
Abstract
Background and Objectives:
Previous studies have emphasized the importance of effectual communication during patient handoffs. The objectives of this study were to (1) implement a resident-driven quality improvement project to improve handoffs by including key elements that are necessary for a safe and effective handoff. We chose to use the IPASS (illness severity, patient summary, action items, situation awareness and contingency planning, synthesis by receiver) mnemonic as our standardized handoff model; (2) Consider balancing measures in an effort to be aware of any negative effects of our interventions on resident satisfaction with the system.
Methods:
A senior resident established a quality improvement team which developed an AIM statement (a written, measurable, and time-sensitive description of the goal of a quality improvement team) and key drivers. A survey was administered to residents regarding their opinions about the handoff process. Tracking of whether or not handoffs included the component IPASS elements was performed over an 11-month period. During this time frame, three Plan-Do-Study-Act cycles were conducted. The first was an educational series involving lecture and role playing. The second was printed cards listing appropriate handoff elements. Intervention three was development of a tool and method to decrease nurse interruptions during handoff.
Results:
Inclusion of six key elements of handoffs improved as follows. Illness severity improved from 5% to 97%, diagnosis from 60% to 100%, patient summary from 71% to 100%, contingency planning from 10% to 100%, action list from 23% to 100%, and receiver synthesis from 0% to 97%. Balancing measures showed the residents were more satisfied with the new system and found it to be more effective at providing a safe transition of care.
Conclusion:
Implementation of a resident-driven multidisciplinary IPASS handoff system resulted in improved inclusion of key handoff elements and increased resident satisfaction.
Improving the communication of IPASS elements during resident handoffs: a resident-driven quality improvement project
The importance of an effective patient handoff between resident physicians at shift change continues to gain exposure in the literature. It is well known that errors in communication account for nearly two-thirds of all sentinel events within a hospital. 1 A study by Brannen et al. 2 in 2009 reported that while 75% of resident handoffs had agreement about the severity of the patient’s illness, there was a low agreement between giver and receiver about the most severe problem and the total problem list. Residents have recognized this gap in receiving and integrating information leads to negative patient outcomes. A 2008 study by Kitch et al. 3 found that 59% of residents reported one or more patients had been harmed due to problematic handoffs; 12% reported the harm had been major.
The issue has come to the attention of the Accreditation Council for Graduate Medical Education (ACGME), which has mandated institutions to provide formal training in and faculty monitoring of patient handoff skills. 4
Recent studies have reported success with implementation of a structured handoff system. In 2012, Starmer et al. developed the IPASS (illness severity, patient summary, action items, situation awareness and contingency planning, synthesis by receiver) mnemonic to help prevent error in verbal patient handoffs. The IPASS mnemonic represents the key elements in a successful handoff process: I: Illness Severity; P: Patient Summary; A: Action Items; S: Situation awareness and contingency planning; S: Synthesis by receiver. 5 Further study by this group in 2013 demonstrated a decrease in medical errors from 33.8% to 18.3% after the implementation of a multifaceted handoff program using IPASS. 6 Finally, the project was applied to nine residency programs in the United States and Canada with a reduction in the overall medical error rate by 23% and a decrease in preventable adverse events by 30%. 7
In our institution, one of our senior residents became interested in coordinating a multidisciplinary quality improvement (QI) project to improve the handoff process. Our study is unique in that it was resident driven. The primary question of our study was to determine whether a multidisciplinary QI process could improve the inclusion of IPASS elements in resident handoff.
Methods
Setting
The setting is a 25-bed pediatric unit within a children’s hospital which is affiliated with an academic institution. The pediatric medical team typically consists of one attending physician, two to three senior residents, and three to four interns. One of the interns works at night and is directly supervised by one senior who is also responsible for covering the pediatric intensive care unit. Handoff traditionally has taken place between the day interns and night intern with the senior residents supervising. An excel spreadsheet is used for written handoff and must be manually updated with new laboratory and imaging results as well as changes in the treatment plan including intravenous and oxygen therapy and medications. Several deficiencies were often noted in the handoff process including disorganization of the handoff, elements included in the handoff varied greatly from caregiver to caregiver, important information was omitted, and irrelevant information was included.
Human subjects protection
This study was presented to the institutional review board and was given exempt status.
Intervention planning
The chief resident became interested in improving the handoff system after observing multiple deficiencies in the handoff process and envisioned implementing a structured approach to the handoff utilizing a nationally recognized mnemonic. A QI leadership team was established in order to assure that any change in the current system would address concerns specific to this institution. The team consisted of an attending pediatric hospitalist, a pediatric resident, two medical students, and two nurse leaders.
The team decided to evaluate two types of measures: process and balancing. The process measure involved a checklist which was used to document whether or not handoff included all the components of the IPASS mnemonic. These components are illness severity, patient summary, contingency planning, action list, and receiver synthesis. 5 After input from the residents that sometimes diagnosis was not included in handoff, the team added diagnosis as a sixth component. It was decided that even prior to any interventions a good handoff should contain these elements though they might be termed or framed in a slightly different way. The plan was to use the checklist to observe handoff and collect data prior to any intervention and then with each Plan, Do, Study, Act (PDSA) cycle.
The team was aware that changes in the handoff system while positive in many ways could also cause problems. For example, perhaps residents would become frustrated because the new system took more time and as a result less time was available for important patient care. In order to address the possibility of negative consequences, the team decided to also evaluate a balancing measure. This involved giving a pre-questionnaire to residents to evaluate their satisfaction with the handoff system and their view of its effectiveness. To evaluate for internal validity and specifically content validity, the questionnaire was reviewed by two experts: one in QI science and the other in clinical and translational research. Following the expert review, a small internal field test was done to check for face validity utilizing individuals who would not be involved in the study. The questionnaire was given before any interventions and after all PDSA cycles were complete.
The team created an AIM (a written, measurable, and time-sensitive description of the goal of a quality improvement team) statement for the process measure: 90% of handoffs would include all six IPASS components. The team identified key drivers:
Resident knowledge of the six key elements of a good handoff.
Resident belief that the six elements actually matter (i.e. improve patient care).
Resident ability to recall the six key elements during the handoff process.
Residents having uninterrupted time to give a focused handoff.
Attending leadership buying into process and emphasizing importance with residents.
Interventions were planned to address each key driver (Figure 1).

Key driver diagram
Plan-Do-Study-Act cycle I intervention
The first intervention was a three-part educational series involving lecture and role playing. Each of the three sessions was 1½ h in length during the lunch period. The QI leadership team members, hospitalist attendings, and residents participated. The sessions were led by the senior resident with attendings helping lead the small group role playing. The sessions not only provided education regarding the six key elements but also strongly emphasized the importance of good handoffs and good communication in general. Participants had the opportunity to practice giving handoff and received feedback from their peers as well as leadership.
Plan-Do-Study-Act cycle II intervention
The second intervention involved giving the residents printed cards which attached to their nametags and listed the six key elements of a good handoff.
Plan-Do-Study-Act cycle III intervention
Nursing leadership educated nursing staff not to interrupt handoff except for emergencies. During handoff time, nurses were instructed to make a list of their needs to give the resident after handoff. A tool was developed for this purpose (Figure 2).
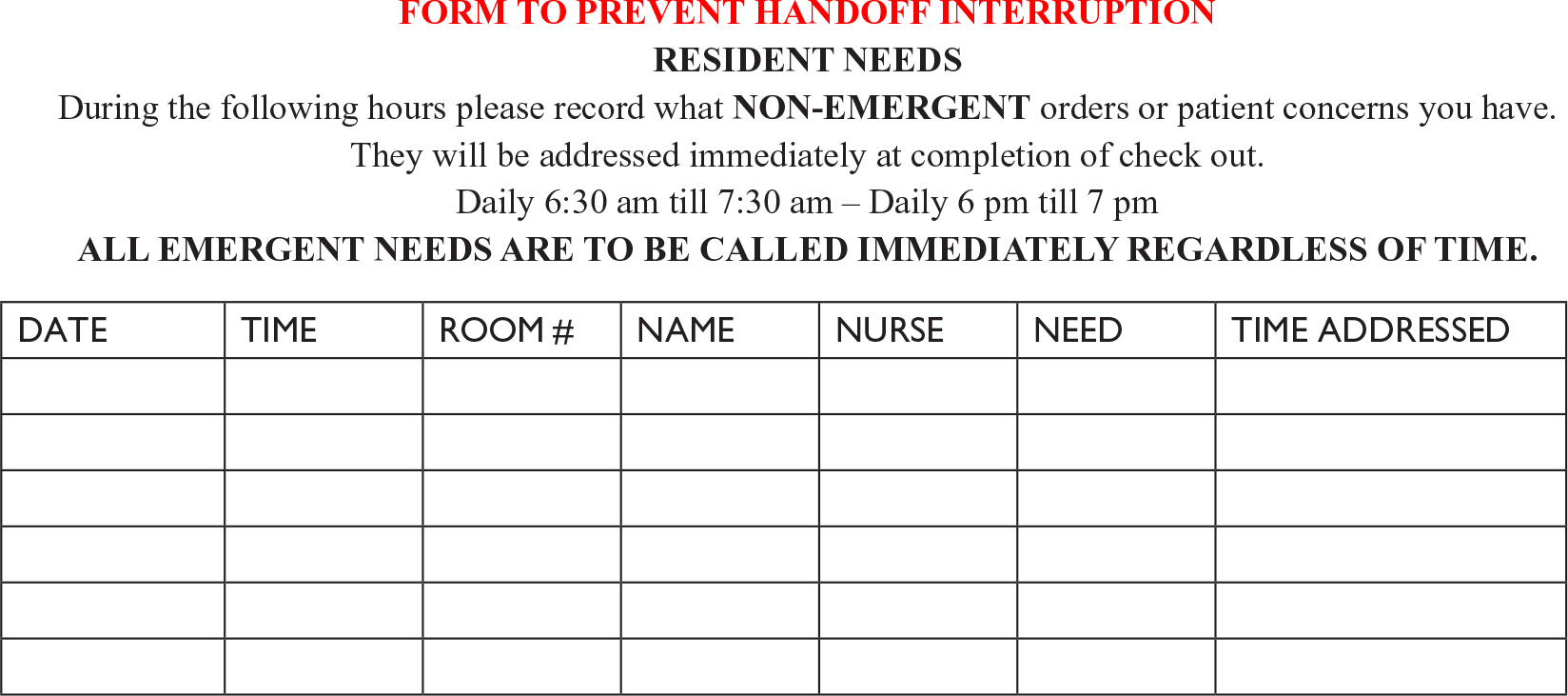
Form to prevent handoff interruption.
PDSA cycles II and III were both expected to cause change by addressing a key element of change theory which is to empower action by removing obstacles. 8 Specifically, cycle II addressed the difficulty organizing an appropriate handoff if one cannot recall the elements and cycle III addressed the issue of lack of focus due to interruptions.
Plan-Do-Study-Act cycle IV intervention
A fourth intervention of having attending physicians present at handoff sessions was planned but the AIM statement was well surpassed at the end of PDSA cycle III, making cycle IV unnecessary. The intent of attending physician presence was to give feedback and encourage the importance of including the six elements.
Data collection
The process data was collected using a checklist on which the observer marked whether or not each patient handoff included illness severity, diagnosis, patient summary, contingency planning, action list, and receiver synthesis. Total time for checkout was also documented. This data collection was done by two members of the QI leadership team. One was the chief resident and the other was a medical student member of the team. In order to assure the quality and adequacy of data collection, the chief resident trained the medical student to recognize the elements of IPASS and observed initial data collection.
For the balancing data, a pre-project questionnaire was developed by the QI leadership team for resident physicians. The questionnaire evaluated satisfaction with the current handoff system, belief in the safety and effectiveness of the system, perceived strengths and weaknesses of the system, whether or not a structured handoff system would be beneficial, and if attending presence would be helpful. A separate questionnaire was developed for use after all the PDSA cycles were complete which reflected the same topics. Both the pre- and post-surveys used a 5-point Likert scale as well as an area for comments.
Analysis
Means on the Likert scale questionnaires were compared using an unpaired t-test. We compared baseline questionnaire data before the first intervention with data following the final intervention. Statistical significance was defined as p < 0.05. In order to assure appropriate rigor, the Mann–Whitney test (two tailed) was utilized for comparison of medians.
Results
The plan for all the PDSA cycles was developed by the QI leadership team. It was determined that more than one cycle would be needed to address all the key drivers.
Process measure
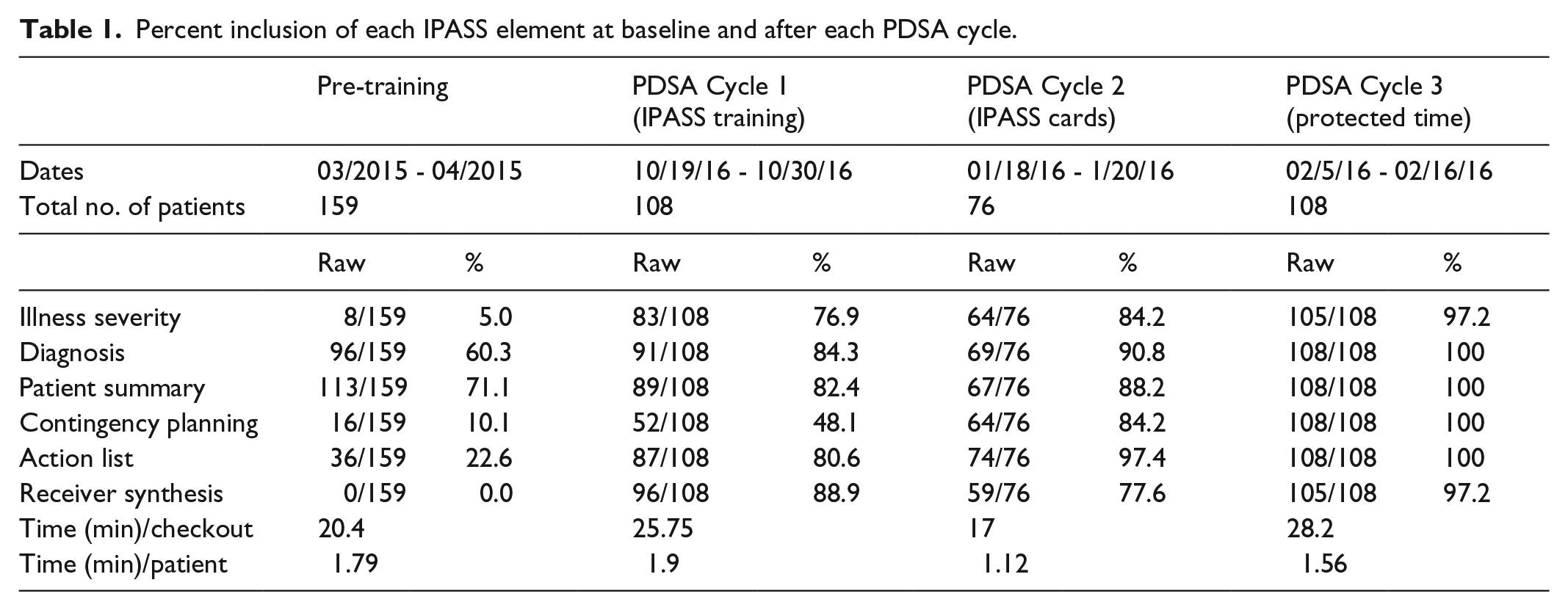
During the study period, a total of 451 patient handoffs were evaluated for inclusion of the six components. Prior to any interventions, illness severity, diagnosis, patient summary, contingency planning, action list, and receiver synthesis were present in 5%, 60%, 71%, 10%, 23%, and 0% of handoffs, respectively. Following all three PDSA cycles, these numbers increased to 97%, 100%, 100%, 100%, 100%, and 97%. Full compliance data showing results after each PDSA cycle are shown in Table 1 and illustrated as a run chart in Figure 3. The time per patient for handoff actually decreased from 1.79 min pre-project to 1.56 min post-project.
Percent inclusion of each IPASS element at baseline and after each PDSA cycle.

Run chart: trending percent inclusion of IPASS elements with each subsequent PDSA cycle.
Balancing measure
A total of 21 residents were anonymously surveyed before the first intervention and following the final intervention. On a Likert scale of 1–5 with 1 being not at all satisfied with the handoff system and 5 being extremely satisfied, the mean score increased from 2.8 to 3.6 (p = 0.007). In regard to the handoff system providing safe and adequate transition of patient information on a scale from not effective to very effective, the mean score was 2.8 at the beginning of the project and 3.7 at the conclusion (p < 0.001). The increase in median score for both satisfaction and effectiveness was also significant at (p = 0.01) and (p = 0.004), respectively.
Written comments were encouraged on both the pre- and post-surveys. The pre-survey comments noted that all diagnoses were not relayed, there were no clear items to be checked out, checkout was not standardized, and there were infrequent contingency plans. On the post-survey, comments noted that handoff was now straightforward, efficient, and structured; it was more effective with fewer interruptions; it was more focused; and the receiver was now clear on which children were the sickest. The only negative comments on the post-survey regarded that handoff took longer. Both the pre- and post-surveys included comments about the written list being time consuming and not self-populating. The majority of residents on both pre- and post-surveys felt that attending presence at some checkouts would be desirable. In total, 11 of the 21 residents said the uninterrupted time was the most helpful intervention in improving their handoffs, while 5 felt the educational sessions were most helpful.
Discussion
We report improved process and balancing measures after our QI project was used to implement the IPASS handoff system for resident physician checkout. Prior studies regarding IPASS implementation have shown an association with decreased medical errors and adverse events as well as increased resident and faculty satisfaction. However, to our knowledge, this is the first report demonstrating a grass roots, resident-driven QI project with successful process and balancing results. A direct comparison between prior studies and our work cannot be made as we did not evaluate outcomes such as decreased medical errors and adverse events; however, we did show comparable results in regard to fewer omissions of key handoff elements and resident satisfaction with the process.
Even though the written list was noted both pre- and post-project to be a negative time-consuming process, we were able to improve resident satisfaction by only addressing the verbal process. Members of our team did meet with administration regarding obtaining an IPASS-compatible electronic medical record (EHR) handoff tool. This was in fact approved but has still not been purchased, and we did not want to wait to begin our improvement process. Our success is a testament to the ability of the frontline person to improve patient care at very little expense. It is interesting that some residents commented the new process takes longer even though it actually is shorter.
Previous studies have shown that handoff quality can be negatively impacted by the working atmosphere including interruptions from frequent nursing phone calls.9,10 Our multidisciplinary team developed a unique method and tool to dramatically decrease these interruptions. The majority of our residents felt this decrease in interruptions was the most useful intervention of our QI team.
A limitation of our study is that it is a small study conducted in one institution. Results may not have generalizability to other centers and situations. For example, our balancing measure questionnaire was not evaluated for external validity. In addition, our improvements may not be sustainable and may weaken over time.
Conclusion
A resident-driven multidisciplinary QI process is an effective method to implement the IPASS handoff system. This can result in improving the handoff process and improving resident satisfaction with the process. Future goals are to look at the outcome measure of adverse events and medication errors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Marshall University Institutional Review Board (IRBnet ID# 735003-1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: An internally funded medical student stipend was provided to Lauren Burley for participation in research. The authors have no financial relationships relevant to this article to disclose.
Informed consent
Informed consent was not sought for this study because EXEMPT STATUS approved by IRB for this quality improvement project which did not involve participation of patients.
Trial registration
This was not a randomized clinical trial so not applicable.