
Abstract
Objective:
This study aimed to assess uncontrolled blood pressure and contributing factors among patients with hypertension.
Methods:
Hospital-based cross-sectional study was conducted from January to April 2021 at Bedele General Hospital. Data were collected using the semi-structured questionnaire. All patients with hypertension were included using consecutive sampling technique unless ineligible. EpiData 4.4.2 was used for data entry, and SPSS 24.0 was employed for analysis. Binary logistic regression analysis was performed to identify factors associated with uncontrolled blood pressure.
Results:
A total of 219 patients with hypertension were included in the study. About 60.3% of participants were male. The mean age of the study participants was 48.54 ± 12.93 years. The prevalence of uncontrolled blood pressure among the study participants was 56.2%. The factors significantly associated with uncontrolled blood pressure were age >60 years (adjusted prevalence ratio = 4.42; 95% confidence interval = (1.71, 11.46); p = 0.002) and the presence of comorbidity (adjusted prevalence ratio = 2.16; 95% confidence interval = (1.22, 3.82); p = 0.008).
Conclusion:
More than half of the study participants had uncontrolled blood pressure. Older age and comorbidity were the predictors of uncontrolled blood pressure. Attaining controlled blood pressure is important to avoid consequences of high blood pressure. So, healthcare provider should focus on achieving target blood pressure goal.
Introduction
Hypertension (HTN) is the main contributor to the global mortality of disease and burden. 1 It has been considered as a disease of developed countries but has been changed radically in the previous decades being now higher in Africa than developed countries. 2 Most low- and middle-income countries are currently confronting a significant public health challenge due to a continued high burden of non-communicable diseases, especially HTN. 1
About 1.39 billion adults population have HTN throughout the world, and the rate is expected to increase as a result of different factors including urbanization, especially in low- and middle-income countries. 3 The HTN prevalence has ever been increasing at an alarming rate among low-income countries, particularly the African. 4 In Ethiopia, a systematic review showed that the prevalence of HTN is 9.3%–30.3% in population-based studies, 7%–37% in institution-based studies, and 13.2%–18.8% in hospital-based studies. 5
HTN is one of the most common cardiovascular disorders leading to cardiovascular diseases–related morbidity and mortality in both developing and developed countries. 6 It is discovered as a main risk factor for health loss and mortality, and accounts for 13% of mortality and 6% of disability throughout the world. 7 It is responsible for at least 45% of deaths due to heart disease and 51% of deaths due to stroke. 5 Poorly controlled HTN also leads to various abnormalities like ventricular remodeling, complex ventricular arrhythmia, re-polarization abnormalities, and autonomic dysfunction. 8
Even though, a multiple effective antihypertensive medications with confirmed benefits in reducing cardiovascular morbidity and mortality are available, blood pressure of patients with HTN remains uncontrolled. In both developed and developing countries, less than 27% and 10%, respectively, of patients with HTN have achieved their goal of blood pressure control. 9 In Ethiopia, the prevalence of uncontrolled blood pressure is significant among patients with HTN. The meta-analysis reported that uncontrolled blood pressure is 48% in the country. 10
There are different contributing factors to uncontrolled blood pressure among patients with HTN. The studies showed that older age associated with uncontrolled HTN.11–13 Another study reported that female gender, younger age, baseline blood pressure, and frequent changes in regimen were associated with poor blood pressure control. 14 Poor medication adherence, lack of information about HTN, and side effects could be considered as possible underlying causes of uncontrolled blood pressure. 15
Blood pressure control is a main challenge in many developing countries including Ethiopia. 4 Factors contributing to uncontrolled blood pressure are inconsistent across the studies in Ethiopia. In addition, there was no study done at Bedele General Hospital among patients with HTN to assess their blood pressure status. Thus, this study aimed to determine the level of uncontrolled blood pressure and contributing factors among patients with HTN.
Methods
Study setting and population
The study was conducted from January to April 2021 at the outpatient care of Bedele General Hospital. The hospital is located in Oromia region, Southwest Ethiopia at 483 km from Addis Ababa, the capital city of Ethiopia. It provides health services for about 57,700 outpatient attendants per year. There are about 230 adult patients with HTN on follow-up at the hospital.
All adult patients with HTN who visited the hospital during data collection period and fulfilled the inclusion criteria were the study population. The inclusion criteria were age 18 years or above, and patients who have started taking antihypertensive medications. Patients who were critically ill or not interested to participate were excluded from the study.
Study design and sampling
A hospital-based cross-sectional study design was used to conduct the study. All adult patients with HTN who attended follow-up at outpatient department of Bedele General Hospital during data collection period and fulfilled the inclusion criteria were included in the study. Small number of patients with HTN was attending the hospital for ambulatory care. Therefore, the sample size was not calculated, and all patients with HTN were included in the study based on fulfillment of the inclusion criteria using consecutive sampling technique. The total number of patients with HTN on follow-up at the hospital was 230. Of 230 patients with HTN on follow-up at the hospital, 219 included in the study and 11 patients were excluded based on the eligibility criteria.
Study variables
The dependent variable was uncontrolled HTN. Independent variables were socio-demographic variables (age, sex, marital status, religion, educational status, occupation, residence, and body mass index (BMI)), clinical characteristics of patients (family history of HTN, presence of comorbidity, duration of the HTN, and antihypertensive medications), and behavioral practices (alcohol consumption, chewing chat, smoking status, and medication adherence).
Data collection
A semi-structured questionnaire was developed for collecting data after reviewing relevant prior studies4,16–21 and using the World Health Organization (WHO) STEPwise approach to surveillance of non-communicable diseases, a previously validated tool. 22 Face-to-face interview was employed to collect data from patients, and Afan Oromo was used to interview the patients using the translated questionnaire to the language. To maintain validity of the data collection tool, it was back translated to English by independent person. Patients’ medical records were reviewed to retrieve relevant data and antihypertensive medications. The data collection was conducted by two pharmacists and one nurse.
The data collectors were trained by the principal investigators before starting data collection. The pretest was done on 5% of patients with HTN attending follow-up at Chora Hospital to check applicability, consistency, and understandability of the questionnaire. An ambiguous and misinterpret questions were edited before starting collecting data. All collected data were evaluated for correctness, consistency, integrity, and clearness by the principal investigator on a daily basis.
Blood pressure measurement
Patient was ordered in a seated position and after a 5-min rest period, blood pressure was measured using a mercury sphygmomanometer by a senior nurse. The three of blood pressure readings were taken to evaluate blood pressure control of the study participants. The baseline blood pressure measurement was taken on the first day that the patient visited the hospital during the data collection period. Then, the first blood pressure measurement was obtained at the first month of initial visit. The second and third blood pressure measurements were made at second and third months following the initial visit during the data collection period, respectively, and the average of these three readings was used to classify patient’s blood pressure as controlled or uncontrolled.
Anthropometric measurements
The patient’s weight was measured on an adult weighing scale to the nearest 0.5 kg, and the height was measured using a standard height board. The BMI was calculated as weight in kilograms divided by height in meters squared. BMI was classified as normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), or obese (⩾30.0 kg/m2).
Statistical analysis
The EpiData Manager 4.4.2 was used for data entry, and Statistical Package for Social Science (SPSS) 24.0 was employed for analysis. Frequency, percentage, and mean value were used for descriptive statistics. The association between patients’ characteristics and uncontrolled HTN was examined by the binary logistic regression model. The p-value < 0.05 was used for statistical significance.
Operational definitions
Controlled blood pressure: it is less than 150/90 mm Hg blood pressure measurement in patients with HTN aged 60 years or older, or blood pressure less than 140/90 mm Hg in aged less than 60 years and all ages of patients with HTN and diabetes mellitus (DM) or chronic kidney disease (CKD). 6
Uncontrolled blood pressure: it is 150/90 mm Hg or above blood pressure reading in patients with HTN aged 60 years or older, or 140/90 mm Hg or above blood pressure reading in patients with HTN aged less than 60 years and all ages of patients with HTN and DM or CKD. 6
Medication adherence: patients who took all the prescribed medications by accepting, agreeing, and correctly following a prescribed treatment during the last 7 days were considered to be medication adherent. 21
Physically active: patients who were doing physical activity or participated in a specific exercise session for at least 30 min per day for 5 days or more per week. 16
Cigarette smokers: the participants who smoke at least one cigarette per day at the time of the study were considered as smokers. 17
Alcohol consumers: male who drink more than two units of alcohol/day and female patients who drink more than one unit of alcohol/day were considered as alcohol consumers. 18
Salt intake: salt intake was defined as WHO recommendation. Accordingly, salt reduction is consumption of below 5 g per day or equivalent to one teaspoon full. 20
Comorbidity: any chronic disease that coexisted with an index disease. 16
Results
Socio-demographic characteristics of the study participants
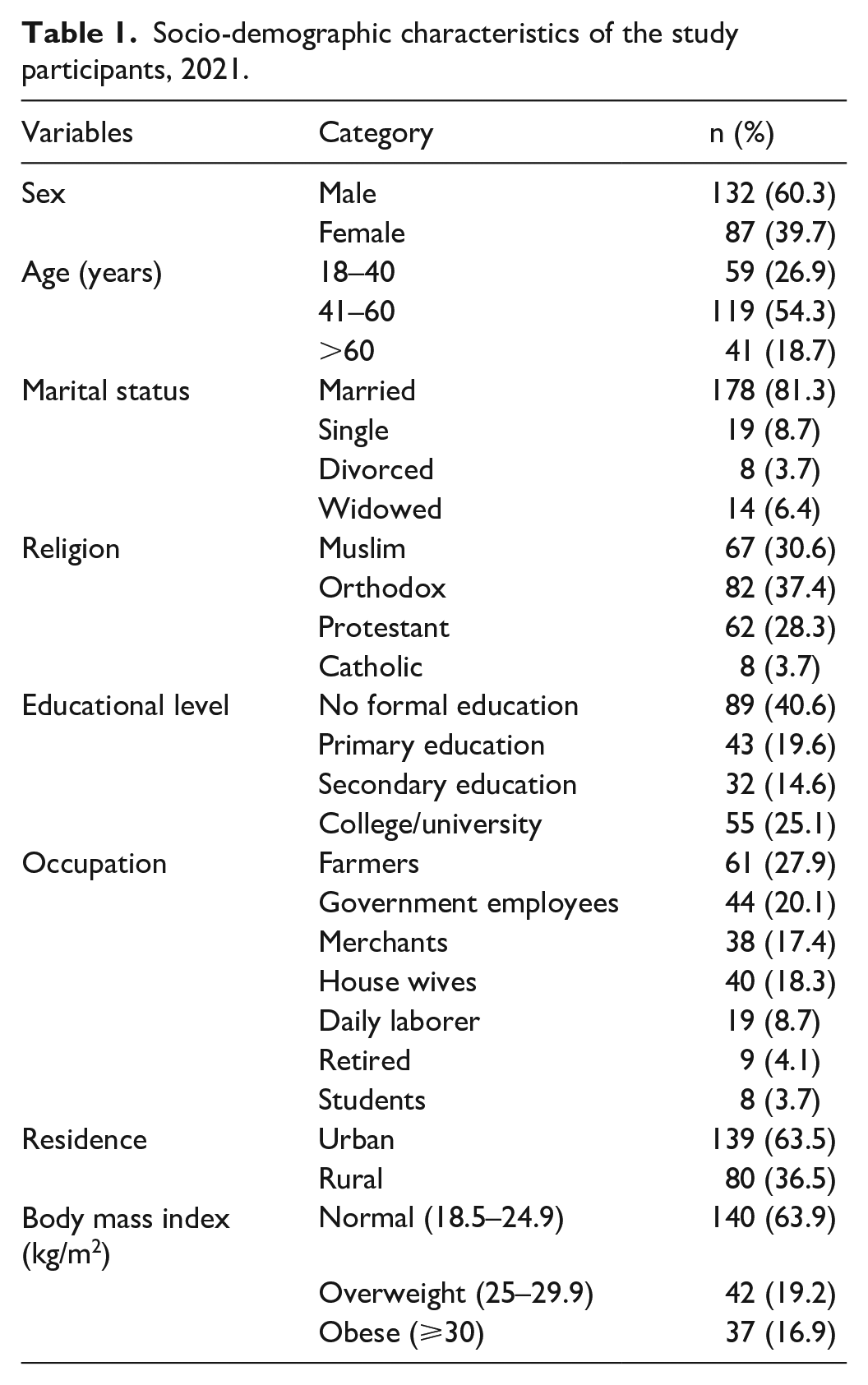
This study included a total of 219 study participants of whom male participants were 60.3%. The mean age of the study participants was 48.54 ± 12.93 years and more than half (54.3%) had age from 41 to 60 years. The majority of the participants were married which counted for 81.3%. In terms of religion, orthodox followers counted the highest number (37.4%). The educational status showed that about 40.6% of participants had never attained formal education. About 27.9% of participants were farmers in terms of their occupational status. Almost two-third of the study participants were urban residents (Table 1).
Socio-demographic characteristics of the study participants, 2021.
Clinical and behavioral characteristics of the study participants
Blood pressure status of the study participants showed that 56.2% had uncontrolled blood pressure. Family history of HTN was identified in 37.0% of the study participants. More than (52.5%) of the study participants had at least one comorbid disease. About 73.1% of the study participants had duration of diabetes 5 or less than 5 years (Table 2).
Clinical and behavioral characteristics of the study participants, 2021.

Antihypertensive drugs usage
Thiazide diuretics were the most frequently prescribed antihypertensive which counted for 35.2%. The other commonly prescribed antihypertensive agents were calcium channel blockers (30.8%) and angiotensin-converting enzyme (ACE) inhibitors (26.9%). About 60.7% of the study participants were using two or more antihypertensive drugs (Table 3).
Antihypertensive medications usage among the study participants, 2021.
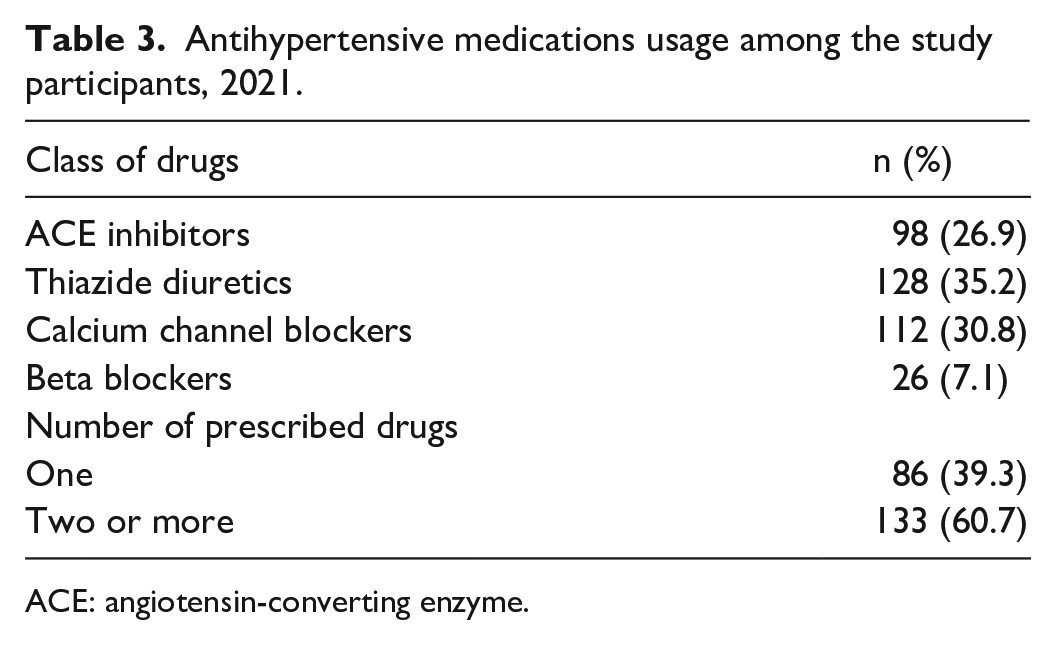
ACE: angiotensin-converting enzyme.
Factors associated with uncontrolled blood pressure
The association between uncontrolled blood pressure and different characteristics of the study participants was determined. A chi square and bivariable analysis showed that there is association between blood pressure status and factors such as sex, age, educational status, place of residence, family history of HTN, comorbidity, and duration of HTN. A significant association was identified between uncontrolled blood pressure and age and the presence of comorbidity in multivariable logistic regression. Participants with older age >60 years were 4.4 times more likely to have uncontrolled blood pressure when compared to younger age (adjusted prevalence ratio (APR) = 4.42; 95% confidence interval (CI) = (1.71, 11.46); p = 0.002). The likelihood of uncontrolled blood pressure was 2.2 times more among participants with comorbidities (APR = 2.16; 95% CI = (1.22, 3.82); p = 0.008) (Tables 4 and 5).
Variables in relation to uncontrolled blood pressure in the study participants, 2021.

BP: blood pressure.
Binary logistic regression analysis for factors associated with uncontrolled blood pressure among the study participants, 2021.

CPR: crude prevalence ratio; CI: confidence interval; APR: adjusted prevalence ratio.
Discussion
Despite treatment, study has shown the high prevalence of uncontrolled blood pressure among patients with HTN. 7 Difficult-to-control blood pressure represents a burden in real life. 23 Effective control of patients’ blood pressure leads to desired therapeutic outcomes like preventing HTN-related complications and mortality which ultimately decreases the global burden of the disease. 14 Controlling HTN often requires the use of several antihypertensive agents, especially in elderly patients or those with stroke or diabetes. 24
This study identified that 56.2% of the study participants had uncontrolled blood pressure. This is consistent with previous studies conducted in Ethiopia which reported 52.7% in Jimma, 19 52.5% in Tigray, 20 56.7% in Bale, 21 57.1% in Debre Tabor, 4 and 55.8% in Dessie city. 25 It is also similar with the finding of the study done in New York which revealed that uncontrolled blood pressure was 51%. 26 However, our finding is higher than a result of study done in Gonder which observed uncontrolled blood pressure in 37% of study participants. 27 The present finding is also higher than the results of study conducted in Thailand and Spain which reported 24.6% and 44.6% of uncontrolled blood pressure, respectively.24,28 The difference in the study population, study design, and sample size might be contributing factors for the discrepancy of the findings.
This study showed that uncontrolled blood pressure is significantly associated with age of the study participants. It is observed that uncontrolled blood pressure is higher with older age, greater than 60 years. This result is consistent with a study conducted by Asgedom et al. 29 which reported that age greater than or equal to 65 years is significantly associated with uncontrolled blood pressure. A study done by Tesfaye et al. 19 also identified old age as a predictor of uncontrolled HTN. Similarly, other studies have shown that elderly patients with HTN have a higher chance of uncontrolled blood pressure.11,13,30 It has been well established that the incidence of chronic disease rises sharply with age and that the majority of patients with a chronic disease are over the age of 65 years. 31 Older people experience greater morbidity with a corresponding increase in medication utilization and are at an increased risk of non-adherence to their medication. 32 Finally, it results in sub-optimal outcome of the treatment. In contradictory to our finding, some studies reported that patients with HTN with older age are at lower risk for uncontrolled blood pressure.27,28,33 This discrepancy might be due to the difference in the sample size and population background.
The presence of comorbidity was identified as a predictor of uncontrolled blood pressure in this study. Our finding is similar with a study conducted by Gebremichae et al. 20 which reported that the presence of comorbidity is independent predictor of uncontrolled blood pressure. The studies showed that patients with HTN who are comorbid with diabetes mellitus are at higher risk of having uncontrolled blood pressure.15,27 A study conducted by Teshome et al. 4 also observed that having asthma comorbidity among patients with HTN is significantly associated with sub-optimal blood pressure control. Patients with HTN who have comorbidities are more likely to require combination therapy, yet physicians are often reluctant to adjust the number and doses of medications to achieve target blood pressure. 34 The presence of additional diseases in patients with HTN may increase medical care costs and pill burden. These in turn may affect patients’ adherence to their medications.
This study observed that there was no significant association between medication adherence and uncontrolled blood pressure. This finding is inconsistent with a study conducted in Dessie, northeast Ethiopia, which reported that poor medication adherence is the determinant of uncontrolled blood pressure for patients with HTN. 25 Other different studies also showed that medication adherence is significantly associated with blood pressure control.15,16 The discrepancy between this study and the previous studies might be due to the difference in the tool used to assess medication adherence. In addition, the smaller sample size in this study might be contributed to the discrepancy.
Limitation of the study
The smaller sample size was one of the limitations of this study. The study was conducted in a relatively small sample size which may affect generalizability of the findings. There might be recall and social desirability bias since the behavioral characteristics of the participants were based on self-reports. Due to the small number of patients with HTN who were attending the follow-up at the hospital, the sample size calculation was not performed, which is another limitation of this study.
Conclusion
This study observed that there were a significant number of patients with HTN who had uncontrolled blood pressure. Older age and the presence of comorbidities were factors significantly associated uncontrolled blood pressure. Attaining controlled blood pressure is important to avoid consequences of uncontrolled blood pressure. So, healthcare provider should focus on achieving target blood pressure goal. Providing continued patients education for patients with HTN regarding the importance of controlling blood pressure is important in optimizing blood pressure.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221126333 – Supplemental material for Uncontrolled blood pressure and contributing factors among patients with hypertension at outpatient care of Bedele General Hospital, Southwest Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221126333 for Uncontrolled blood pressure and contributing factors among patients with hypertension at outpatient care of Bedele General Hospital, Southwest Ethiopia: A cross-sectional study by Tadesse Sheleme, Oda Jilo, Firomsa Bekele, Wayessa Olika, Birbirsa Safera and Yadeta Babu in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the study participants and data collectors for their cooperation.
Author contributions
T.S., O.J., F.B., W.O., B.S., and Y.B. contributed to the conception, design, data collection, and analysis. T.S., and O.J. participate in writing up the manuscript, and F.B., W.O., B.S., and Y.B. reviewed and edited the manuscript. All authors read and approved the final manuscript and agreed its submission for publication.
Availability of data and materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Mettu University (PHAR56/13).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.