
Abstract
Objectives:
Our goal was to assess the association between potentially inappropriate medication use and risk of falls in the Parkinson’s disease population.
Methods:
This was a retrospective cohort study conducted at an outpatient Parkinson’s Disease Treatment Center. Individuals 65 years of age or older, diagnosed with Parkinson’s disease who attended at least three visits in 2015 for physical, occupational therapy, or physician’s visits were included in the study. Electronic medical records were utilized to perform chart reviews, and medications were analyzed to identify prescription medications, combination preparations, over-the-counter medications, and dietary supplements. The goal of this study was to test the following hypothesis: elderly individuals with Parkinson’s disease who take multiple potentially inappropriate medications are more likely to experience a fall compared to elderly individuals with Parkinson’s disease who do not take multiple potentially inappropriate medications.
Results:
A higher mean number of prescription medications were associated with falls in elderly Parkinson’s disease patients (6.53 vs 5.21, p < 0.01). Polypharmacy (taking five or more prescription and nonprescription medications) was not significantly associated with falls. Patients taking potentially inappropriate medications specifically contraindicated for those with a history of falls and fractures were more likely to report falls (p < 0.04). Analysis of the specific therapeutic medication categories demonstrated no significant differences between those who did and did not report falls.
Conclusion:
A future prospective study at Parkinson’s disease center should include an electronic medical record–based intervention to reduce the total number of medications, as well as to minimize the use of high-risk medications.
Introduction
Parkinson’s disease (PD) is a neurodegenerative movement disorder that typically presents with tremor, rigidity, bradykinesia, and impaired balance. 1 The prevalence of PD continues to rise with aging population. 2 An association between drugs and falls in the elderly has long been studied.3–7 In part due to aging, and in part due to the symptoms of the disease, individuals with PD are at an increased risk of falls, with annual fall rates ranging from 46% to 68% in some PD populations which puts them at a significantly higher risk of suffering from fall-related injuries than the general population. 8 Thus, falls negatively impact mobility and activities of daily living in PD patients, affecting their quality of life. 9
The American Geriatrics Society Beers Criteria recently updated criteria for potentially inappropriate medications (PIMs) that have unfavorable balance between adverse events and benefits linked to poor patient outcomes including falls. 10 Almost 30% of adults over 65 years of age regularly use five or more prescription medications. 11 Polypharmacy, defined by the World Health Organization as the “use of too many medicines per patient,” 12 has been associated with adverse drug events, hospitalization, mortality, and falls; however findings are mixed, and there is heterogeneity between studies. 13 Additionally, there is a lack of consensus in the literature regarding the definition of polypharmacy.6,7,14
Multiple research studies have focused on the etiologies and consequences of falls in individuals with PD; however, the association of the use of multiple PIMs and falls in PD has not been studied, to our knowledge. The purpose of this retrospective study was to test the following hypothesis: elderly individuals with PD who take multiple PIMs are more likely to experience a fall compared to elderly individuals with PD who do not take multiple PIMs.
Methods
This retrospective cohort study was conducted at the Adele Smithers Parkinson’s Disease Treatment Center of the New York Institute of Technology’s (NYIT) College of Osteopathic Medicine (Old Westbury, NY). Depending on the needs of the patients, weekly sessions include one-on-one visits with occupational, speech, physical therapist, psychologist, and/or physician specializing in osteopathic manipulative medicine. Medication lists are updated at each office visit by a physical therapist and/or physician. This study was approved by the institutional review board of the NYIT on 3 May 2016, and the waiver of the informed consent was granted.
PD individuals aged 65 years and older of both genders were included in the study. Exclusion criteria were long-term therapy for addiction, less than three office visits and patients younger than 65 years of age. Since there is no prior literature on the incidence of falls in those individuals with Parkinson’s disease who do not take medications, sample size was calculated for multiple regression using a range of potential effect sizes. With a small effect size of 0.2, assuming alpha = 0.05, a power of 80%, the following minimum sample size would be needed: 51. With a medium effect size of 0.5, assuming alpha = 0.05, a power of 80%, the following minimum sample size would be needed: 23. With a large effect size of 0.8, assuming alpha = 0.05, a power of 80%, the following minimum sample size would be needed: 16. We aimed to collect at least 100 subjects.
Of the 199 individuals screened, 41 were excluded due to age or fewer than three office visits. Patients with less than three office visits were excluded from the study due to lack of continuity of care and incomplete medical records.
We analyzed data from electronic medical records (EMRs) of 158 individuals with PD, 65 years of age or older who attended at least three visits in 2015 for physical, occupational therapy or physician’s visits. All subjects were diagnosed with PD (ICD G20) by a licensed neurologist based on distinguishing clinical features and diagnostic criteria. 15
Data were collected on quantity of medications, pharmacologic or therapeutic categories and net of sociodemographic controls, including age, gender, and race/ethnicity. A chart review was performed, and medications were analyzed to identify prescription medications, combination preparations, over-the-counter medications, and dietary supplements. The total number of prescribed medications was calculated by subtracting dietary supplements and over-the-counter medications from the total list of medications reported.
Polypharmacy was defined as the regular use of five or more prescription medications. 14 Medication lists were cross-referenced with PIMs from the AGS 2015 Beers List, as well at the PIMs contraindicated in specific populations including PD and those with a history of falls and fractures. 10 Data were also analyzed using a definition or six or more or seven or more medications as the cutoff for polypharmacy, to ensure that the definition did not affect our results.
History of a diagnosis was reported for PD, balance disorders, depression and anxiety disorders, diabetes, chronic pain, dementia, hypertension, arthritis, osteoporosis, and vision problems. Fall-related history included number of falls during study period, injuries associated with falls, hospitalizations from falls, alcohol use, fear of falling, freezing, reported loss of balance, and use of a walking aid. The Centers for Disease Control and Prevention (CDC) defines a fall when “a person unintentionally comes to rest on the ground or another lower level, with or without loss of consciousness.” 16 Freezing (difficulty initiating gait) is an important motor symptom of PD that plays a role in increasing fall risk in these patients. 8
Differences between comparison groups were tested using a chi-square or Fisher’s exact statistic for categorical variables and a t-test for continuous variables. For multivariable analysis of categorical outcome variables, unconditional logistic regression was used to estimate odds ratios and 95% confidence intervals, adjusted for any covariates for which there was a significant difference in results between the two comparison groups. As demographic variables were not significantly different between groups, they were not adjusted for. Freezing, an independent risk factor for falls, was distributed differently between groups, and thus, logistic regression was performed adjusting for this variable.
Results
Table 1 shows the demographic characteristics of the study population. Of those enrolled, 81 participants (51%) reported ≥1 fall and 77 (49%) reported no falls. The mean age, gender breakdown, and racial breakdown were not significantly different between those who reported falls and those that did not report falls. There was a statistically significant difference between the two groups in reported incidences of freezing. Of those who reported falls, 55.56% (n = 45) reported freezing, while 24.68% (n = 19) of those who did not report falls, reported freezing (p < 0.0001).
Demographics of the study population.
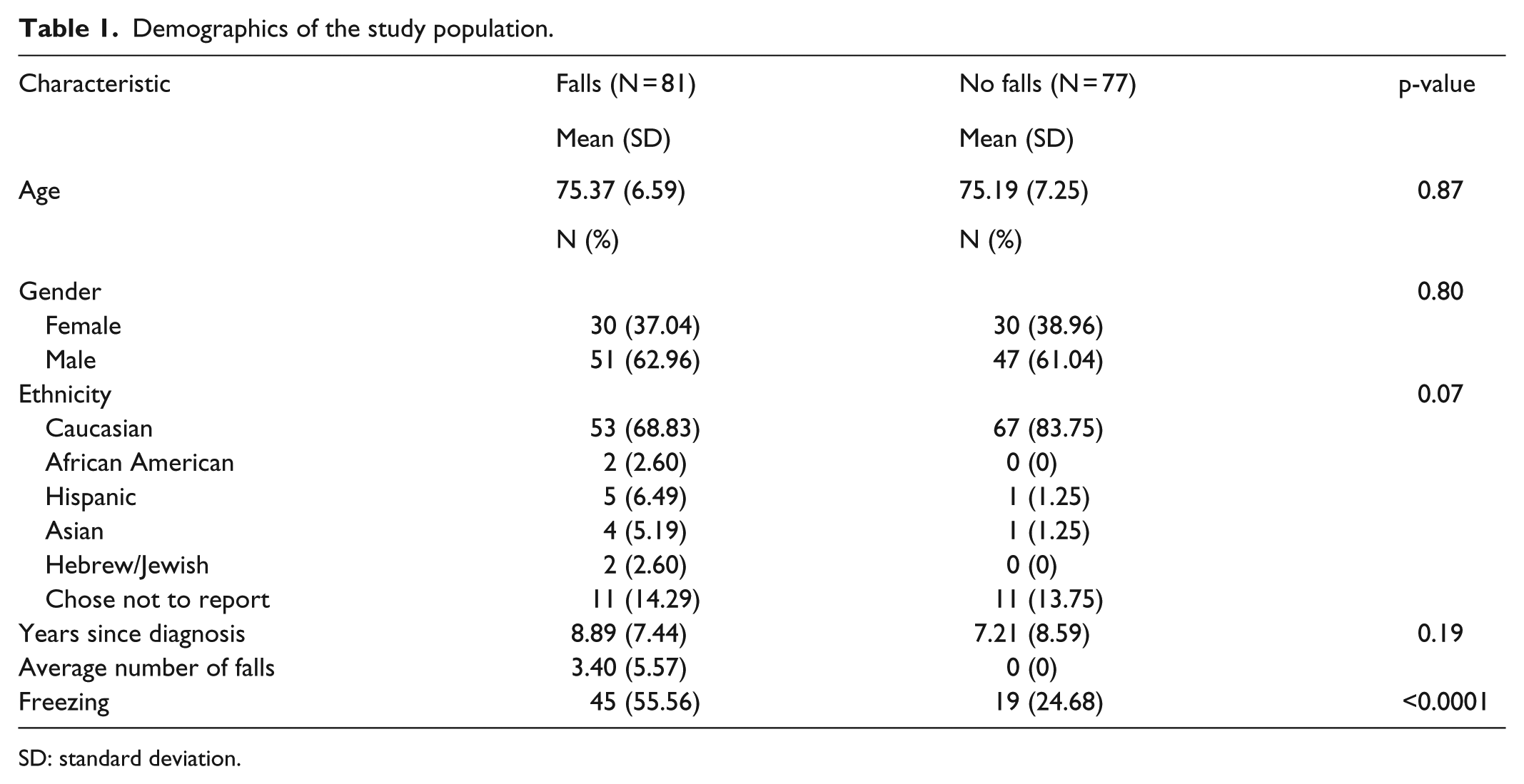
SD: standard deviation.
Table 2 shows the breakdown of comorbidities in the study population. The percentage of history/presence of depression or anxiety in those also reported falls was 35.8% (n = 29) and 17.11% (n = 13) in those not reporting falls. There was a statistically significant difference in depression and anxiety between the two groups (p = 0.01). There was no significant difference in other comorbidities including diabetes, hypertension, arthritis, osteoporosis, and vision problems between fallers and nonfallers.
Study population stratified by comorbidities.

Table 3 shows the mean number of medications used by those who did and did not report falls. The mean number of prescription medications taken by those who reported falls was 6.53 (standard deviation (SD) = 3.31), while in those who did not report falls, the mean number was 5.21 (SD = 2.63). The difference was statistically significant (p = 0.01). The mean number of PIMs contraindicated in patients with history of falls taken by those who reported falls was 0.55 (SD = 0.50), while in those who did not report falls, the mean number was 0.34 (SD = 0.48). The difference was statistically significant (p = 0.01). There were no differences between those who did and did not report falls in terms of total number of medications, number of over-the-counter medications, or number of PIMs.
Medication use and falls.

PIM: potentially inappropriate medication; SD: standard deviation.
Table 4 shows the use of specific categories of drugs used by those who did and did not report falls. There were no statistically significant differences seen between groups in terms of use of specific medication categories.
Specific categories of medication use and falls.

COMT: catechol-O-methyl transferase.
Table 5 shows the odds of medication use by those who did and did not report falls. Taking any medication, prescription medications, nonprescription medications, or PIMs was not significantly associated with falls. Taking PIMs contraindicated in patients with history of falls was associated with falls. The odds ratio comparing use of these medications in those who reported falls versus those who did not report falls was 2.32 (95% confidence interval (CI) = 1.22–4.40, p = 0.04).
Odds ratios for medication use and falls.

OR: odds ratio; CI: confidence interval; PIM: potentially inappropriate medication.
Controlled for freezing.
Table 6 shows the odds of polypharmacy use by those who did and did not report falls. Polypharmacy including all prescription and nonprescription medications was not significantly associated with falls. When data were analyzed using a medication cutoff or six or seven or more medications, no significant results were seen (data not shown).
Odds ratios for polypharmacy a and falls.
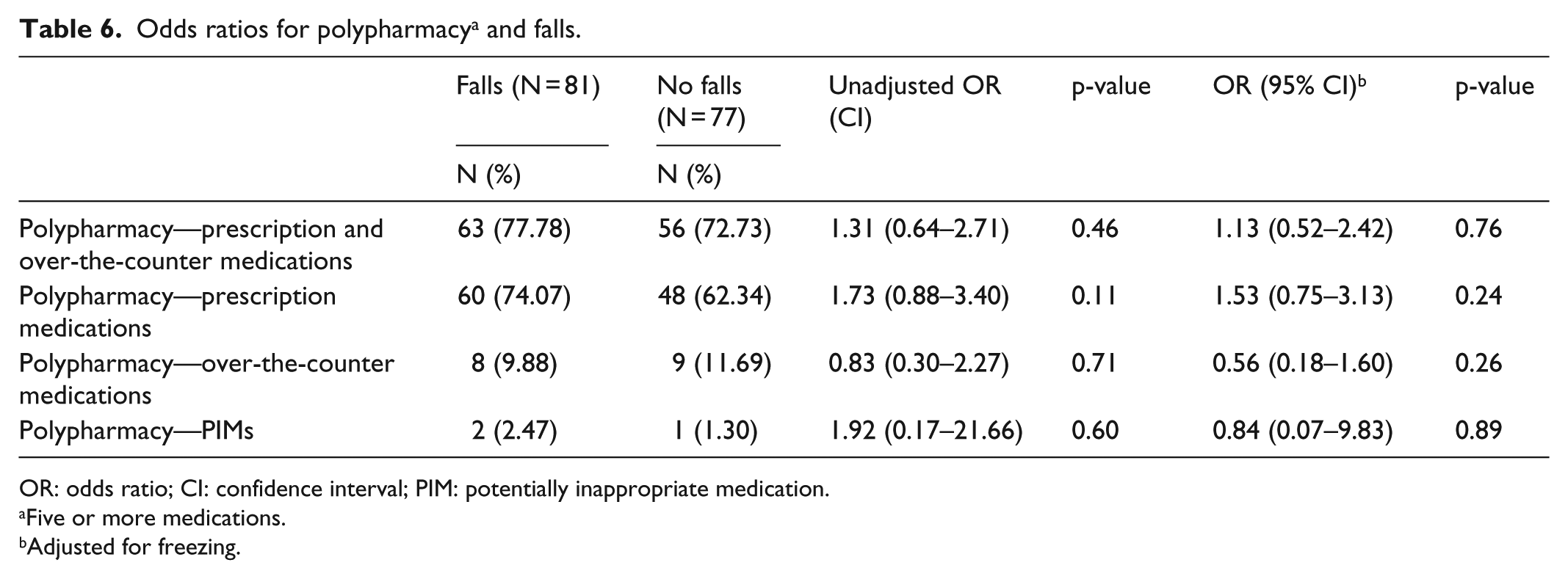
OR: odds ratio; CI: confidence interval; PIM: potentially inappropriate medication.
Five or more medications.
Adjusted for freezing.
Discussion
The practice of prescribing multiple medications to older patients is associated with adverse events in the literature, including the potential of drug–drug interactions and serious adverse effects of medications, including hospitalizations.17,18 In this study, we found that individuals taking PIMs specifically contraindicated for those with a history of falls and fractures, per Beers guidelines, were more likely to report falls. 10 Analysis of the specific therapeutic medication categories demonstrated no significant differences between those who did and did not report falls.
Our findings are supported by those reported from the population-based prospective cohort study which demonstrated that fall risk is associated with daily use of multiple drugs only when at least one drug is an established fall-risk increasing drug. 7 Others showed that the use of more than one prescribed medication can double the risk of falls leading to hospitalizations, even after adjusting for demographics, social circumstances, or comorbidities. 19
With regard to specific medication categories, previous studies reported mixed results. Schrag et al. 20 found no association between the use of sleep medications and falls in PD, while others reported higher risk of falls in elderly individuals taking long-acting benzodiazepines and sedative hypnotics.3,21,22 The use of antidepressants (selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs)) and neuroleptics was previously reported to be associated with falls in PD patients. 20 We did not find this association in our study.
It is noteworthy that of the 158 individuals observed, 104 were prescribed at least one PIM. Prevalence of PIMs (66%) in our sample of elderly individuals with PD is much higher than PIM prevalence of 22%–30% documented in studies of community-dwelling elderly populations,23,24 therefore making it difficult to compare published studies on the elderly and falling with our own study.
We found that depression and anxiety in individuals with PD were associated with falls. Similar research findings in community-dwelling elderly population demonstrated that depressive symptoms increase the risk of falls, independent of the use of antidepressant medications.25,26 These findings and high prevalence of depression in PD population 27 suggest a potential benefit of screening for depression in Parkinson’s patient in multifactorial fall prevention interventions. 25 In our study, freezing was associated with falls, similar to what has been previously reported. 28 No association between falls and arthritis, or other chronic diseases, such as diabetes, hypertension, osteoporosis, or vision problems, was found.
Among limitations of this study method is its retrospective design. However, reliability and validity of retrospective chart review for this type of study have been previously shown by others.17,29–32 Other potential limitations are the small size of sample and reliability of the collected data. It is possible that there was a lack of significant effect seen with these PIMs due to the small sample size. The data were also limited in that information on medication dosages was not gathered, and no information was available in the medical charts on severity of PD disease, and thus, these variables were not controlled for. Finally, data collected from EMRs on prescribed medications may be incomplete or missing.
A challenge to this study was defining the appropriateness of medications. Medications identified by the updated Beers criteria are “potentially inappropriate,” not “definitely inappropriate” due to complexities of pharmacotherapy in older patients with comorbidities. 33 Clinicians caring for PD patients should use the 2015 AGS Beers criteria as a starting point for identification of potentially harmful medications and search for safer alternatives. 33
CDC has recognized a need to increase awareness among primary care physicians to conduct comprehensive medication review as part of the fall-risk assessment in the elderly. 34 This medication review should include an evaluation of number of medications and screening for PIMs, eliminating of potential therapeutic duplications, and screening for drug–drug interactions. 35
A future prospective study at PD center should include an EMR-based intervention to reduce the total number of medications, as well as minimize the use of high-risk medications. EMR has been previously used to conduct a comprehensive medication review in vulnerable patient population6,36 and to alert the primary care physician of the changes that may help to prevent falls. 6
Despite its limitations, the results of this study demonstrate that a higher mean number of prescription medications were associated with falls in elderly individuals with PD. This demonstrates the importance of conducting a comprehensive medication review as part of a multifactorial fall prevention program in PD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from New York Institute of Technology Institutional Review Board BHS-1197.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent requirement was waived by the IRB.