
Abstract
Background:
Tissue plasminogen activator within 4.5 h of onset is effective for acute ischemic stroke. However, only small proportion of patients is treated due to delayed presentation. We aimed to examine the factors associated with delays of stroke patients in Riyadh, Saudi Arabia.
Methods:
A cross-sectional survey was conducted at King Abdulaziz Medical City, Riyadh, Saudi Arabia, during a 6-month period. An interviewer administered structured questionnaire addressed to the acute stroke patients or their relatives was used to explore the factors associated with delayed arrival.
Results:
A total of 227 patients attending the emergency department were interviewed. The mean age was 60.4 ± 15.6 years. Approximately 56.4% presented after 4.5 h of stroke onset. Factors associated with late arrival were being alone during the onset of stroke, not being transported in an ambulance, not knowing that they were experiencing a stroke, and residing outside the city of Riyadh.
Conclusion:
More than half of patients missed the golden hours for thrombolysis due to delayed presentation. Reasons include lack of knowledge, underuse of ambulance and difficult access to care. Urgent community-based interventions are needed to address these factors.
Introduction
Stroke is a common neurological emergency which carries significant morbidity and mortality. The incidence of stroke is currently increasing among the populations of low- and middle-income countries.1,2 Stroke is a major health burden as it is a leading cause of physical disability in adults and the second most frequent cause of mortality after heart disease. 3 Apart from the serious imSSSpact that it has on one’s health, stroke also imposes tremendous costs on a nation’s society and economy. The expense associated with post-stroke rehabilitation and care is significant and the increasing number of disabled stroke patients can adversely affect productivity of a country. 4
Despite the proven efficacy of intravenous tissue plasminogen activator (IV tPA) within the first 4.5 h after the onset of symptoms, 5 only a small proportion of stroke victims receive this medication. The lack of administration of IV tPA is mainly due to the delayed presentation of patients to the emergency department (ED).6–11 Factors contributing to this delay are many and are influenced by awareness of stroke signs and symptoms, perception of the importance of early presentation for treatment, religious and cultural beliefs, educational level, geographical accessibility and technical factors such as the availability of diagnostic facilities and therapies.12–16 Data on acute stroke patients’ health-seeking behaviors in Saudi Arabia are lacking. The aim of this study is to examine how stroke patients in a stroke center located in Saudi Arabia reacted to the stroke symptoms, how fast they arrived at the ED and the factors that contributed to their late arrival.
Methods
Patient population
The patients in this study were ischemic and hemorrhagic stroke patients arriving at the ED at King Abdulaziz Medical City (KAMC) in Riyadh, Saudi Arabia, during the 6-month period from November 2012 to April 2013. KAMC is a 900-bed non-profit academic and tertiary center with a population catchment area of approximately half a million and has a well-established thrombolysis program and stroke unit. Case identification was through ascertainment by hospital neurologist and confirmed by imaging. All identified cases of both genders were candidates for inclusion in the study if they were 18 years or older and did not develop the stroke while in the hospital. The time of stroke onset was documented as the time the patient or an observer first noticed signs and symptoms of stroke.17,18 After approval was obtained from the appropriate institutional review boards, patients were interviewed.
Interview and data collection
Nurses and medical residents were recruited as interviewers. Interviewers were taught the procedure of obtaining informed consent, the methods of administering the structured questionnaires and recording the responses. Following case identification, the interviewer was informed and written consent was obtained from all patients who agreed to participate by the interviewer prior to the start of the interview. If patients had communication deficits, a caregiver who resided with the patient was consented and interviewed. The interviewer knew only that the patient had been diagnosed with a stroke and that we wanted to know more about the reasons why participants did or did not delay seeking medical attention. A one group test with a 0.05 two-sided significance level will have an approximate 80% power to detect the differences between the null hypothesis proportion and of 0.45 and the alternative proportion of 0.55 for a required sample size of 227. The questionnaire used in the interview was developed based on preliminary in-depth interviews with healthcare providers who dealt with stroke patients on a daily basis and with a sample of patients diagnosed previously with stroke at the same institution. This method that was used for the development of the domains of the instrument is recommended because of its ability to yield evidence of the face validity of the constructs of the instrument for use among the target population. 19 The instrument was subsequently tested by study investigators on 12 patients for clarity, feasibility and time management and further revised for content validity by a neurologist prior to the start of the study. The final structured instrument included 24 questions with a variety of close-ended and open-ended answer formats on the topics of demographics (such as age, gender, nationality and place of residence), socioeconomic factors (such as education, employment status and income), physical activity and smoking status, pre-existing morbidities and risk factors, pre-existing disabilities, stroke symptoms and knowledge of stroke warning signs. Participants were also asked whether they had ever heard about stroke and from whom, and whether they knew the “Red Crescent” number (an emergency care and transportation service similar to the “Red Cross”). Questions that were related to transportation mode to the hospital, destination after experiencing signs and symptoms, arrival date and time, and time seen by the physician were also documented. A question was included that related to the perceived barriers preventing early arrival to the hospital. At the end of the interview, each patient was asked an open-ended question about their illness experience, their interpretation of the signs and symptoms and their perceived barriers for their late presentation for treatment after stroke. Questions were read to the participants by the interviewer. The structured interview took about 20 min to complete.
Analysis
Data were analyzed for statistical significance using the procedures of logistic regression of Stata 13.0. Arrival time after stroke was the dependent variable dichotomized as either early (≤4.5 h) or late (>4.5 h). Various variables such as demographics (age dichotomized as ≤60 or >60 years and gender), socioeconomic status (income categorized as ≤7000 Saudi Riyals (SR) or >7000 SR and education split into two categories; less than high school education and high school graduate or more), behavioral risk factors (physical activity and smoking status), knowledge about signs and symptoms of stroke, knowledge about available emergency services, comorbidities, factors related to the experience with stroke and interpretation of signs and symptoms, and perceived barriers to delayed presentation for treatment after acute stroke were the independent variables.
Univariate analyses were performed to assess the association of each of the independent variables and arrival time for care (early vs delayed). Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for all comparisons. To determine which factors were predictive of later arrival when adjusted for other predictors, a multiple logistic regression was performed with all variables that showed significance with the univariate analysis (p ≤ 0.05). Stepwise backward elimination was applied for all variables that did not show significance. The final model fit was assessed with the Hosmer–Lemeshow test.
Results
Characteristics of patients and methods of presentation after stroke onset
During the 6-month data collection period, 227 patients (158 with ischemic stroke, 36 with transient ischemic attack and 33 with hemorrhagic stroke) that arrived at the ED were interviewed. There were 156 males and 71 females. The mean age was 60.4 ± 15.6 years. There were 60 patients; 26% who were living outside the city of Riyadh. The demographic characteristics of patients are presented in Table 1. The acute stroke signs and symptoms experienced by the patients included motor weakness 77.3%, speech difficulty 63.7%, dizziness 35.8%, altered level of consciousness 22.7%, visual changes 17.9% and headache 15.7%.
Demographic characteristics of the study population (N = 227).

SR: Saudi Riyals.
A total of 159 patients (70.0%) did not know that they were experiencing a stroke; they attributed their symptoms to exhaustion (16.2%), diabetes complications (10.0%), psychological reasons (3.5%), hypertension (5.7%) or the evil eye (1.7%). A relative or caregiver was present for 215 (94.7%) of the patients during the onset of stroke symptoms.
Of the 227 interviewed patients, 124 (54.6%) presented late (>4.5 h) after onset of stroke and 103 (45.4%) presented early (65 patients in less than 30 min, 9 patients between 90 and 180 min and 29 patients arrived after 180 min). A total of 190 patients (83.7%) initially presented to our hospital, while the rest presented to local primary healthcare centers or consulted with a traditional or religious healer before coming to our hospital. Delayed presentation to the hospital after onset of stroke was attributed to failure to recognize stroke signs and symptoms (61.5%), lack of transportation (14.3%), distance from the hospital (12.1%), lack of awareness about the importance of early arrival to the hospital for treatment of stroke (8.8%), being alone during the onset of stroke (5.0%) and seeking alternative medicine to alleviate symptoms (3.3%). About 18.1% reported arriving at the ED by ambulance, while the majority arrived by private car. As many as 87 patients (38.3%) reported not knowing the number for the “Red Crescent,” the emergency medical service. There were 60 patients (26.4%) who were living outside the city and required a travel time of 30 min or more to reach the hospital.
Factors contributing to late presentation for care after onset of stroke
In the univariate analysis, being alone during the onset of stroke (OR = 10.4; 95% CI: 1.3–82.0), not knowing the emergency services number (OR = 2.0; 95% CI: 1.1–3.3), not being transported in an ambulance (OR = 3.3; 95% CI: 2.0–10.0), not knowing that they were experiencing a stroke (OR = 4.2; 95%CI: 2.0–8.7), residing outside of the city of Riyadh (OR = 30.0; 95% CI: 9.0–99.0) and experiencing blurred vision (OR = 2.3; 95% CI: 1.1–4.9) were factors associated with late arrival to the hospital after the onset of stroke (Table 2). There were no differences between the late versus early arrivals in age, gender, income, level of education, vascular risk factors (diabetes, hypertension, high cholesterol, heart disease or smoking status), pre-existing physical disability, previous stroke experience and different stroke symptoms.
Association of late arrival for treatment after onset of stroke with patients’ characteristics (N = 227).

OR: odds ratio; CI: confidence interval.
SR: Saudi Riyals ≈ US$0.26.
Ref. (1.0): absence of acute symptom.
Ref. (1.0): absence of risk factor.
Ref. (1.0): absence of disability; more than one answer option allowed for symptoms, risk factors and disabilities.
Bolded results are significant.
In the multivariate logistic regression analysis, being alone during the onset of stroke, not being transported in an ambulance, not knowing that they were experiencing a stroke and residing outside the city of Riyadh were factors that remained significant independent predictors of late arrival at the ED after stoke onset (Table 3).
Final logistic regression model results for relative odds for late arrival to the hospital after onset of stroke (N = 227).
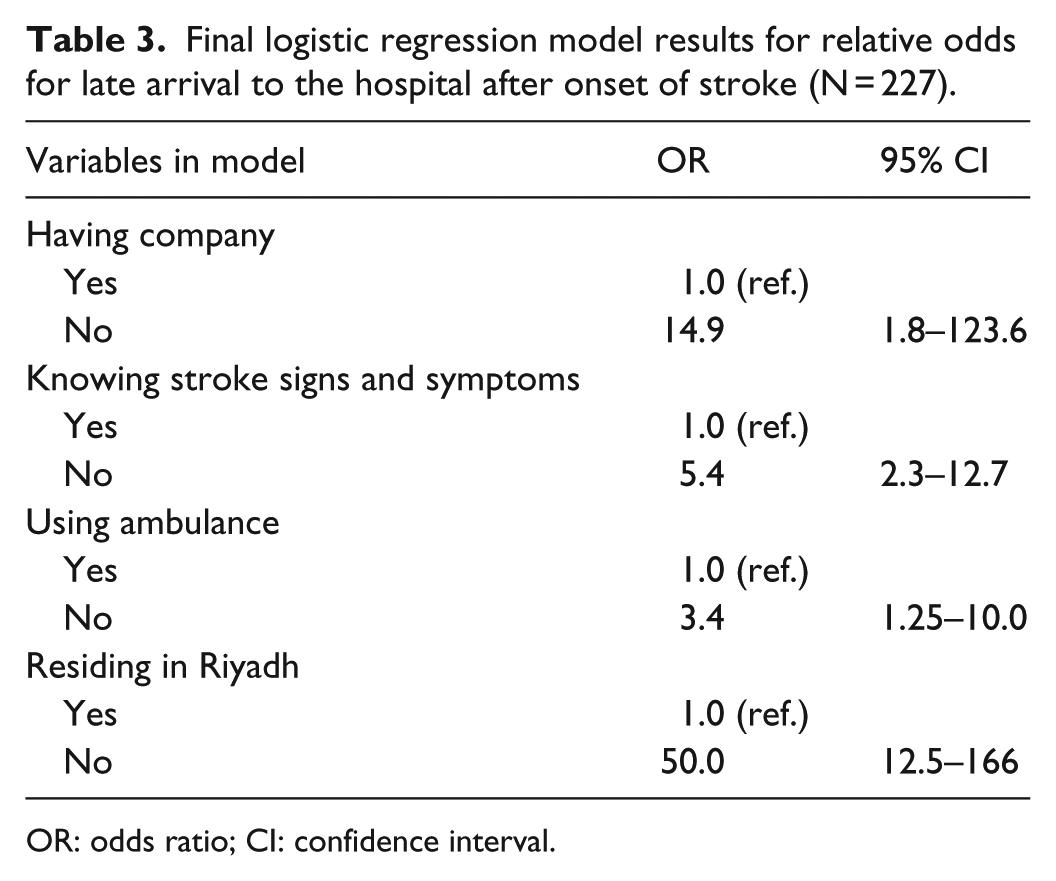
OR: odds ratio; CI: confidence interval.
Discussion
This study highlighted important contributing factors for late presentation after onset of stroke at the ED in a major hospital in Riyadh, the capital of Saudi Arabia. More than half of the patients arrived late after the onset of stroke (>4.5 h). Being alone during the onset of stroke, not being transported in an ambulance, not knowing that they were experiencing a stroke and residing outside the city of Riyadh were factors associated with late arrival, both in univariate and multivariate analyses. Analysis showed that patients who were alone during the onset of symptoms were more likely to arrive late. It has been reported in the literature that living alone is associated with delay in seeking medical treatment.20,21 Also, the study patients who were aware of stroke manifestations and remembered the Red Crescent contact number (emergency services number) were more likely to reach the hospital early. These findings are of particular importance given the known association between the timely treatment of stroke and the increased likelihood that the patient will have better functional outcomes following their stroke. The administration of IV tPA must begin within 4.5 h from the onset of stroke in order to have a beneficial effect. 22 IV tPA remains largely underutilized, with recent international studies estimating that 10%–20% of all eligible patients receive the treatment. 23 These low rates prompted the assessment of IV tPA utilization in different healthcare settings and to devise methods to improve the proportion of patients receiving this treatment. In a study by Barber et al. that investigated 1168 patients presenting to the EDs of the city of Calgary in Canada over a 3-year period, about 73% of patients presented outside the treatment window because they waited to see whether the symptoms would improve on their own. 24 In this study, over half of the patients did not arrive early to the hospital despite their inability to explain their symptoms; additionally over a third of the patients investigated attributed their symptoms to fatigue or diabetes. Patients with prior strokes or with comorbidities did not arrive earlier than other patients for treatment. These findings demonstrate an important lack of knowledge that needs to be targeted by planned educational campaigns especially in high-risk patients. In a survey conducted among 83 practicing neurologists in Saudi Arabia, establishing stroke units and increasing public awareness about stroke were identified as the top priorities for improving stroke care in the country. 16 Also, a recent study conducted among the general population in Riyadh city regarding stroke awareness demonstrated an alarming lack of knowledge about stroke signs, symptoms, and associated risk factors. 25
Among the factors associated with late arrival of patients with stroke was failing to transport the patient by ambulance. Several studies have demonstrated that the use of ambulance services is associated with earlier arrival for care.26,27 Only 18.5% of the patients in this study used ambulance services after stroke onset. This rate of ambulance usage is much lower than what has been reported in other studies where ambulance usage was as high as 60%. 17 In a study of 102 Saudi emergency services personnel, 98% indicated that they would dispatch stroke patients to the nearest hospital, irrespective of the availability of stroke treatment. 28 Educational campaigns targeted at the medical response team personnel will supplement the efforts to ensure timely arrival at facilities with established acute stroke care systems. One other significant factor for late arrival at the ED was living outside the city of Riyadh. Geographical location has been established as a main reason for late arrival in many other studies.17,18,29 Many of the patients in this study presented to their local primary healthcare centers before arrival at the ED. Similar to other studies, consulting with local doctors is a significant reason for delay.26,30,31 A well-established network of local doctors in close and distant proximity to the stroke center to facilitate communication and consultation with stroke specialists, and facilitating the emergency transport system between remote clinics and the stroke center, are all essential for improving the use of thrombolytic therapy in Saudi Arabia.
Limitations of the study
A limitation of this study is that it was conducted in a single center during a 6-month period and the sample size is small. Despite this limitation, this study provided background information on the factors associated with delay in presentation of stroke patients in Saudi Arabia. In order to overcome this limitation, future studies are needed across several hospitals with stroke centers and a thorough evaluation of all factors mentioned in this study as potential causes for delayed arrival of stroke patients for treatment. Also, a bigger sample size to ascertain the findings of this study is highly suggested.
Conclusion
Despite the extended time window for thrombolytic therapy, significant delay in patient presentation is noticed. Studying the factors contributing to delay is a great challenge as the causes cannot be easily limited to one factor. Barriers to arrival for treatment within the recommended time frame among Saudi population should be thoroughly investigated and dealt with seriously to help achieve optimal care for stroke patients, manifested in the administration of the right treatment for the right patient in the right time. While the objectives of this study may have been reported previously in different societies, they are essential steps that need to be described in our society before allocating resources and funding for nation-wide interventions. Many of the factors contributing to the delay in treatment after onset of stroke can be overcome. Health promotion campaigns to improve community awareness of stroke signs and symptoms, transferring patients to hospitals with thrombolysis facilities in a timely manner and efficient use of the ambulance service are strategies to help early presentation for treatment after stroke onset. Taking these basic steps will ensure that stroke care in Saudi Arabia will progress at a steady rate to reach the lead position that it deserves.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from King Saud bin Abdulaziz University for Health Sciences Institutional Review Board. Proposal Number FI/2013.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written Informed consent was obtained from all subjects before the study or written informed consent was obtained from legally authorized representatives before the study in the case that the patient was unable to communicate.