
Abstract
Objectives:
To present findings of a workshop with physical activity professionals in Manitoba, Canada, to facilitate the enhancement of physical activity promotion efforts by exploring (1) effective physical activity strategies, (2) methods to strengthen physical activity strategies, (3) challenges in implementing physical activity strategies in Manitoba, and (4) strategies to support collaboration.
Methods:
The Manitoba Research Chair in Primary Prevention hosted a workshop for 54 stakeholders in Manitoba. Qualitative and quantitative data obtained from the workshop were analyzed using qualitative content analysis and univariate descriptive analysis. Purposive sampling was used to recruit participants with diverse experiences in physical activity promotion.
Results:
Strategies were identified and presented according to the socioecological model. Community assessment and community engagement, regional partnerships, capacity building, and mitigation of barriers characterized the discussion. In addition, discussions emphasized the need for the consistent and comprehensive application of a provincial physical activity action plan. The workshop ended with a discussion of the importance of collaboration to improve physical activity programs and initiatives.
Conclusion:
Several common needs were identified that reflect topics from the broader literature. Collaborations and insights from workshop participants provide direction to target increased physical activity support and programming across disciplines, sectors, and regions.
Keywords
Introduction
Physical activity (PA) is bodily movement produced by skeletal muscles that require energy expenditure. 1 Despite the evidence in favor of increasing PA, many adults persistently fail to obtain the recommended 150 min a week of moderate intense PA.2,3 Physical inactivity, defined as less than 150 min of PA a week, is the third leading global risk for mortality in the world.4,5 Regular PA is associated with weight maintenance and reduced risk of developing some chronic diseases.6–10 Individuals who are physically active have a 14% lower risk of mortality from coronary heart disease relative to sedentary individuals. 4 PA has also been shown to (1) prevent bone loss; (2) reduce the number of falls and fractures; (3) improve body composition, coronary blood flow, and cardiac function; and (4) enhance psychological well-being.7,9,10
Despite the scientific evidence showing the health benefits associated with PA, low levels of PA are pervasive. Worldwide, 31% of adults are considered inactive. 11 Rates of inactivity are even higher in North America, where 45% of Canadians and 63% of the US population are not meeting the PA recommendation.4,12 Equally alarming, in 2013 global health care costs related to physical inactivity were estimated at US$53.8 billion, which does not account for additional costs associated with reduced productivity and functional ability. 13 In 2009, physical inactivity in Canada was associated with CanS2.4 billion in health care costs and CanS4.3 billion in indirect costs, including measurable reductions in productivity. 14
Over half (57%) of the 1.3 million people living in Manitoba, Canada, reside in Winnipeg 15 and almost one-third (28%) of the population lives in rural and remote communities. 16 First Nation, Metis, and Inuit populations represent 17% of the Manitoba population. 17 Manitoba is doing poorly compared to other Canadian provinces on a number of health indicators. For example, mortality from diabetes and premature mortality rates in Manitoba are higher than the national average. 18 Primary prevention, such as PA, may help improve these outcomes.4–10 However, rates of PA in Manitoba have stayed relatively consistent. In 2013, 43% of Manitobans were inactive during their leisure time. 12 There have been a number of public-sector-based efforts to increase PA in the Manitoba population: targeted policy, government-supported promotion, and formation of PA action plans and provincial coalitions of PA providers. 19 PA initiatives including In Motion, 20 Healthy Together Now, 21 and Active Canada 20/20 22 are national in scope. These initiatives suggest that programs and strategies should be tailored to the context of implementation. There is limited evidence to guide the development and improvement of low-cost and effective-at-scale PA interventions. 8
In May 2016, the Primary Prevention Research Team, comprised of both male and female researchers, hosted a full-day workshop for individuals working in the PA sector in Manitoba, Canada. The overall goal of this forum was to bring together a diverse group of PA stakeholders from across sectors, disciplines, and health regions in Manitoba. The workshop provided an opportunity to share strategies and experiences in PA promotion to assess (1) effective PA strategies, (2) methods to strengthen PA strategies, (3) challenges in implementing PA strategies in Manitoba, and (4) strategies to support collaboration. The workshop identified factors that affect PA promotion currently and in the future.
Methods
This qualitative descriptive study identifies and summarizes the activities, challenges, and needs of a diverse stakeholder group involved in PA promotion. Purposive sampling was used to recruit participants who could represent communities across Manitoba and within various kinds of settings (e.g. school, community) and within various roles (e.g. policy, community engagement). The Physical Activity Coalition of Manitoba (PACM), a group of PA stakeholder organizations, assisted with recruitment of workshop participants. Recruitment strategies included flyers and emailed invitations, as well as personal communications from MG and PACM.
The 54 workshop attendees comprised representatives from across the province. Seven participants who had registered for the workshop did not attend. Perspectives and experiences were presented by stakeholders from non-profit organizations (recreation, sport; 27.8%), regional health authorities responsible for the delivery of health care services (25.9%), academic institutions (25.9%), provincial and federal levels of government (13.0%), regional school divisions (1.9%), and other stakeholder groups (5.5%). The majority of attendees were female (81.5%). There were frontline (20.4%), managerial (18.5%), coordinator (16.7%), consultation (11.1%), and policy/health (5.6%) specialists as well as research oriented professionals (22.2%) and students (5.5%). Ethical approval for the workshop was obtained from the University of Manitoba Health Research Ethics Board.
Data collection
An environmental scan of PA initiatives and programs operating in Manitoba preceded the workshop. The findings provided the focus for facilitated discussion of strengths, challenges, and opportunities for action around PA initiatives and strategies in Manitoba. The facilitator’s guide was developed for the workshop with guidance from Health in Common, an organization offering planning and evaluation support services. The facilitator’s guide was structured around the following questions: (1) what is working in the promotion of PA, (2) what could strengthen what is working, (3) what are the challenges to PA strategy implementation in Manitoba, and (4) strategies to support cross-regional and interdisciplinary collaboration. The facilitator’s guide was not piloted prior to the workshop. Prior to the workshop, facilitators (PW, MH, MG, GH, JR, AK) attended a training session to review the agenda, the facilitator’s role, and note-taking expectations. At the beginning of the 1-day workshop, informed consent was obtained from all participants.
Data analysis
Quantitative data (workplace, organization information) were entered and analyzed using predictive analytics software (PASW) Statistics 18 software to describe the workshop attendees. Facilitator notes from workshop flip charts and participants’ worksheets (questions of interest) were organized by question type and entered into NVivo 10 analysis software for content analysis. The data collected from each of the inquiry topics were coded by three researchers (MG, LK, PW). The codes were then grouped into categories that characterized the factors that were important to the participants. To enhance dependability of the analysis, three researchers (MG, LK, PW) were involved in coding and met to discuss discrepancies until consensus was reached. The findings were presented to the facilitators who validated the categories according to their interactions with participants. The workshop facilitators reviewed the final groupings to assess accuracy and appropriateness of the reported categories.
We used a socioecological theoretical framework to report the workshop findings.23,24 According to Sandelowski, 25 a theoretical framework to report results provides a vehicle to present qualitative descriptions enabling researchers to resist simple classification of the results. The social-ecological model is a comprehensive approach to examine the person-context interrelationships within five socially organized subsystems that influence PA participation: the individual, interpersonal, organizational, community, and public policy environments. The model helps identify opportunities and potential targets to promote PA by recognizing interrelated factors that influence one’s ability to be sufficiently active.23–25 The socioecological model supported the choice of categories in the content analysis. Emergent categories from the analysis enabled a more nuanced description of factors as well as interrelationships within, and between, systems. A summative report of workshop findings was prepared and sent to workshop participants. Researchers have maintained contact with some participants to inform researchers of PAs.
Results
The data analysis resulted in a number of categories, which the researchers then organized within the socioecological model. This model provides a constructive framework for presenting the emergent categories and the relational subtleties that became evident.23–25 We identified one category at the individual level, three categories within the interpersonal environment, three categories in the organizational environment, five categories related to the community, and five categories discussing public policy (Figure 1). Previous literature has demonstrated the importance of each socioecological system when developing and implementing a PA program.23,24

Workshop participant feedback within the socioecological framework.
What is working in the promotion of PA?
PA professionals emphasized the need to consider individual-level circumstances and interpersonal relationship in the development and implementation of PA programs. PA programs considered successful by workshop participants were built on identified needs of individuals within the community to address community-specific barriers. For example, the In Motion program was a provincial strategy to encourage PA and healthy eating with specific community programs led by, and tailored to, individual circumstances. Community groups applied for In Motion grants to implement age-specific community tailored programs such as dance classes for seniors, family fun nights, and pedometer-walking groups, all of which were initiatives tailored to needs identified by individuals in the community. Workshop participants felt the successful programs result from engaging individuals and discussing their PA needs (Table 1).
Identified actions from the PA workshop.

PA: physical activity; MPAAP: Manitoba Physical Activity Action Plan.
The table outlines the actions discussed by the 54 PA workshop participants following review of the environmental scan of PA initiatives and programs operating in Manitoba. Actions are presented in each of the areas of the socioecological framework.
At an organizational level, workshop participants discussed long-term partnership commitments that generate better outcomes for PA program participants by increasing continuity of staff and programs, and engagement with PA participants. At the community level, effective PA programs are “integrated into existing programs” that consider community context. Integration of PA professionals into community programs produce multi-sector partnerships that led to improved PA programs more appropriately tailored to the community. PA program integration requires support at a societal level. Workshop participants discussed effective relationships and partnerships such as the PACM and their contribution to the Manitoba Physical Activity Action Plan (MPAAP). The “MPAAP creates [a] similar vision [for PA], guidelines [for PA programs], and enhances PA promotion initiatives.” The action plan “identified [the] need to focus on broad context and built environments …” (Table 1).
What could strengthen what is working in PA promotion?
At an individual level, workshop participants identified specific areas that should be addressed to increase PA participation, including barriers of PA participants (e.g. childcare, transportation), knowledge about PA programs and the importance of PA for health and well-being, availability of PA professionals and programs, and barriers in program administration. “[We] need to listen to participants we are trying to support … delivering programs based on participants’ needs.” Workshop participants reported programs responsive to local needs and barriers are more successful in reaching diverse populations. Within the interpersonal environment, this requires collaborating with community groups and priority populations (e.g. Indigenous populations) to address context-specific barriers to participation, including cultural appropriateness, safety, transportation, and accessibility. Workshop participants recognized PA program development and expansion should be complemented with the implementation of equity-based programming (Table 1).
Within the organizational environment, workshop participants perceived multi-sectoral PA initiatives as cost-effective collaborations, “supporting each other in work [both physically and mentally] and [increasing eligibility for] resource obtainment.” Shared resources between programs described by workshop participants included facilities, people, funding, programming, and time. Multi-sector collaboration can “increase funding source [eligibility] by diversifying and becoming more attractive to funders” (Table 2). Collaboration among key stakeholders can create supportive networks, build capacity, and generate a larger resource base. “Shared resources [can help to] address gaps and challenges in funding and resources,” as well as improve reach, flexibility, and sustainability of PA programs (Table 2).
How can collaboration improve PA interventions and strategies.
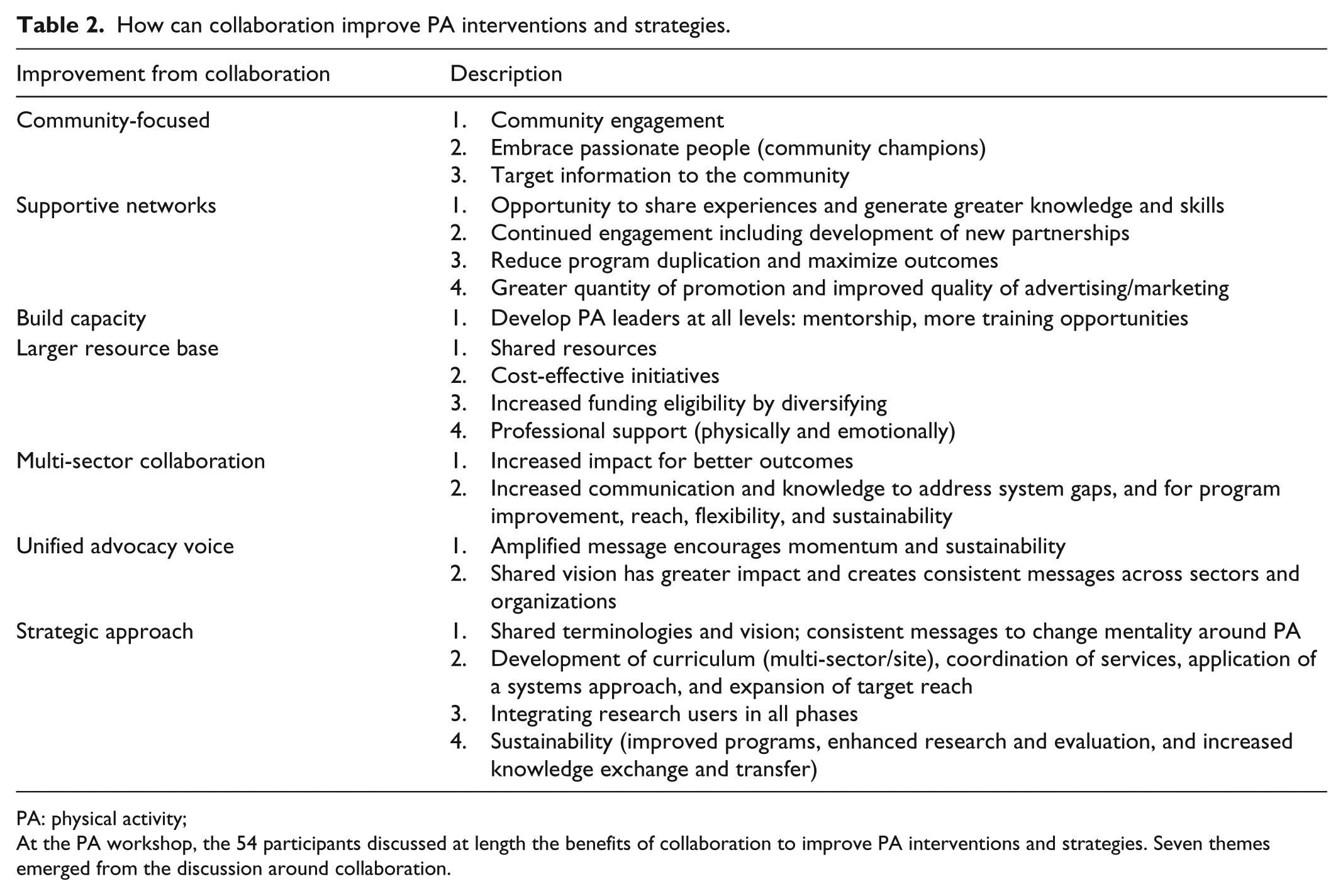
PA: physical activity;
At the PA workshop, the 54 participants discussed at length the benefits of collaboration to improve PA interventions and strategies. Seven themes emerged from the discussion around collaboration.
Building on strengths discussed in the individual, interpersonal, and organizational levels, workshop participants explained increased community outreach, coupled with “integration into community healthcare services, workplaces and early year’s centers” (e.g. schools, daycares), would increase community members’ PA (Table 1). There is a need to “foster local, regional, and provincial inter-sectoral relationships, networks and partnerships” and “improve communication of goals” (Table 1). “Working together creates shared terminology [and] shared vision,” “enables the development of curriculum …,” “enhances coordination of services, and applies a systems approach” (Table 2). “Stronger policies,” explained workshop participants, should “focus on the broader context to address influences of [the] social and built environment on PA.”
At a societal level, participants indicated developing a “unified advocacy voice” would “amplify our message” and create a “collective voice for change [to] allow [for] momentum and sustainability.” “[We can create] shared vision [and terminology, that] has a greater impact [and encourages system level change with] consistent messaging across sectors and organizations” (Table 2). Workshop participants felt improved coordination of PA services can lead to a system-wide approach to improve sustainability of the PA system and produce better outcomes for participants. “System-level change” can be ascertained with the creation of a “unified voice,” increased knowledge of the benefits of PA, and increased awareness of PA leaders and best practices.
Current knowledge translation (KT) activities within the PA sector focus on equipment and training of PA professionals and presentations at local conferences. Although current KT activities (e.g. training on exercise equipment) are beneficial for PA professionals, workshop participants sought expansion to include different modes and avenues for KT, and greater quantity and improved quality of PA research. Workshop participants explained they require additional PA research and evaluation complemented with “more formal opportunities for knowledge exchange that engage [PA] leaders, policy-makers, [researchers] and funders.” “There is a lack of [PA] data at a local level [for research]” combined with “limited connectivity” to share available information (Table 1). Workshop participants suggested the “creation of an information hub [can] support knowledge development and exchange of research and practice-based successes [derived from context specific data and experience]” (Table 1). “[We] need to build the case for greater investment [in PA].”
What are the challenges to implementing PA strategies?
Workshop participants noted challenges to implementation of discussed strategies. Within the individual system, workshop participants explained that individuals from particular subpopulations in Manitoba are less likely to meet the PA recommendation, including Indigenous populations, new immigrant populations, new mothers, Hutterites, and those living in small rural and remote communities. Needs assessments can assist PA program development by highlighting the needs and wants of individuals within the community (Table 1). “Project goals with the incorporation of a participant lens and communication with stakeholders [will enhance PA program development and expansion].”
Within the interpersonal environment, cultural awareness training for PA professionals and the incorporation of a “welcoming environment” into PA programs is critical to increasing PA participation. Culture appropriate environments will encourage community members to feel comfortable discussing PA needs with program representatives. Many workshop participants identified a need, within the organizational environment, for additional professional development training, and more research and evaluation (Table 1). Collaboration can provide training opportunities as well as practical and financial support. “[We need to] learn new skills … through increased training opportunities [that become available with partnerships].” Collaboration creates joint knowledge and understanding of the system, motivation for continued engagement, and more expertise through combined perspectives and experience with past successes and failures. “More perspectives [create a] more complete understanding [of the system], by learning from each other’s experiences and preventing duplication or recreating the wheel” (Table 2).
At a community level, PA professionals at the workshop felt individuals outside of the PA sector frequently misunderstood their qualifications. Cross-sectoral and jurisdictional collaboration within PA is challenged by infrastructural and communication complexities (e.g. understanding of PA vocabulary). Funding needs to be directed toward the built environment to improve infrastructure for active living (Table 1). Increased knowledge of PA initiatives and PA professionals’ expertise among community members and potential partners can enhance PA initiatives (Table 2).
Challenges at a society level are associated with the political climate (Table 1). Workshop participants explained that the MPAAP created an opportunity to consider new ideas and think creatively. However, in practice, there is a “lack of a common vision and unified voice” within the PA sector. Workshop participants explained, currently the PA sector in Manitoba is “characterized by fragmented service delivery, inconsistent policies across organizations, a lack of political knowledge … and support, and ideological differences on how to move forward.” To strengthen PA programming, there is a need to establish a “holistic and comprehensive approach to PA” by “eliminating [the] red tape surrounding program delivery and making prevention a priority at the government [level].” Workshop participants advocated for increased government support and financial resources to strengthen PA initiatives and programming (Table 1). “Increased funding and improved funding models” are required to develop and maintain PA initiatives. In Manitoba, many workshop participants spoke of the “general lack of support for PA [programs] or policy, and no support from administration” (Table 1). PA is not consistently viewed as an essential service to improve population health, explained workshop participants. “We need provincial consistency.” PA needs to be seen as a priority within preventive health services before there will be motivation to increase PA in all jurisdictions.
Discussion
This workshop highlighted the importance of the individual, interpersonal, organizational, community, and public policy in the development of feasible and actionable PA strategies. Here, we discuss the potential actions and next steps that might be helpful.
The individual: need assessment
Our study participants identified need assessment and participant feedback as avenues to support and tailor PA initiatives to the needs of the priority population(s). Research has found some segments of the population are less able to obtain sufficient amounts of PA due to the limited reach of PA interventions and reduced public benefit from inappropriately designed programs.3,9,26 Need assessments promote inclusion, provide detailed information on community members’ experiences, and empower the participant by providing an opportunity to build relationships and create necessary changes. Overall need assessments help build successful programs responsive to local needs and barriers. 27 In Manitoba, there have been more than CanS515,000 awarded to 204 Manitoba communities through In Motion grants. However, the In Motion program funding is no longer available to support community initiatives. 20 Funding availability is a major obstacle preventing needs assessments and the establishment of individualized and community-based programming. Physical Activity Plan Toolkits and Community Assessment Tools are available to provide direction on involving the community in program planning; these resources should be evaluated and shared among stakeholders.27,28
The interpersonal environment: community engagement
Our findings are consistent with literature that shows sufficient PA participation is associated with positive social norms and greater social interaction within a community.9,23,24 Healthy Together Now was a Manitoba initiative that provided funding and support to 1200 community-based activities that encouraged healthy lifestyles. For example, the Duck Bay Fit for Fun Family Day was a community-led program to promote the benefits of PA. Healthy Together Now 21 emphasized the importance of fostering and developing community champions who can lead community activities. However, similar to In Motion, there have been funding reductions preventing the continuation of Healthy Together Now program funding. Limited short-term resources for programming prevent long-term health benefits from sustainable PA initiatives. Collaborative approach to PA including a variety of stakeholders can overcome resource limitations and produce sustainable programs.
The present study suggested an equity approach be used to develop and implement PA programs. The Winnipeg in Motion’s 29 report, “Equitable Access: Why It Matters,” explains how, and why, equity is important for increased access to healthy food and PA among all income levels and types of communities. Evidence shows cultural awareness training combined with priority population engagement will lead to the development of more successful PA programs and services.29,30 The large First Nation and Metis populations in Manitoba, particularly in northern and remote Manitoba communities, have unique community and cultural characteristics that should influence the implementation of a PA program. 17 Similar to our study, Macniven et al. 9 discuss the impact of culture and community factors on obtaining sufficient levels of PA participation within Indigenous populations. Community engagement and context-specific programs can aid in overcoming the barriers to PA including a lack of infrastructure and social supports conducive to PA participation.9,30,31 Furthermore, meaningful inclusion of local representatives in program planning, implementation, and evaluation can foster a sense of community ownership; indeed, our findings suggest “nothing about us without us” initially described within the context of Indigenous research may be a helpful guiding principle for building sustainable PA programs. 31
Organizational-level interactions: integrated programming
Our study documented some examples of how collaboration between PA professionals and other sectors can enhance PA strategies. Fostering relationships, partnerships, and networks with community members and a variety of service providers, researchers, government departments, and funders will develop the infrastructure to support more efficient, effective, and evidence-informed PA programs. PA programs built by networks inclusive of health, education, social services, and employment personnel can comprehensively attend to individual and community needs within the program. 32 Long-term PA partnerships lead to improved programming and higher rates of PA participation among community members attributable, in part, to increased flexibility and sustainability of programs and staff, increased resource acquisition, and increased training opportunities. A Manitoba, website, housed by PACM, provides resources, networking opportunities, training and education/research in the area of PA, which can assist in establishing partnerships for PA strategies. 33
Community-level interactions: the broader environment
Community outreach, coupled with integration into community services, can influence individuals’ PA participation by attending to their skills, beliefs, and context.9,34,35 Despite evidence for the integration of PA professionals and health care providers,8,9,35-37 workshop participants reported integration barriers due to limited knowledge among community members and health professionals about PA professionals and their qualifications. Winnipeg in Motion 38 has created a webpage to inform health care providers how they can influence and promote PA. Integration of PA professionals and health providers can increase the amount of individualized advice provided to patients for increasing PA.8,36,37
The built environment, including the amount of green space, destinations within walking distance, and walkability of the community, has been shown to impact the level of PA participation.9,23,24,30,38,39 Workshop participants emphasized the need for funding support to address barriers within the built environment. For example, the limited number of biking and walking paths in some areas of Winnipeg is a deterrent for PA. As referenced by Active Canada 20/20, 22 “government departments responsible to community planning, design and transportation should establish and implement policies to prioritize active transportation” (p. 17). Physical and social infrastructures within communities need modernization to make PA an inviting, practical, and accessible option.
Public policy: national guidance and financial commitment
Throughout the workshop, it was clear that the current MPAAP was not being implemented as intended. 19 Effective implementation of the MPAAP requires a consistent approach, a common vision, and a unified voice. Public policy must recognize the importance of community assessment, community engagement, community integration, and collaboration. Combined knowledge can create a comprehensive approach to address the broader constraints and barriers experienced during implementation of PA strategies. Prior to the workshop, PA funding from governments and non-government organizations had been increasing. However, at the time of the workshop, two key programs, In Motion and Healthy Together Now, had received funding cuts. Workshop participants felt continued advocacy from coalitions and PA professionals, as well as additional research noting benefits of PA, will increase support for PA initiatives.
Similar to this study, Horodyska et al. 32 highlighted the importance of long-term partnerships, implementation consistency, integration of existing resources, and multi-level, multi-component interventions when developing and implementing PA programs. As proposed by workshop participants, multi-sectoral PA initiatives can create cost-effective collaborations to address the individual, social, and physical environments that impact PA. Such interventions have the greatest potential to be effective and sustainable, and are therefore appealing to practitioners and funding bodies. 32
Finally, participants identified the importance of research and evaluation, as well as improved avenues for knowledge exchange. Highlighting PA successes including documenting impactful interventions and providing evidence to show that PA meaningfully affects health outcomes can provide direction to future program expansion and contribute to sustainability in the PA sector. New research and knowledge exchange avenues must be more sensitive to the range of domains for PA, variations in participation, and consider a broad range of outcomes. 40
Limitations
Workshop participants had expertise in PA and expressed an interest in participating in the workshop. Findings from this workshop represent experiences from a sample of PA stakeholders from Manitoba, Canada, before extrapolating to an international context consideration should be given to societal differences. Workshop discussions were not audio recorded, and thus verbatim transcripts from attendees were not available. Rather, facilitators took notes during the discussions and attendees were asked to provide individual written responses to questions of interest. These notes and written responses were transcribed for content analysis. 41 Results suggest categories for future actions that can be verified through further research.
Conclusion
To increase PA, strategies should be aimed at the individual’s immediate environment and extend into their indirect environment with consideration for public policy, culture, and social ideologies that underpin PA participation at a societal level. A holistic and comprehensive approach to PA characterized by collaboration, community assessments and engagement, and mitigation of barriers to PA participation can increase PA. Participatory approaches to program development, research, and evaluation were desired by workshop participants, with a focus on adapting knowledge and best practices to the context of implementation. Additional PA research and program evaluations will not only enhance current PA initiatives and programs but build sustainability within the PA sector. KT within, and outside of, the PA sector can create PA advocates who can generate political influence to aid in enhancement of PA programs and build sustainability in the PA sector.
Footnotes
Acknowledgements
We thank all workshop attendees and Health in Common Executive Director, Cathy Steven, for contributing to the workshop development and facilitation, and collection of the data for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Health Research Ethics Board at the University of Manitoba (H2016:149 (HS19650)).
Funding
This research was funded by a primary prevention research chair awarded to Alan Katz sponsored by Heart and Stroke Foundation and Research Manitoba.
Informed consent
Written informed consent was obtained from all subjects before the study at the workshop.