergency department visits, higher expenses, morbidity, and mortality are some of the effects of DTPs. 3 It is estimated that 5–10% of all hospital admissions and up to 28% of emergency department visits are medication related, 4 with a significant proportion (70–90%) being preventable.5,6
Irrational drug use has also resulted in high extra costs for medical care in Ethiopia. 7 In Ethiopia, the Community-Based Health Insurance (CBHI) initiative was set up as a community-based health project that gathers premium payments made by voluntary community members into a fund that covers basic healthcare costs. The country has been implementing the CBHI scheme as a pilot to increase access to sustainable healthcare. Each participating household gets a CBHI health card that permits healthcare access without having to pay at the time of service. However, if the medication is not available at that institution (shortage of medications due to limited supply), the individual will be liable to purchase the medication out-of-pocket, which contributes to non-adherence to treatment. The financial constraint on the premium rates also affects the sustainability of the CBHI initiatives. Hence, early identification of DTPs and timely interventions to resolve them can improve patients’ health and minimize treatment costs.
Antimicrobial drugs, which are the cornerstones for treating infectious diseases, are the most widely prescribed, dispensed, and used drugs in the healthcare system. 8 Antimicrobial use-related DTPs refer to the inappropriate use of antimicrobial drugs that can affect the health outcomes of patients. 9 It contributes to the spread of drug resistance.10,11 In the United States, among patients receiving outpatient antimicrobial drug therapy, more than 60% of the study participants had at least one form of DTP. 12 DTPs were prevalent in 47.0% and 66.0% of Turkey 13 and Northern Sweden hospitals 9 , respectively.
In developing countries, antimicrobial drugs are the most frequently prescribed drugs. 14 They are also the most commonly reported drug classes in DTPs.15–17 A study at Jimma University specialized hospital showed that antimicrobial use-related DTPs were found in about 70% of the study participants, and incorrect doses were the most common. 7 To our knowledge, there are limited studies conducted on the prevalence of antimicrobial use-related DTPs in the southwest of Ethiopia. Hence, this study aimed to assess the magnitude and patterns of antimicrobial use-related DTPs and to identify the associated factors among patients on antimicrobial drug therapy in the medical ward of Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital (WCUNEMMCSH), Southwest of Ethiopia. Early identification of antimicrobial use-related DTPs and the associated factors may enhance the prevention and management of DTPs. Thus, this study may contribute to better practice in the use of antimicrobial drugs in the study area.
Methods
Study area
This study was conducted at WCUNEMMCSH, in Hossana town, Hadiya Zone, Southern Nations Nationalities People Region. Hossana is 235 km away from Addis Ababa, the capital city of Ethiopia. The hospital is a teaching hospital and serves about 1.5 million people, along with neighboring zones and special woredas. The inpatient service is organized into medical, surgical, pediatrics, and obstetrics and gynecology wards with 250 beds. Outpatient service includes hospital pharmacy, general ambulatory care, emergency department, and antiretroviral therapy clinics that serve the community.
Design and duration of the study
A hospital-based prospective observational study was conducted involving all patients admitted to the medical ward of WCUNEMMCSH, Hossana-Southwest Ethiopia, from June 2021 to August 2021.
Study population
The study population was patients admitted to the medical ward of WCUNEMMCSH from June 2021 to August 2021 who were treated with antimicrobial drugs and fulfilled the inclusion criteria.
Inclusion and exclusion criteria
Inclusion criteria
Adult patients admitted to the medical ward, treated with antimicrobial drugs, and with more than 48 h of stay in the ward were included in the study.
Exclusion criteria
Critically ill patients admitted to the intensive care unit were excluded from the study.
Sample size
All patients admitted to the medical ward during the study period that fulfilled the inclusion criteria and gave written consent were included in the study. This brought the sample size to a convenient sample of 128 patients.
Study variables
Dependent variable: Presence of antimicrobial use-related DTPs
Independent variables: Sociodemographic characteristics, history of recent antimicrobial drug use, comorbidity, the total number of drugs used, length of hospital stay, and number and type of antimicrobial drugs used
Data collection techniques
Using a structured data abstraction format, trained graduating class pharmacy students reviewed the medical records of patients to collect data. Both the national guidelines (the Standard Treatment Guideline for a General Hospital, 18 and Guidelines for Management of Opportunistic Infections and Antiretroviral Treatment in Adolescents and Adults in Ethiopia) and evidence-based international clinical guidelines (Infection Diseases Society of America Antimicrobial Prophylaxis and Therapeutic Guidelines, World Health Organization Guidelines, Pharmacotherapy/Applied Therapeutics textbooks, as well as Medscape online drug interaction checker) were used to evaluate the appropriateness of drug therapy and to assure compliance with the recommendations of the local and international clinical guidelines. The identified DTPs were recorded and classified using the DTP Registration Format, which is based on the Cipolle DTP classification system with slight modifications. 19
A pilot study was conducted on 10 (7.8%) of the study population to ensure the validity of the data collection instruments. DTPs are classified as the need for additional drug therapy, unnecessary drug therapy, ineffective drug therapy, inappropriate dosage, adverse drug reactions (ADRs), and non-adherence. 19
Operational definitions
The need for additional drug therapy: a DTP that occurs when there is a medical condition requiring another drug therapy or preventive therapy is required to reduce the risk of developing a new condition, or a medical condition requires combination therapy for better efficacy.
Unnecessary drug therapy: a DTP that occurs when there is no valid medical indication for the drug at the time or multiple drug products are used while only single-drug therapy is appropriate or the condition is best treated with non-drug therapy.
Ineffective drug therapy: a DTP that occurs when the drug is not the most effective for the medical problem; the drug product is not effective for the medical condition, the condition is refractory to the drug product being used; or the dosage form is inappropriate.
A dose too low: a DTP that occurs when the dose is too low to produce the desired outcome, the dosage interval is too infrequent, a drug interaction reduces the amount of active drug available, or the duration of therapy is too short.
Dosage too high: a DTP that occurs when the dose is too high or the dosing frequency is too short or the duration of therapy is too long for the patient or a drug interaction causes a toxic reaction to the drug product, or the dose was administered too rapidly.
ADR: a DTP that occurs when the drug product causes an undesirable reaction that is not dose related or a safer drug is needed because of patient risk factors, or a drug interaction causes an undesirable reaction that is not dose related or the regimen was administered or changed too rapidly.
Non-adherence: a DTP that occurs when the patient does not understand the instructions or the patient prefers not to take or forgets to take the medication.
Quality assurance of data
To assure quality, data were collected by three trained graduating class pharmacy students who had the basic knowledge of pharmaceutical care services and documentation of DTPs. The collected data were reviewed and supervised regularly for the completeness and cleanness of the data abstraction and DTP registration formats.
Statistical analysis
The collected data were entered into a computer using Epi Info 7 software and analyzed using the Statistical Package for Social Science version 20. A test of association between the independent variables and the presence of DTPs was done using binary and multiple logistic regressions. To declare a significant association, a probability value (p value) of 0.05 was used. Results were reported as crude odds ratio and adjusted odds ratio (AOR) with a 95% confidence interval (95% CI) to measure the strength of the association between predictor and outcome variables.
Results
Sociodemographic and clinical characteristics of the study participants
Out of 128 admitted and enrolled study participants, male and female respondents account for 61 (47.7%) and 67 (52.3%), respectively (Table 1). More than two-thirds of the patients were in the age group of 18–39 years. The majority of the study participants 86 (67.2%) were from rural areas; 101 (78.9%) were married, and more than one-third of the study participants were illiterate. Of the total study participants, 64 (50.0%) were orthodox and 57 (44.5%) were protestant. The monthly income of the majority of the study participants was between 500 and 2500 Ethiopian Birr.
Sociodemographic characteristics of the study participants admitted to the medical ward of WCUNEMMCSH from June to August 2021 (N = 128).

ETB: Ethiopian Birr; WCUNEMMCSH: Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital.
The major reasons for hospital admission were pneumonia 79 (61.7%), tuberculosis 20 (15.6%), urinary tract infection 16 (12.5%), and bacterial meningitis 13 (10.2%) (Table 2). Among the study participants, 45 (35.2%) of them had no history of recent antimicrobial drug use (within the previous 2 months), 42 (32.8%) had a history of recent use of antimicrobial drugs, and the remaining 41 (32.0%) could not differentiate the antimicrobial drugs they used. In total, 83 (64.8%) of the study participants were found to have two or more comorbidities. Only 12 (9.4%) of the study participants were without comorbid conditions. During hospitalization, about 61 (47.7%) of the study participants used fewer than 5 drugs for treatment, whereas 67 (52.3%) of the study participants used more than 5 different medications at the same time. More than three-fourths of the study participants stayed in the hospital for more than 7 days. From 288 antimicrobial drugs containing orders, the most frequently prescribed were ceftriaxone 120 (41.7%), azithromycin 69 (24.0%), and ciprofloxacin 32 (11.1%).
Clinical characteristics of the study participants admitted to the medical ward of WCUNEMMCSH from June to August 2021 (N = 128).
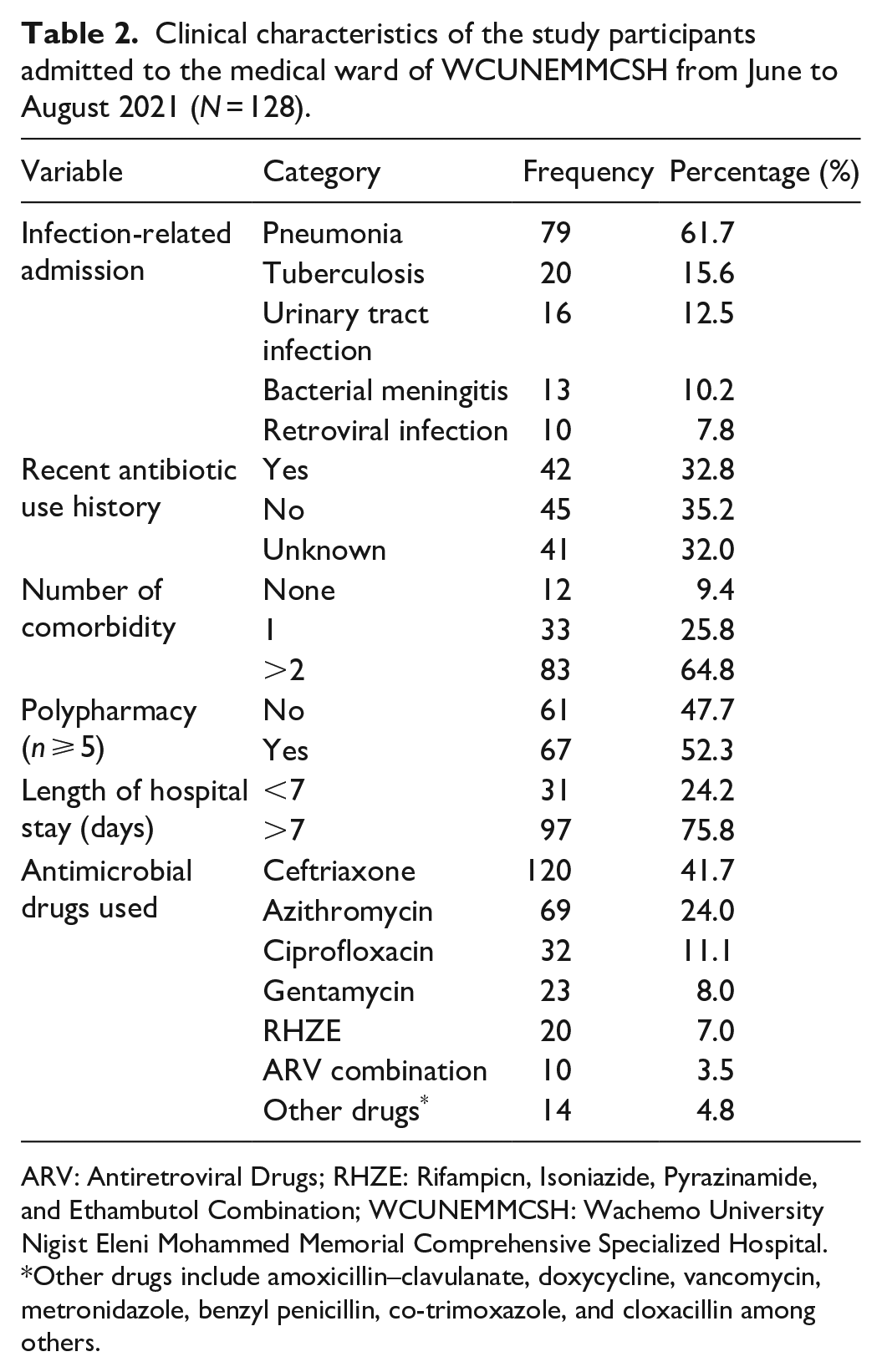
ARV: Antiretroviral Drugs; RHZE: Rifampicn, Isoniazide, Pyrazinamide, and Ethambutol Combination; WCUNEMMCSH: Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital.
Other drugs include amoxicillin–clavulanate, doxycycline, vancomycin, metronidazole, benzyl penicillin, co-trimoxazole, and cloxacillin among others.
Prevalence and characterization of DTPs
In all, 98 (76.6%) of the study participants experienced at least one type of antimicrobial DTP (Table 3). The most common DTPs were unnecessary drug treatment in 42 (32.8%), the need for additional drug treatment in 36 (28.1%), non-adherence in 30 (23.4%) of the patients, ADRs in 26 (20.6%), dosage too low in 15 (11.7%), dosage too high in 9 (7%), and ineffective drug therapy in 7 (5.5%). Of the study participants, 42 (32.8%) had one type of DTP, about 46 (35.9%) had two forms of DTP, and 10 (7.8%) had three forms of DTP.
The types of antimicrobial-use related DTPs identified in the study participants admitted to the medical ward of WCUNEMMCSH from June to August 2021 (N = 128).

ADRs: Adverse Drug Reactions; DTPs: Drug Therapy Problems; WCUNEMMCSH: Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital.
Predictors of antimicrobial use-related DTPs
The sociodemographic and clinical characteristics were analyzed to determine whether they could predict the occurrence of antimicrobial use-related DTPs or not. In this study, the binary logistic regression showed that there is no significant association between the occurrence of antimicrobial use-related DTP and sociodemographic variables including age, sex, marital status, area of residence, educational level, and occupation.
The length of hospital stay and the number of diagnosed diseases per study participant were found to be significantly associated with antimicrobial use-related DTPs using binary and multivariate logistic regression (Table 4). The study participants who had a length of hospital stay of more than 7 days were about three times more likely to have at least one form of DTP than those who had a length of hospital stay of seven days or less (AOR = 2.97, 95% CI = 1.06–8.32, p = 0.04). The study participants who had more than two diagnosed diseases were identified to be about three times more likely to have antimicrobial use-related DTPs than those who had one type of diagnosed disease in the multivariate logistic regression (AOR = 3.10, 95% CI = 1.12–8.15, p = 0.02).
Predictor variables of antimicrobial use-related DTPs among the study participants admitted to the medical ward of WCUNEMMCSH from June to August 2021 (N = 128).

AOR: Adjusted Odds Ratio; CI: Confidence Interval; COR: Crude Odds Ratio; DTPs: Drug Therapy Problems; ETB: Ethiopian Birr; WCUNEMMCSH, Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital.
Discussion
Antimicrobial use-related DTPs are among the major challenges for the healthcare system. 2 Failure of treatment, hospital re-admissions, emergency department visits, increased medical care costs, and increased risk of mortality are some of the effects of DTPs. 17 Identification of DTPs will help design preventive strategies, and provide responsible care and educational intervention to improve patient’s adherence to drug therapy.2,3,9 To our knowledge, this is the first study to determine antimicrobial use-related DTPs and factors associated with DTPs among patients admitted to the medical ward of WCUNEMMCSH, southwest Ethiopia. In this study, more than two-thirds of the study participants had at least one type of antimicrobial use-related DTPs. Unnecessary drug treatment and the need for additional drug treatment were the most common antimicrobial use-related DTPs. The contributing factors were multiple diseases diagnosed and the prolonged length of hospital stays.
The prevalence of at least one antimicrobial use-related DTP in this study (76.6%) is comparable with the studies done at the medical wards of Jimma University Specialized Hospital (75.7%), 20 Dessie Referral Hospital (75.5%), 15 Wollega University Referral Hospital (71.5%), 21 and Dilla University Referral Hospital (70.7%) 22 that revealed at least one antimicrobial use-related DTP. This might be due to the existence of health facilities at a similar level. However, the prevalence of DTPs associated with antimicrobial use was higher in our study than in previous studies conducted in Brazil (33.6%), 11 Switzerland (37.0%), 23 and Turkey (46.6%). 13 This difference might be explained by the level of patient care, particularly from access to effective antimicrobial drug prescribing practice guidelines or protocols for antimicrobial use, which would be explained by high access variability to those key process indicators for optimal and rational antimicrobial use practice. The prevalence of antimicrobial use-related DTPs in this study was also higher than that of the studies done in Ataye Hospital (38.7%), 24 Tikur Anbessa Specialized Hospital (52.0%), 25 and University of Gondar Teaching Hospital (66.0%). 16 This might be due to differences in the study population, design, or period.
Of the antimicrobial drugs ordered in our study, ceftriaxone (41.7%) was the most commonly used, followed by azithromycin (24.0%). These drugs are among the first-line or second-line drugs for infectious diseases such as bacterial meningitis, pneumonia, and sepsis that were prevalent in the study setting. Furthermore, these drugs were more frequently prescribed than other drugs in the study setting. In addition, ceftriaxone (25.8%) was also the most frequent specific drug prone to DTPs in the study done in Dessie Referral Hospital, 15 whereas penicillin (40.0%) and ceftriaxone (19.3%) were the most frequently prescribed antimicrobial drugs in the medical ward of Arba Minch Hospital, southern Ethiopia. 26 This difference in our case may be due to patients’ being exposed to the other antimicrobial drugs at different referral levels.
Unnecessary drug therapy (32.8%) was the most frequently identified antimicrobial use-related DTP in our study, which is comparable with the studies conducted at Dessie Referral Hospital (30.2%), 15 Jimma University Specialized Hospital (28.9%), 20 and the Mizan, Bonga, and Tepi Hospitals of southwest Ethiopia (28.9%), 27 but higher than reported at Wollega University Referral Hospital (21.1%). 21 The contributing factors to this higher rate of unnecessary drug therapy may be the absence of a valid medical indication at that time, the use of broad-spectrum antibiotics, using antimicrobial drugs for a long period of time, and multiple drug products (duplication of therapy) being used for a condition that requires single drug therapy.
The next frequently seen antimicrobial use-related DTP in our study was the need for additional drug therapy (28.1%), which is comparable to the studies done in Jimma University Specialized Hospital (29.6%), 20 and Mizan, Bonga, and Tepi Hospitals of southwest Ethiopia (31.3%). 27 However, the need for additional drug therapy in our study was higher than that of studies conducted at Dilla University Referral Hospital (13.5%) 22 and Wollega University Referral Hospital (22.8%). 21 This may be due to failure to give preventive drug therapy to reduce the risk of developing a new condition and additional drug therapy to attain synergistic or additive effects. Failure to provide additional drug therapy may contribute to poor clinical outcomes or the development of preventable complications, both of which may lengthen hospital stays and incur additional costs for patients and the healthcare system as a whole.
The third frequently seen antimicrobial use-related DTP in our study was non-adherence of the patients to their medication (23.4%), which is comparable to the studies in Mizan, Bonga, and Tepi hospitals (21.7%), 27 but higher than that of the studies conducted in Jimma University Specialized Hospital (17.1%) 20 and Dessie referral hospital (5.7%). 15 The reason for this higher non-adherence rate in our study may be the low-income level of the study participants, which is mainly related to unaffordability in covering both health expenditure and purchasing drugs. In addition, the use of multiple drugs at the same time, which might lead to difficulty differentiating their medications, contributes to non-adherence. The non-adherence of the patients to their medication reported in our study, however, was lower than that reported in the studies conducted at Dilla University Referral Hospital (29.7%) 22 and University of Gondar Teaching Hospital (28.9%). 16 The difference might be due to the difference in the availability of the drugs and study duration, as it was conducted for a shorter period of time in our study.
The other frequently seen antimicrobial use-related DTP in our study was ADR (20.6%), which is comparable with that of a study done at Tikur Anbessa Specialized Hospital (23.0%) 25 but higher than that of studies conducted at Dessie referral hospital (9.4%), 15 at Jimma University Specialized Hospital (8.6%), 20 and at Mizan, Bonga, and Tepi hospitals (7.6%). 27 This higher rate of ADRs in our study may be due to an inappropriate combination of antimicrobials with other drugs. The difference in the prevalence of ADRs among the studies could also be due to under-or over-reporting of ADRs that may contribute to under-or over-estimation.
Another antimicrobial use-related DTP in our study was an inappropriate dosage of 18.7% (dosage: too low 11.7% and too high 7.0%). The occurrence of a dosage too low in our study might be due to an inappropriately shorter duration of antimicrobial drug therapy and the use of low dose in cases where it is needed optimally. Low-dose antimicrobial drug use may contribute to the development of drug resistance. The occurrence of a dosage too high in our study may be due to the use of drugs for a long period of time. In addition, a drug interaction is a possible contributing factors. High doses of antimicrobial drug use could result in dose-dependent toxicities of the drugs. The prevalence of inappropriate dosage in our study, however, was lower than that of the studies in Mizan, Bonga, and Tepi hospitals 38.2% (dosage: too low 22.4% and too high 15.8%), 27 in the University of Gondar Teaching Hospital 39.1% (dosage: too low 20.7% and too high 18.4%), 16 and in Jimma University Specialized Hospital 44.0% (dosage: too low 28.9% and too high 15.1%). 20 This difference might be due to differences in the study population, setting, study design, and time period. The close supervision by health professionals might also have contributed to the low prevalence of inappropriate dosage among the admitted patients in our study.
Prevalence of ineffective drug use (5.5%) was the least observed antimicrobial drug use-related DTP in our study and was lower than that of the studies conducted in Jimma University Specialized Hospital (9.2%), 20 University of Gondar Teaching Hospital (18.4%), 16 and Wollega University Referral Hospital (20.4%). 21 The ineffective drug use in our study may be due to the frequent use of broad-spectrum antimicrobial drugs for a long period of time due to a lack of well-established diagnostic setup and culture-based diagnosis. This overuse of broad-spectrum antimicrobial drugs might contribute to the development of antimicrobial drug resistance and needs coordinated intervention.
In this study, the sociodemographic and clinical characteristics of patients were analyzed to determine whether these variables could predict the occurrence of antimicrobial use-related DTPs or not. The binary logistic regression showed that there is no significant association between the occurrence of antimicrobial use-related DTP and sociodemographic variables including age, sex, marital status, area of residence, educational level, and occupation. This finding is consistent with studies done in the University of Gondar Teaching Hospital (66.0%), 16 Wollega University Referral Hospital (71.5%), 21 Tikur Anbessa Specialized Hospital (52.0%), 25 and the studies in Mizan, Bonga, and Tepi hospitals (28.9%). 27
The two variables that were identified as predictors of the prevalence of antimicrobial use-related DTPs in our study were the number of diagnosed diseases and the length of hospital stays. These findings were consistent with reports of studies conducted at the University of Gondar Teaching Hospital 16 and Wollega University Referral Hospital 21 that reported comorbidity and length of hospital stays as determinants of antimicrobial use-related DTPs. Compared to study participants who were diagnosed with one disease, those who had more than two diseases diagnosed displayed a significantly higher rate of inappropriate use of antimicrobial drugs. As the number of disease conditions increases, the number of drugs taken will usually increase. This may result in drug–drug interactions, medication errors, non-adherence, and ADRs. Length of hospital stay was also another determinant of inappropriate use of antimicrobial drugs, that is, prolonged hospital stay was the risk factor for the occurrence of DTPs. The more the patient stayed in the hospital, the more likely the patient had a chance to acquire new infections such as hospital-acquired infections. These infectious diseases require additional and more complex medications, which further contribute to the occurrence of DTPs such as poor adherence.
There are some limitations to this study. First, the shorter time used for the study limited the total sample size involved in the study, although we included all patients admitted to the medical ward during the study period that fulfilled the inclusion criteria and gave written consent to participate. Second, the study did not attempt to classify DTPs based on their severity levels, that is, mild, moderate, and severe. Third, the study did not determine the outcomes of DTPs. Hence, further research is warranted. However, the method we followed and the study design we employed increased the strength of our study and may give us the confidence to draw conclusions from our findings.
Conclusions
Our findings showed that there was a high prevalence of antimicrobial use-related DTPs among patients admitted to the medical ward of WCUNEMMCSH during the study period. The number of diagnosed diseases and the length of hospital stay were determinants of the presence of antimicrobial use-related DTPs. Interdisciplinary health professionals should work together to reduce the high prevalence of DTPs among medical ward-admitted patients in WCUNEMMCSH. An expert-oriented, well-developed best practice guideline to monitor the consistency of antimicrobial drug prescriptions and use should be established. A valid guideline, if effectively disseminated and implemented, may have the potential to optimize drug therapy and improve treatment outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221140228 – Supplemental material for Antimicrobial use-related drug therapy problems and associated factors among patients in the medical ward of Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, Southwest Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221140228 for Antimicrobial use-related drug therapy problems and associated factors among patients in the medical ward of Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, Southwest Ethiopia by Arega Adere, Amin Edao, Melaku Tesfaye and Zelalem Petros in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are grateful to WCUNEMMCSH management, administrative staff, and the healthcare professionals in the medical ward for their permission and continuous support in conducting this study. Our appreciation also goes to the graduating pharmacy students who collected the data.
Author contributions
AA, AE, and ZP conceived and designed the study. AA and AE collected the data. AA, AE, and ZP analyzed the data. AA, AE, MT, and ZP wrote this article. All the authors revised and edited the article and approved the final revision for submission.
Availability of supporting data
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Department of Pharmacy, College of Medicine and Health Sciences, Wachemo University (Ref. No. Phar 142/2013 E.C). A support letter was sent to the hospital, and permission was obtained from WCUNEMMCSH officials to conduct the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects and the legally authorized representatives of illiterate subjects before the study.
Written informed consent to participate
The benefits and harms of the study were explained to the patients participating in the study, and written informed consent was obtained from all subjects and the legally authorized representatives of illiterate subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.