
Abstract
Objectives:
Numerous studies have shown that links exist between exposure to acid suppression among adults and nutritional deficiencies, especially vitamin B12 and iron. While the use of acid suppression among children and infants is common, nutritional deficiency remains a concern but does not have numerous studies to support it. We conducted a cohort study to examine this concern; the hypothesis we proposed is that acid-suppressive therapy (AST) during infancy is linked to anemia in the first year of life.
Methods:
This retrospective cohort study included infants born between 2017 and 2018 who visited Legacy Community Health. The inclusion criteria were exposure to acid suppression for a minimum of 1 month and a hemoglobin reading at 12–15 months. Infants who had hemoglobinopathies, failure to thrive, or malabsorption syndromes were excluded. Mean hemoglobin was calculated, and student’s t-test was applied to find statistical differences between the two groups. Change in weight before and after treatment was recorded. Occurrence of respiratory and gastroenterological adverse events was recorded in the exposed group.
Results:
Overall, 135 exposed infants were identified 135 controls were selected. The majority of the sample included Hispanic girls. Ranitidine was the most commonly prescribed medicine. The duration of treatment was 3 months. Weight improved significantly at termination of the treatment. There was no significant difference between the hemoglobin level of cases and controls, and both were not considered anemic.
Conclusion:
AST was not linked to anemia, despite the slightly lower hemoglobin in some cases. There were few weaknesses in our study; therefore, further studies can examine this link by focusing further on medication type and close follow-up. We found that although proton pump inhibitors are considered the first line of treatment, histamine-2 receptor antagonists were more frequently prescribed. Strategies to familiarize general pediatricians with the NSAPGHAN guidelines might be needed.
Introduction
Many reports have raised concerns regarding the side effects of long-term use of proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs), collectively referred to as acid-suppressive therapy (AST). The most important adverse effects include decreased bone density, infection, and low vitamin B12 levels. In a review by Ito and Jensen, the duration of PPI use was linked to decreased non-heme iron absorption. 1 Moreover, it has been reported that the prolonged use of PPIs decreases iron absorption, which is beneficial in patients at risk of iron overload due to conditions such as hereditary hemochromatosis and congenital dyserythropoietic anemia.2,3
In a retrospective cohort study by Sarzynski et al., 4 using PPIs for 1 year was associated with iron deficiency anemia (IDA) in adult patients. In addition, Vinnakota and Brett 5 concluded that AST (including PPIs and H2RAs) was associated with IDA. In 2016, the New England Journal of Medicine reported a link between prolonged exposure to PPIs (here defined as 2 years) and IDA. 6
Few studies in children have investigated the adverse effects of long-term AST use. In a 10-year literature review, Cohen et al. 7 reported anemia as a side effect of lansoprazole and pantoprazole. Another report assessing the adverse effects of AST among infants outlined different complications, including bacterial overgrowth and increased risk of infections, such as Clostridioides difficile infection, gastroenteritis, and community-acquired pneumonia, these potential complications could arise from using omeprazole or ranitidine for 8 weeks. Infants with very low birth weights who were receiving H2RAs had higher rates of necrotizing enterocolitis. However, the report did not mention anemia as a potential complication. 8 In a commentary published in the Journal of Pediatrics, Hassall 9 discussed AST in infants. Numerous adverse effects were linked to using AST in children, such as acute gastroenteritis, community-acquired pneumonia, necrotizing enterocolitis, candidemia, and increased food allergies. While AST has been linked to adverse nutritional effects in adults (such as decreased iron and vitamin B12 absorption), whether this holds true for children is unknown, which limits the exposure of children to AST only when needed.9,10 In their pediatric gastroesophageal reflux clinical practice guidelines, the North American society for pediatric gastroenterology, hepatology and nutrition (NASPGHAN), based on case–control studies, outlined similar risks when using PPIs and H2RAs, while still recommending H2RAs when PPIs are not available. 11
In an assessment of knowledge and beliefs regarding gastroesophageal reflux disease (GERD) among 1245 participating pediatricians, 82% believed that GERD could be treated with AST without the need for diagnostic testing. Of these, 19% thought that H2RAs were more effective. In addition, many clinicians stated that they would prescribe H2RAs as the first-line treatment. 12
Sources of iron in infants vary. In addition to prenatally stored iron, milk (either breastmilk or formula) is one of the main sources of iron. Breastmilk is low in iron concentration but has a high bioavailability. Formula milk is enriched with ferrous sulfate. At 4–6 months of age, infants typically start eating solid foods. Elemental iron–enriched cereals are the main source of this nutrient until infants start consuming meat at approximately 8–9 months of age. Iron absorption occurs in the duodenum, where Fe3+ is reduced to Fe2+ by duodenal cytochrome B and then enters enterocytes through the divalent metal transport 1 (DMT1) transporter. Iron is stored as ferritin in enterocytes and as hemosiderin in the liver, spleen, and bone marrow. Ferroportin is the protein which transports iron from inside the cell to the interstitium, the iron is then transported to areas of need via transferrin. Hepcidin is a regulatory protein secreted by the liver; an increased secretion of hepicidin downregulates iron absorption. It has been noted that hepcidin concentration decreases throughout infancy to prevent iron deficiency. 13 In contrast, low gastric pH increases iron solubility, which in turn facilitates iron absorption. 14 It was recently postulated that PPIs inhibit iron absorption via hepcidin upregulation and duodenal ferroportin inhibition. 15
Many adult studies have examined the relationship between anemia and AST; however, few pediatric studies have investigated this relationship. This study aimed to determine the association between exposure to AST during infancy and anemia at 1 year.
At Legacy Community Health, we screen children for IDA by evaluating the hemoglobin concentration at 12 months of age, in accordance with the American Academy of Pediatrics recommendations and in agreement with the statement by the Centers for Disease Control and Prevention. 16 HemoCue Hb 201+ is a device used in our organization as a point-of-care hemoglobin analyzer for the accurate quantitative determination of hemoglobin in children up to 5 years of age. Training fieldworkers and staff is important to ensure the correct operation of the instrument, including maintaining quality control.17,18
Methods
This retrospective cohort study was conducted at Legacy Community Health, a primary-care health organization in southeast Texas. The institutional review board of the Sam Houston State University approved this study. The data were analyzed anonymously; therefore, the requirement for consent was waived. The electronic medical record (EMR) system used was Athena Health (AthenaPractice V20) (Visualutions, Inc., Spring, TX, USA). The sample was identified through a manual search of the EMR and included patients born between January of 2017 and December of 2018. The cases of interest were infants who were exposed to at least one type of acid-suppressive agent (PPI or H2RA) for a minimum of 1 month and who had a hemoglobin reading at the age of 12–15 months. The medications included ranitidine, famotidine, omeprazole, lansoprazole, and pantoprazole. Age at treatment initiation, treatment duration, pre- and post-treatment weight-for-age percentiles adjusted for gestational age, hemoglobin readings at 12–15 months of age, and occurrence of respiratory or gastroenterological illnesses during treatment were documented. The second group of infants was the randomly selected controls born between 2017 and 2018, whose hemoglobin levels were also measured and recorded at 12–15 months of age, and who were not exposed to AST, and exclusion criteria did not apply to them. Other data, such as ethnicity and sex, were also recorded. The hemoglobin level was assessed by trained clinic medical assistants using the HemoCue Hb 201+ system (HemoCue, Angelholm, Sweden). Patients with hemoglobinopathies, malabsorption syndromes resulting in failure to thrive, or GI bleeding were excluded.
Statistical analysis
Based on a two-group comparison of hemoglobin levels in children reported by Yewale and Dewan, 19 an a priori power analysis determined that a total sample size of 52 would be sufficient to detect a statistically significant difference between two groups at the .05 level with 80% power using a two-tailed independent samples t-test. Although Yewale and Dewan found a large effect (d > .8), they decided that a more conservative estimate of effect size should be used. An additional power analysis estimating a medium effect size (d = .5) determined that a total sample size of 128 would be sufficient to detect a statistically significant difference at the .05 level with 80% power using a two-tailed independent samples t-test. A power analysis was conducted using G*Power version 3.1.9.2.
After collection, the data were analyzed using IBM SPSS version 26 (SPSS, Inc., Chicago, IL, USA). Anemia was defined as a capillary hemoglobin level < 11 mg/dL. Respiratory adverse events constituted the diagnosis of upper respiratory illness or pneumonia during the course of treatment. Adverse gastroenterological effects included diarrhea or vomiting during the course of the treatment.
The EMR search retrieved a total of 150 charts for infants who had received at least 1 month of AST before their first birthday during the 2 years from January of 2017 to December of 2018. Fifteen patients did not have a record of hemoglobin measured at 12–15 months of age and were excluded from the study, leaving a final AST sample of 135 infants. We identified infants born between 2017 and 2018 who were not exposed to AST and whose hemoglobin was measured at 12–15 months of age; 135 infants were selected. Half were born in 2017 and the other half in 2018.
Results
Demographics
The ethnicity of the sample was mostly Hispanic (51.9%), followed by African-American (28.9%); 54.8% were female and 45.2% were male (Table 1). The ethnicity of the sample reflects the demographics of our patient population, as it includes mostly Hispanic and African-American people.
Ethnicity and sex of the AST and control samples.

Choice of pharmacotherapy
Table 2 shows the breakdown of the types of medicines used for AST and the side effects documented during treatment. Over 90% of infants received ranitidine as an acid suppressant. The most common side effects of the treatment were respiratory issues (36.3%), while a small minority (5.2%) experienced gastrointestinal issues.
AST medication and side effects.

AST: acid-suppressive therapy.
Duration of treatment
As shown in Table 3, all infants included in the exposed study group began their AST therapy before 11 months of age, and the therapy was terminated before their first birthday. The average age at medication initiation was 3 months; however, in some cases, treatment was started as early as 1 month. The average duration of medication was 3.22 ± 3.2 months. The average age at the first follow-up after medication termination was 7 months, with some patients seen as late as 11 months, shortly before the first birthday.
Age at initiation and termination; duration of medication therapy.

SD: standard deviation.
Hemoglobin variable
The research question proposed in this study was addressed in two ways. First, hemoglobin levels measured at 12–15 months were compared among patients exposed to AST therapy before 12 months and among infants who were unexposed. The results of the independent sample t-test are presented in Table 4. There was no significant difference in hemoglobin levels between infants who had been exposed to AST therapy and those who were unexposed (t (268) = 0.76, p = 0.447). Nonetheless, the absolute value of the average hemoglobin in the exposed group was slightly lower than that in the unexposed group.
Comparison of hemoglobin in infants exposed vs unexposed to AST therapy in the first year.

AST: acid-suppressive therapy; SD: standard deviation.
A second analysis was conducted to determine whether the overall incidence of anemia (defined as ctHb g/dL < 11.0) was greater in those exposed to AST therapy in the first year than in those not exposed. Table 5 shows the results of a chi-square test of independence, indicating that the 12.6% incidence of anemia in the exposed infants was not significantly greater than the 11.1% incidence in the unexposed infants (χ2(1) = 0.142, p = 0.706).
Anemia incidence in infants exposed vs unexposed to AST therapy in the first year.
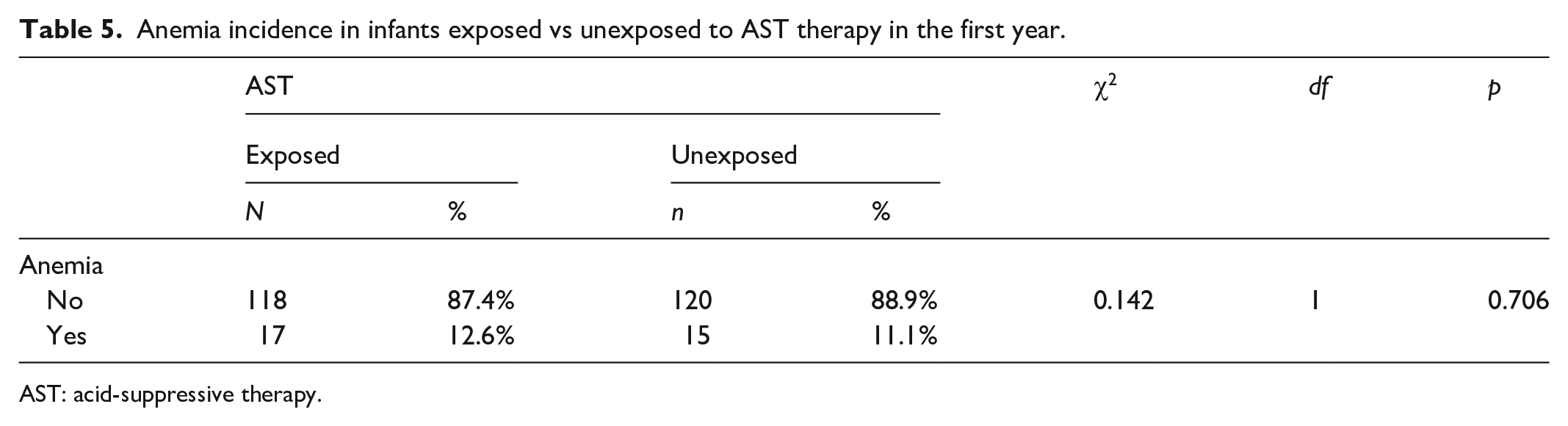
AST: acid-suppressive therapy.
Weight analysis
A final analysis was conducted to determine whether exposure to AST affected weight gain. A paired t-test was used to compare the weight percentiles measured at the initiation of AST with those measured at the first follow-up appointment after termination of the therapy. Table 6 presents the results. The average weight percentiles increased significantly (t (134) = 2.17, p = 0.032). Although the post-treatment weight-for-age percentile increased, it might be difficult to attribute this to a direct response to therapy rather than the natural progression of weight gain among infants.
Change in weight percentile from initiation to first post-therapy follow-up in infants exposed to AST therapy in the first year.

SD: standard deviation.
Discussion
Our study is an attempt to further elaborate on the effects of gastric acid suppression among infants and the development of anemia at the age of 1 year. We found that both groups had normal hemoglobin levels. While the exposed infants had slightly lower hemoglobin levels than the non-exposed group (11.85 mg/dL and 11.94 g/dL, respectively), this difference was not statistically significant. The normal hemoglobin level at 12 months did not reflect the hemoglobin value immediately after termination of therapy.
The most commonly prescribed acid-reducing medication was ranitidine, started at an average of 3 months of age and as early as 1 month of age. Acid-reducing medications were prescribed for an average of 36 months. The average age at which infants placed on AST had their first follow-up after termination was 7 months. The weight-for-age percentiles were significantly higher after treatment than before treatment in the exposed group. Among the infants included in the case group, males were prescribed AST more than females were.
Finally, during the course of treatment, 36.3% of the infants who received AST were diagnosed with a respiratory illness, while 5.2% were diagnosed with a gastrointestinal illness. Of those who developed respiratory or gastrointestinal illness, the majority was on ranitidine and a minority was on lansoprazole.
As discussed earlier, many concerns raised in the pediatric population stem from the adult data. Few studies have examined the association between anemia and acid suppression among infants. In adults, the development of iron deficiency or vitamin B12 deficiency is associated with long-term usage, typically 1 or 2 years of treatment, resulting in the recommendation to monitor patients for anemia if treatment is prolonged. The side effects that pertained to the pediatric population were mostly respiratory and gastroenterological. A 10-year literature review reported a higher rate of adverse events with AST than in our study. For instance, the use of ranitidine was associated with 74% of patients developing gastroenteritis and 19% developing pneumonia. In our study, we reported 36.3% respiratory and 3.2% gastroenterological adverse events. 7 In the context of acid reflux disease, weight gain can be a natural progression of the condition or a direct response to medication.
Diaz et al. 12 reported that, in the context of gastroesophageal reflux, 30% of pediatricians started their patients on AST. In the context of GERD, 82% of pediatricians started their patients on AST, with 33% starting PPI, and 74% starting H2RAs. This is consistent with the practice of our providers, which differs from the NASPGHAN recommendations that doctors should refrain from the use of acid suppression in cases of reflux and that PPIs remain the first-line of pharmacotherapy in cases of GERD. The duration of treatment might be within the recommendations, despite the fact that many patients receive treatment for a longer duration than recommended. 9
Limitations
Our study was limited by several factors. While the sample size was adequate to identify a statistical difference, the sample was selected from a period of 2 years. Including infants over a wider time range may be more representative. Infants in the unexposed group were randomly selected, and the mean value of hemoglobin in that group might not be precise. Moreover, most patients were exposed to ranitidine, which was recently withdrawn from the market. 20 Given the small sample size of infants who received PPIs, it was difficult to compare hemoglobin levels based on the type of AST exposure. Given the nature of the study, it was difficult to control for dietary iron and conduct an analysis of hemoglobin and other red blood cell indices before and after treatment. Therefore, effect of dietary iron intake compared to use of acid-suppressive therapy was difficult to assess. In this study, hemoglobin was obtained months after termination of treatment, which might not reflect the true value of hemoglobin immediately after termination. The hemoglobin levels were slightly lower in the exposed group, which may be a concern. Adverse events, such as respiratory or gastroenterological symptoms, were the mere occurrence of those symptoms rather than an attempt to find a link or causal effect. The two groups were not compared in specific range of time, making it difficult to obtain variables such as weight gain and adverse events in order to conduct a meaningful comparison. These are important considerations for a prospective follow-up study that should be conducted in the future. It was difficult to obtain similar symptoms in the control group and a comparison was not conducted.
Conclusion
AST appears to have limited effects on hemoglobin levels in children by the age of 12 months. While found to be slightly lower in the exposed group, hemoglobin continued to be within the normal range, and weight gain was observed before and after treatment, which could be a reflection of therapy effectiveness. Primary-care pediatricians in our organization were found to use H2RA as the first choice of acid suppression; however, PPI is considered more effective according to the NASPGHAN guidelines. A controlled prospective study is recommended to better investigate the effects of AST, particularly PPIs, on hemoglobin and other red blood cell indices before and after treatment, as well as adverse events.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Sam State Houston University Institutional Review Board. STUDY #: IRB-2020-349.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for the present study because the research involves no more than minimal risk to subjects; the research could not be carried out practicably without the waiver or alteration; the waiver or alteration will not adversely affect the rights and welfare of the subjects; and patient information was de-identified.