
Abstract
Background:
Our previous work demonstrating great ease and predictability of cannulation of the major aortic arch branches with an upwardly pointing 3DR catheter, irrespective of aortic arch type, led us to hypothesize that centering or “cresting” of these vessels must occur along the superior most aspect of the aortic arch in a curvilinear fashion.
Methods:
We retrospectively analyzed 111 computed tomographic scans of the chest and thoracic aorta with intravenous contrast performed at our hospital between April 2011 and May 2012 utilizing TeraRecon image reconstruction software. Four studies were excluded due to poor image quality and/or surgical changes to native aortic architecture.
Results:
Of the 107 studies included, 104 (97.2%) demonstrated centering of the major aortic arch branches on a curvilinear line “cresting” the superior most aspect of the aortic arch irrespective of arch type. Of the three studies that did not demonstrate this “cresting,” two were found to have aberrant right subclavian arteries associated with a type I aortic arch, and one had an aberrant right common carotid associated with a type II aortic arch.
Conclusion:
Operators engaging major aortic arch branches need to be mindful of the fact that these vessels are indeed centered on a line “cresting” along the superior most aspect of the aortic arch, and any algorithm that, by taking this information into account, reduces catheter manipulation in the aortic arch could potentially result in a reduction in distal atheroembolic events.
Introduction
The ease and predictability of cannulation of the major aortic arch branches (MAAB), irrespective of arch type, with an upwardly pointing 3DR catheter without manipulation as it is gradually withdrawn from right to left led us to hypothesize that a “cresting” of the MAAB must occur along a curvilinear line traversing the superior most aspect of the aortic arch (AA) 1 (Figure 1). Following simple laws of physics dictated by centrifugal forces generated by bending of catheters as they are gently withdrawn in the AA the tip of torque free upwardly pointing 3D RCA catheter automatically seeks this superior most curvilinear line and effortlessly falls into the MAAB take off sequentially. This line is curvilinear and therefore any particular MAAB take off located along this line may not cut through the 12 O’clock position and rather through various positions between 11:45 and 13:00. 2

Steps involved in sequential withdrawal technique with 3DR catheter: (a) the 3DR catheter is positioned in the proximal ascending aorta and withdrawn with the tip pointing cephalad. As the catheter is withdrawn, the slack depicted by the shaded area is eliminated. The catheter invariable intubates the Right brachiocephalic artery (BCA) without torqueing or manipulation and (b) sequential engagement of the Left Common Carotid artery and Left Subclavian then occurs as the catheter is further withdrawn in a torque free manner.
Since distal atheroembolic events are rather common in carotid angiography and interventions both in the targeted and in the non-targeted carotid distributions,3–7 attention to this “cresting” of the MAAB during such procedures may tend to reduce catheter manipulation and the attendant distal atheroembolic phenomena, irrespective of the catheter utilized to engage the MAAB (Vitek, Right Coronary Artery or 3D Right/Williams, etc.).
Aim
The aim of this study is to make operators mindful of the anatomy of the AA and thus leading to improved cannulation of the vessels thereby reducing catheter-related adverse events. This may lead to the development of better and more refined approaches in the future for carotid artery access.
Methods
After obtaining approval from the hospital Institutional Review Board, we retrospectively reviewed 111 computed tomographic (CT) scans of the chest and thoracic aorta done with intravenous (IV) contrast. Data were collected between April 2011 and May 2012, and we included roughly 50% of cases, which were selected to ensure randomization and reduce bias. A total of 111 studies were selected after applying our exclusion criteria and 107 studies on whom complete data were available were made part of the study. Studies were selected randomly for review and the images were deconstructed and analyzed utilizing commercially available TeraRecon imaging software. All bone and extraneous vasculature were removed from the images so that the origins of the MAAB were clearly visible in both two- and three-dimensional views (Figures 2 and 3). The superior most aspect of the aorta was defined manually by adjusting the curved planar reformation (CPR) software-generated reference line and referencing it in both coronal and sagittal views (Figures 3 and 4). This line was then followed in a sagittal bird’s-eye view and marked at its intersection with the origins of the right brachiocephalic, left common carotid, and the left subclavian arteries (Figure 5). A total of four studies were excluded from our analysis: three studies due to poor image quality and/or incomplete filling of the vasculature with contrast and one due to distortion of the AA related to surgical repair. Complete data were available for 107 patients.

TeraRecon image with software-generated curved planar reformation (CPR) line placed in center of aortic arch.
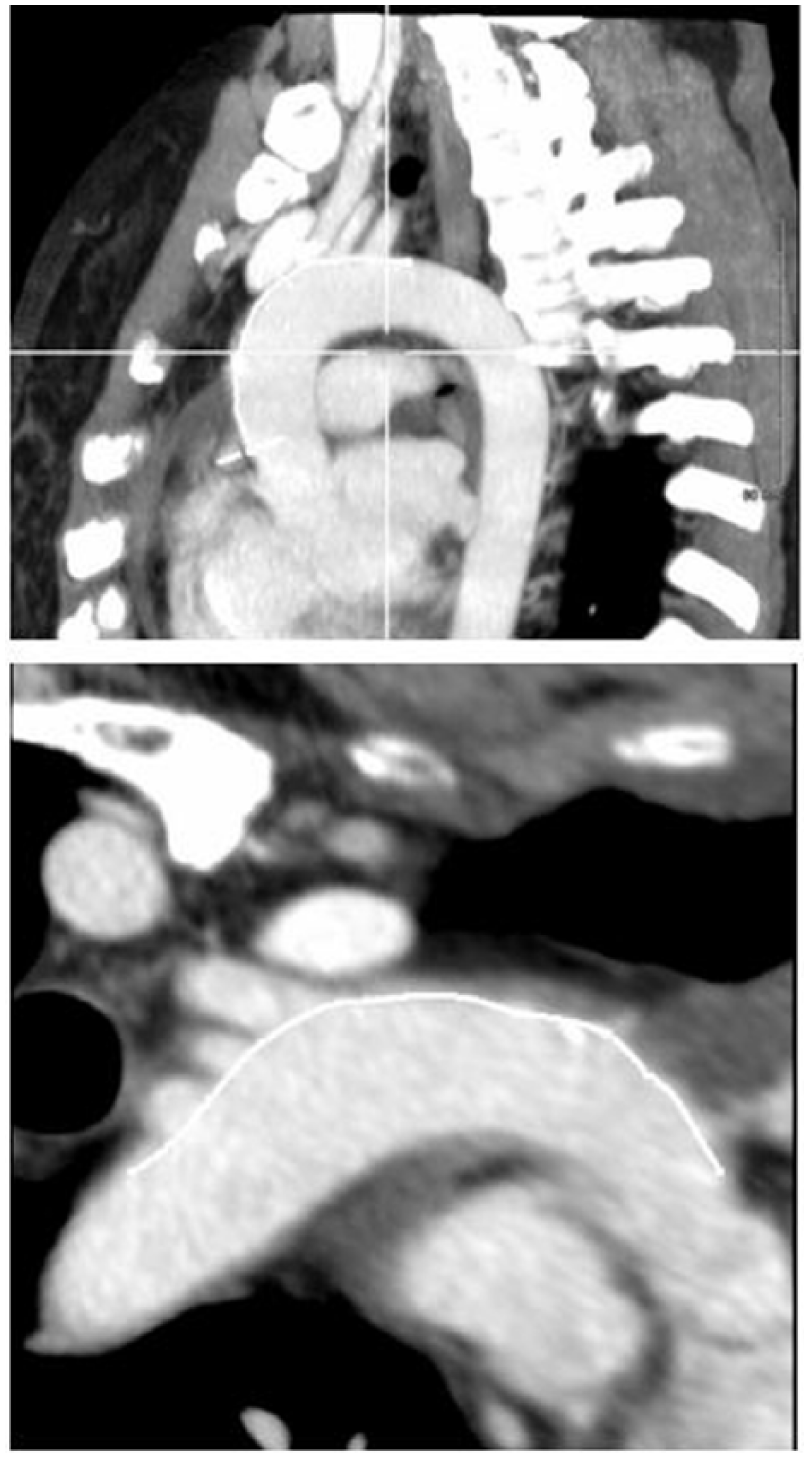
Manual CPR line adjustment to superior most aspect of aortic arch on two-dimensional image.

Corresponding curved planar reformation line positions at superior most aspect of aortic arch on three-dimensional TeraRecon image reconstructions.

Intersection of curved planar reformation line with origination of brachiocephalic vessels.
AA type was determined by CT scan. Type I AA was defined as an arch in which the MAAB arise from the outer curvature of the arch in the same horizontal plane without angulation and where the vertical distance from the origin of the right brachiocephalic artery (BCA) to the top of the arch is <1 diameter of the left common carotid artery (CCA). Type II AA was defined as an arch in which the MAAB arise between the parallel planes delineated by the upper and lower curves of the arch representing moderate angulation and where the vertical distance from the origin of the right BCA to the top of the arch is between 1 and 2 diameters of the left CCA. A type III AA was defined as an arch in which the right BCA arises proximal or caudal to the lesser curvature of the AA and where the vertical distance from the origin of the right BCA to the top of the arch is >2 left CCA diameters8–10 (Figure 6). Bovine AA was defined as a common origin of the right BCA and the left CCA. The patients were then compared according to baseline characteristics inclusive of age, gender, height, weight, body surface area, history of hypertension, coronary artery disease (CAD), diabetes mellitus, and arch type.
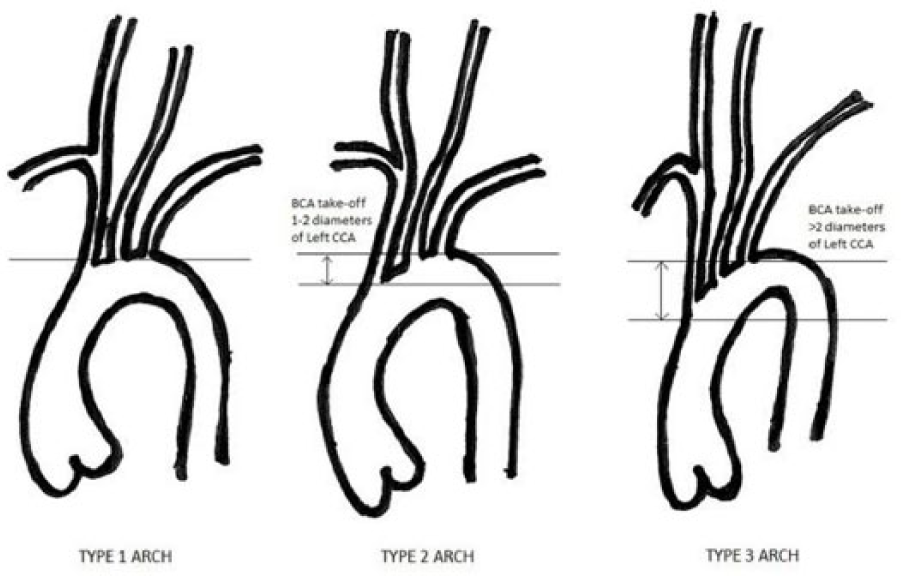
Aortic arch types.
Statistical analysis
Data were collected and stored on Microsoft excel sheets. Statistical analysis was completed using SPSS version 20 to assess frequency and prevalence of various aortic arch types. Demographic data were also stored in a similar way and all results are presented in Table 1.
Patient demographics based on 107 patients with complete data.

BSA: body surface area; HTN: hypertension; DM: diabetes mellitus; CAD: coronary artery disease; BCA: brachiocephalic artery.
Inclusion criteria. All patients 18 years of age or older undergoing computed tomographic angiography (CTA) of the coronaries arteries or CT imaging of the chest and/or thoracic aorta with IV contrast.
Exclusion criteria. Any criteria excluding a patient from receiving a CT scan with IV contrast, including but not limited to, renal insufficiency/failure, pregnancy, or known contrast allergy. Additionally, patients with known congenital anomalies, or who had undergone previous endovascular repair, stenting, or cardiothoracic surgery requiring arch reconstruction, or morbidly obese patients too large to fit in the CT scanner were excluded.
Results
The mean age of the 107 patients on which complete data were available was 58.2 ± 15.9 years. Of these patients, 58.9% were hypertensive, 11.2% had CAD, and 20.5% had diabetes.
A total of 64 of the 107 (59.8%) of patients had a type 1 AA, 14/107 (13.1%) had type 2 AA, 10/107 (9.3%) type 3 AA, and 19/107 (17.8%) had a bovine AA which is generally consistent with larger demographic studies of AA anatomy.
Ninety-seven percent of the patients studied (104/107) demonstrated “cresting” of MAAB take off along a curvilinear line following the superior most aspect of the aorta (Table 1). Of the three studies that did not exhibit this “cresting,” two were found to have aberrant right subclavian arteries associated with a type 1 AA, and one had an aberrant right CCA associated with a type 2 AA.
Discussion
Numerous human cadaveric and CT scan–based studies have reviewed the prevalence of AA type and branching patterns. 11 The bovine arch anomaly is well known with its incidence in the general population varying from 20% to 27%.11,12 In Demertzis et al.’s review of 92 living patients aged 69.4 ± 9.9 years, they found that 47% of patients had a type I AA, 36% to have a type II AA, and 17% to have a type III AA. In our cohort of patients, 59.8% had a type I AA, 13.1% type II AA, 9.3% type III AA, and 17.8 % had a bovine AA. A higher prevalence of type I AA in our series may in part be explained by the fact that our patient population was considerably younger at 58.2 ± 15.9 years. While some authors state there is no association of AA type with age, others clearly suggest significant age-related changes occur over time, in particular in the setting of prolonged hypertension.9–11 Our previous work also confirms increased prevalence of type II and III AA with increased age and in patients with left ventricular hypertrophy (LVH). 12 These age-related changes in AA anatomy generally coexist with increased calcification, tortuosity, and elongation of the transverse, ascending and descending aorta especially in patients above the age of 80 years. 13 Both Lam and Katstrup suggested in retrospective subgroup analyses in the carotid revascularization endarterectomy versus stenting trial (CREST) that altered arch anatomy was associated with significantly higher periprocedural cerebrovascular events especially in octogenarians.10,11,13–16 Furthermore, in a review of 298 cases, Faggioli et al. 10 found that arch type was the only variable independently associated with neurological complications.
Therefore, any algorithm that incorporates methodology for an atraumatic cannulation of the MAAB especially in the setting of type II and III AA may lend itself to enhanced procedural safety during brachiocephalic interventions including carotid stenting. Thus, our finding of near universal “cresting” of the MAAB along a line “cresting” the superior most aspect of the AA in a curvilinear fashion irrespective of arch type may be information that needs to be factored into the calculus when engaging MAAB during brachiocephalic interventions like carotid and subclavian artery stenting.
Limitations
Limitations of our study include a single center study with a small sample size. Larger studies would be needed possibly with cadaveric arch analysis to validate cresting of AA. Another limitation to this study is sample size, and the power thereof. Our study population was retrospectively attained and included everyone who received at CT chest and thoracic aorta between the above said time period. The 111 patients do not provide sufficient power for true external validity, but rather a snapshot. While significant, our results should not be taken out of context.
Conclusion
When performing brachiocephalic interventions including carotid stenting, operators need to be mindful of the fact that irrespective of arch type, the MAAB are centered along a “crest” traversing the superior most aspect of the AA.
Any algorithm that results in reduced catheter manipulation by taking the above information into account while cannulating MAAB could result in a reduction in distal atheroembolic events, especially those occurring in the non-targeted cerebrovascular territories.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was waived by institutional review board (IRB) at Newark Beth Israel Medical Center as this was a retrospective study with evaluation of imaging and demographic data. No drugs or interventions were used and patients were deidentified and investigators were blinded during analysis. IRB approval #2017.21
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
The requirement to obtain written informed consent was waived by the Institutional Review Board because our study was a retrospective chart review in which standard of care was not altered in any way. The patients had already undergone imaging which was used in our study.