
Abstract
Objective:
This study investigates the influence of personal characteristics and health-related variables on the care dependency status among elderly in-patients with clinically diagnosed Alzheimer’s disease in two countries.
Methods:
A descriptive cross-cultural survey was administered to a convenience sample of 137 elderly in-patients. Patients were recruited from a hospital in Japan (N = 77) and from a nursing home in the Netherlands (N = 60).
Results:
In both countries, almost all participants are assessed on the severity level of care dependency in the range of “completely care dependent” (Japan: 35.1%; the Netherlands: 20.0%), or “to a great extent care dependent” (Japan: 24.7%; the Netherlands: 45.0%), to “partially care dependent” (Japan: 22.1%; the Netherlands: 21.7%).
Conclusion:
This study demonstrates that there is no interdependence between the severity level of care dependency and personal characteristics of patients with Alzheimer’s disease in both countries. Regarding the interplay of health-related variables on the severity level of care dependency, a difference was found between countries.
Introduction
Many countries in the world have to cope with an aging population. Older adults, aged over 65 years, have an 11% prevalence of Alzheimer’s disease. 1 Dementia due to Alzheimer’s disease is a multifaceted disease that affects all aspects of a patient’s life. Alzheimer’s disease is a progressive neurodegenerative disorder characterized by loss of memory and cognition, declining ability to function in daily life, and changes in personality and behavior.1,2 Functional impairment in Alzheimer’s disease is typically referred to as a disability in everyday functioning that results primarily from cognitive impairment, with notable losses in the ability to perform daily activities. 2 In regard to Alzheimer’s disease, dependence can be defined as the level of assistance required by a patient due to deterioration in cognition, physical functioning, and behavior. 3
The aging of the population in western countries has consequences for health-care facilities. 4 These facilities will be faced with an increasing number of demented people with health problems. The consequences of these health problems affect the daily functioning of the patient due to the loss of physical and mental functions. The risk of functional decline and loss of independence increase during and after admission of patients with dementia to hospital and long-term care facilities. 5
Loss of independence can be perceived in relation to the decrease of self-care abilities and the onset of care dependency. Care dependency means that the self-care abilities of a person in terms of their daily physical and psychosocial human needs (e.g. eating and drinking, hygiene, and social contacts) have decreased to such an extent that the person’s care demands are, to some degree, dependent on professional support. 6 Care dependency is an important correlate of general and disease-specific health status. 7 Impairment in the ability to perform normal daily tasks can lead to patients becoming dependent on caregivers. 8
Besides dependence in self-care, the above-mentioned facilities will also be faced with increasing numbers of demented patients with behavior problems. 4 Indications of behavior problems include psychotic phenomena, such as delusional thinking, suspiciousness, and hallucinations, as well as a number of other behavioral disturbances, including agitation, violence, and verbal outbursts. 9 Many elderly in-patients demonstrate behavior problems. As dementia progresses, insight may be lost and attempts to provide care may cause frustration and anger both for those providing care and for the person affected. The causes of behavioral problems are often multiple and include a combination of loss of abilities, loss of insight, and lack of inhibition. 10 Behavior problems of dementia patients often scare and exhaust both family members and caregivers. 11 Consequently, the management of these behavioral symptoms among patients with Alzheimer’s disease has become a major task for families and professional workers. 12 Therefore, it becomes necessary to understand the behavior problems as well as the needs of patients admitted in hospitals and long-term care facilities in order to plan their optimal care plan.
Many studies have been conducted with the aim to investigate the interplay between behavioral symptoms and interaction of neurobiological, cognitive, and environmental factors.13–19 Studies investigating the interdependence between care dependency and behavioral problems are scarce. To our knowledge, there are no studies assessing the interdependence between the care dependency status and behavioral problems of elderly hospital or nursing home patients. This information can be used by nurses and other health-care professionals to provide better guidance and to design interventions.
It was proposed that personal characteristics, including individual-related (age and gender) and health-related issues, are associated with the care dependency severity level of elderly in-patients. This assumption was tested in two countries—Japan and the Netherlands—with the aim to investigate the interplay of personal characteristics on the care dependency status among elderly in-patients with clinically diagnosed Alzheimer’s disease, within and between both countries. Research questions addressed in this study were as follows: (1) What are the personal characteristics of the patients? (2) What scores on care dependency and behavioral problems do patients have between and within each country? and (3) How are personal characteristics related to the severity level of care dependency? The choice for both countries arose from an existing research cooperation of the authors in the field of care dependency, respectively, with patients admitted in a hospital (Japan) and in a nursing home (the Netherlands).
Methods
Design
A descriptive cross-cultural survey was administered to a convenience sample of 137 elderly in-patients. Patients were recruited from a hospital in Japan (N = 77) and from a nursing home in the Netherlands (N = 60). Data were collected from August 2012 to June 2013. The long period of data collection in terms of the small number of participants has to do with the (low) number of admissions during the research period in both countries.
Participants and procedure
Patients had to fulfill the following selection criteria for inclusion into the study: patients with an age older than 60 and—to be able to compare patients from both countries with each other—with a Mini-Mental State Examination (MMSE) score less than 25 out of 30.
After obtaining informed consent from the patient or his or her legal representative, data collection took place in two ways. First, a research assistant reviewed the patient record for patients characteristics including age and gender. From the patient record, information about the MMSE score, use of glasses and hearing aid, pressure ulcer, fall, and the clinical diagnosis as reason for admission was obtained. Second, a research assistant interviewed nurses who were familiar with the patients to rate them on the severity level of care dependency, the Care Dependency Scale (CDS), and the Behavioral Pathology in Alzheimer’s Disease Rating Scale (BEHAVE-AD).
Data collection
Severity level of care dependency
The severity level of care dependency was used to identify eligible groups of respondents for this study. This one-item scale identifies five levels of progressive dependency, from level 1 = “completely dependent on care” from others to level 5 = “almost independent.” This one-item scale is short, simple, and user-friendly and suitable for use in this study to identify the severity level of patient’s care dependency. 20
Cognitive impairment
The MMSE was used to obtain comparable groups from both countries by measuring their cognitive impairment. The MMSE was introduced as a brief screening method for assessing the mental status of patients with psychiatric disorders. 21 Later, the MMSE was also recommended as a screening test for a global impression of cognitive functioning in the routine clinical examination of elderly patients. Cognitive function was measured with the 30-item version of the Mini Mental State Examination (MMSE-30). Any score greater than or equal to 25 points (out of 30) indicates a normal cognition. Below this, scores can indicate severe (≤9 points), moderate (10–18 points), or mild (19–24 points) cognitive impairment. 22
CDS
The CDS provides a framework for assessing the care dependency status of institutionalized patients on 15 daily human needs: eating and drinking, continence, body posture, mobility, day or night pattern, getting dressed and undressed, body temperature, hygiene, avoidance of danger, communication, contact with others, sense of rules and values, daily activities, recreational activities, and learning ability. The instrument consists of these 15 items, each one of which has an item description and five care dependency criteria. Nurses rate all items by selecting one criterion out of the five. Low scores on the items indicate that patients are completely dependent on care. However, high scores mean that patients are almost independent of care. From the CDS, development and psychometric testing has been described in several studies.23–27 Besides these studies, the psychometric properties of the CDS were determined using datasets from Canada, Italy, Norway, and the Netherlands; 28 Finland, Spain, and the United Kingdom; 29 and Germany, 30 Japan, 31 and Poland. 32
BEHAVE-AD
The BEHAVE-AD is the most widely used instrument for the evaluation of dementia-related behavioral changes. 33 It addresses the following seven categories: delusions, hallucinations, activity disturbances, aggressiveness, diurnal rhythm disturbances, affective disturbances, and anxieties and phobias. Each item is rated on a 4-point severity scale ranging from 0 (indicates absence of a symptom) to 3 (indicates a symptom which is severely manifest (e.g. with an emotional and physical component). Rating is carried out by a clinician interviewing the patient’s spouse and/or caregiver and inquiring whether or not the behavior has occurred within the past few weeks. 11 Administration time is about 20 min. Summary descriptions of the methodology for scoring the BEHAVE-AD have been published. 34
Ethical considerations
In the Netherlands, the patients or their legal representative were orally informed about the purpose of the study. In Japan, the patients or their legal representative were informed using the documents about the purpose of the study. They were told that participation was voluntary, and that a questionnaire should be completed by a nurse most involved in their daily care. Those who volunteered to participate and signed an informed consent form were included in the final sample. To ensure confidentiality and anonymity, the names of the participants were encoded, and data analysis did not allow individual patients to be identified. In the Netherlands, permission regarding the research was given in 2012 by the Regional Medical Ethical Committee in Leeuwarden. In Japan, permission was obtained from the research ethics committee of HamamatsuUniversity. This study was performed under the principles outlined in the Declaration of Helsinki.
Statistical analysis
Descriptive statistics were performed and expressed as mean ± standard deviation. The Mann–Whitney U test was used to compare the means of item variables for patients at study entry between both countries because the variables were ordinal and not normally distributed. Furthermore, differences among the three severity levels of care dependency were calculated with Kruskal–Wallis test. In addition, post hoc test (Bonferroni) was performed for correcting for multiple comparisons to verify the difference between the severity levels of care dependency.
A bivariate correlation analysis (Spearman’s ρ) was performed between personal characteristics, health-related variables, and the severity level of care dependency. The statistical threshold for significance was set at p < 0.05. SPSS-19.0 for Windows (SPSS, Chicago, IL) was used for all statistical analyses.
Results
Personal characteristics
As seen in Table 1, participants in Japan had a mean age of 86.7 years. Although the Dutch sample was significantly younger (age of 83.1 years), the participants in both countries were primarily female, 58.4% for Japan and 53.3% for the Netherlands. The reason for hospital admission in Japan was the diseases of the respiratory system (22.1%), diseases of the nervous system (20.8%), and diseases of the circulatory system (19.5%). In the Netherlands, the most important reason for admission in the nursing home was mental and behavioral disorders (71.7%). Unlike Japanese participants (39.0%), most of the Dutch participants use glasses (76.7%), whereas an opposite image can be seen in the use of a hearing aid: 67.5% Japanese participants versus 16.7% Dutch participants. Gradually, more pressure ulcers have been measured in the Dutch sample (15.0%) than in the Japanese sample (9.1%). More fall incidents have been found in the Japanese sample (24.7%) than in the Dutch sample (16.7%).
Results of individual-related and health-related variables (N = 137).

ICD-10: International Classification of Diseases-10; SD: standard deviation; BEHAVE-AD: Behavioral Pathology in Alzheimer’s Disease Rating Scale; NS: nonsignificant.
Care dependency and behavioral problems
Because of the small numbers in the Japanese and Dutch sample levels “to a limited care dependent” and “almost independent,” we combined both levels with the level “partially care dependent” and analyzed three severity levels: “complete care dependent,” “to a great extent care dependent,” and “partially care dependent.” Mann–Whitney U test revealed no significant difference on the CDS sum score between both countries. Furthermore, on each severity level, there are only a few items that show a significant difference between Japanese and Dutch item score. With regard to the mutual relationship between the three severity levels of care dependency, we see no significant differences between both countries on the following BEHAVE-AD categories: affective disturbance and anxieties and phobias.
Regarding the differences on severity level of care dependency within both countries, Kruskal–Wallis tests reveal for both countries significant differences in the mean scores for the 15 CDS items and in the mean CDS sum score between the three severity levels of care dependency. Furthermore, the mean total BEHAVE-AD scores and mean scores for the seven BEHAVE-AD categories for each of the three severity levels are shown in Table 3. Bonferroni correction has been used to determine which means of the three severity levels differ from each other. Post hoc comparison shows important differences between the three severity levels of care dependency for most of the 15 CDS items and CDS sum score. From the following CDS items in the Japanese sample (mobility, avoidance of danger, recreational activities, and learning ability) and in the Dutch sample (hygiene, avoidance of danger, sense of rules and values, daily activities, and learning ability), the means between the severity levels “complete care dependent” and “to a great extent care dependent” do not vary. Regarding the BEHAVE-AD scores, post hoc comparison (Bonferroni) indicates no important differences between the three severity levels of care dependency for BEHAVE-AD categories and sum scores in the Dutch sample. For the results in the Japanese sample, see Table 3.
Severity level of care dependency
As shown in Table 4, in Japan, the severity of care dependency has a significant but weak relationship with the number of ICD-10 diagnostic categories, use of glasses, pressure ulcer, fall, activity disturbances, and BEHAVE-AD sum score. Moderate relationship was found with use of hearing aid, aggressiveness, and diurnal rhythm disturbances. For both countries, the severity level of care dependency was very strongly related to CDS sum score.
Discussion
The aim of this study was to investigate the interaction of personal characteristics and health-related variables on the care dependency status among elderly in-patients with clinically diagnosed probable Alzheimer’s disease in Japan and the Netherlands. The main findings are that there is hardly a difference in having daily human needs among patients with Alzheimer’s disease between both countries. However, behavior problems show an opposite image.
Personal characteristics
The descriptive outcomes reveal a significant difference regarding the CDS item body posture and mobility. On both items, the Japanese participants are “to a greater extent care dependent,” whereas the Dutch participants can be described as “partially care dependent.” The possible course, as an explanation for this difference, can be found in the higher number of Japanese patients with the admission diagnosis “diseases of the musculoskeletal system” and the higher percentage fall incidents: 24.7% versus 16.7% as found in the Dutch sample.
The mean score on the severity level of care dependency shows no significant difference between both samples. In both countries, almost all participants are assessed on the severity level of care dependency in the range of “completely care dependent” (Japan: 35.1%; the Netherlands: 20.0%), or “to a great extent care dependent” (Japan: 24.7%; the Netherlands: 45.0%), to “partially care dependent” (Japan: 22.1%; the Netherlands: 21.7%). With the exception of the CDS items eating and drinking, body posture, and mobility, all other CDS item scores and mean sum score revealed no significant difference between Japanese and Dutch participants.
Except for the category anxieties and phobias, Mann–Whitney U test shows a significant difference in the mean score on the BEHAVE-AD categories and sum score between both countries. Another notable difference between both countries can be found with regard to the mean score on the BEHAVE-AD categories and sum score. With the exception of the category diurnal rhythm disturbances, the Japanese participants had a lower score than found in the Dutch sample. This means that the Japanese participants have little or few behavioral problems. The explanation for this may be found in the fact that the Japanese sample is mainly characterized by somatic diagnosis what justifies admission in a hospital, while the Dutch sample is characterized by a high percentage (71.7%) of mental and behavioral disorders, which in many cases is the reason for admission in a nursing home.
Care dependency and behavioral problems
As Table 2 shows, on each severity level, there are only a few items that show a significant difference between Japanese and Dutch CDS item score. There appears to be a tendency for daily human needs in a relatively stage-specific sequence in patient’s severity level of care dependency. It can be concluded that as the severity level of care dependency increases from 3 to 1, the number of CDS items with a significant difference on the item score decreases, and patients in both countries have almost the same daily human needs regarding nursing care and support in fulfilling these needs. Furthermore, identification of these stage-specific aspects is relevant for nurses and other health-care professionals to design interventions and to provide better care.
CDS andBEHAVE-AD mean scores (±SD) between both countries per severity level of care dependency (Mann–Whitney U test).

CDS: Care Dependency Scale; SD: standard deviation; BEHAVE-AD: Behavioral Pathology in Alzheimer’s Disease Rating Scale; NS: nonsignificant.
Regarding the BEHAVE-AD categories, it can be seen that as the severity level of care dependency increases from partially to complete care dependent, the scores on almost all BEHAVE-AD categories, with the exception of category hallucination (level 1) and diurnal rhythm disturbances (level 2), reveal no significant difference between both countries. With regard to the mutual relationship between the three severity levels of care dependency, we see no significant differences between both countries on the following BEHAVE-AD categories: affective disturbance and anxieties and phobias in relation to the severity level of care dependency. Furthermore, the findings suggest that when the severity level of care dependency increases from partially to complete care dependent, the differences between both countries disappear regarding the prevalence of problem behavior.
This study proposed that personal health-related issues as daily human needs and behavior problems are associated with the care dependency severity level of elderly in-patients. Unlike the differences between both countries, we also analyzed the differences within each country. The results, as shown in Table 3, indicate that in both countries, there is a significant difference on each of the three severity levels with regard to the 15 CDS mean item scores and CDS sum score. This means that an increase in dependency on others in fulfilling daily human needs is accompanied by a change in the severity level of care dependency from “partially care dependent” to “complete care dependent.”
CDS andBEHAVE-AD mean scores (±SD) within each country per severity level of care dependency (Kruskal–Wallis).

CDS: Care Dependency Scale; SD: standard deviation; BEHAVE-AD: Behavioral Pathology in Alzheimer’s Disease Rating Scale; NS: nonsignificant; 1 = complete care dependent; 2 = to a great extent care dependent; 3 = partially care dependent.
Bonferroni post hoc test:
1 versus 2: these groups do not vary; 1 versus 3: these groups vary; 2 versus 3: these groups vary.
1 versus 2: these groups vary; 1 versus 3: these groups do not vary; 2 versus 3: these groups vary.
1 versus 2: these groups do not vary; 1 versus 3: these groups do not vary; 2 versus 3: these groups vary.
1 versus 2: these groups do not vary; 1 versus 3: these groups vary; 2 versus 3: these groups do not vary.
It is apparent from Table 3 that the severity level 1 “complete care dependent” and 3 “partially care dependent” had a lower mean severity scores on six (Japan) or five (the Netherlands) of the seven BEHAVE-AD categories and the mean total BEHAVE-AD score than did severity level 2 “to a great extent care dependent.” Examination of Table 3 indicates that across the three severity levels of care dependency, wide variations in the perceived intensity of these symptoms are reported by care professionals. This curvilinear relation has also been demonstrated 11 between the total score on the BEHAVE-AD and global severity of dementia as measured with the Global Deterioration Scale. 35 Furthermore, Kruskal–Wallis tests reveal no significant differences in the mean scores for the seven BEHAVE-AD categories and in the mean total BEHAVE-AD score between the three severity levels of care dependency for the Netherlands. For Japan, Kruskal–Wallis tests show no significant differences in the mean scores for the following three BEHAVE-AD categories: hallucinations, affective disturbances, and anxieties and phobias. This means that in both countries, the prevalence of these behavioral problems remains stable despite an increase in the severity of the patient’s care dependency. For the Japanese sample, it is also noteworthy that aggressiveness is the only behavior that decreases constantly as care dependency increases.
Severity level of care dependency
The results, as described in Table 4, indicate that there is no statistical consistency between the severity level of care dependency and personal characteristics in both countries. This was in accordance with other studies. 26 From the health-related variables, only the daily human needs as measured with the CDS revealed in both countries a very strong correlation. 26 Another remarkable difference between both countries is the difference in significant correlations between the other health-related variables and the severity level of care dependency. While in the Netherlands, no significant correlations are found, variables such as diagnostic categories, use of glasses, use of hearing aid, pressure ulcer, fall during last 30 days, and some BEHAVE-AD measurements are of significant influence on the severity level of care dependency among Japanese patients with Alzheimer’s disease. A possible explanation may be that, in contrast to the Dutch sample, most of the Japanese patients were characterized by somatic-related diagnosis.
Spearman’s correlation matrix of personal characteristics, health-related variables, and severity level of care dependency.
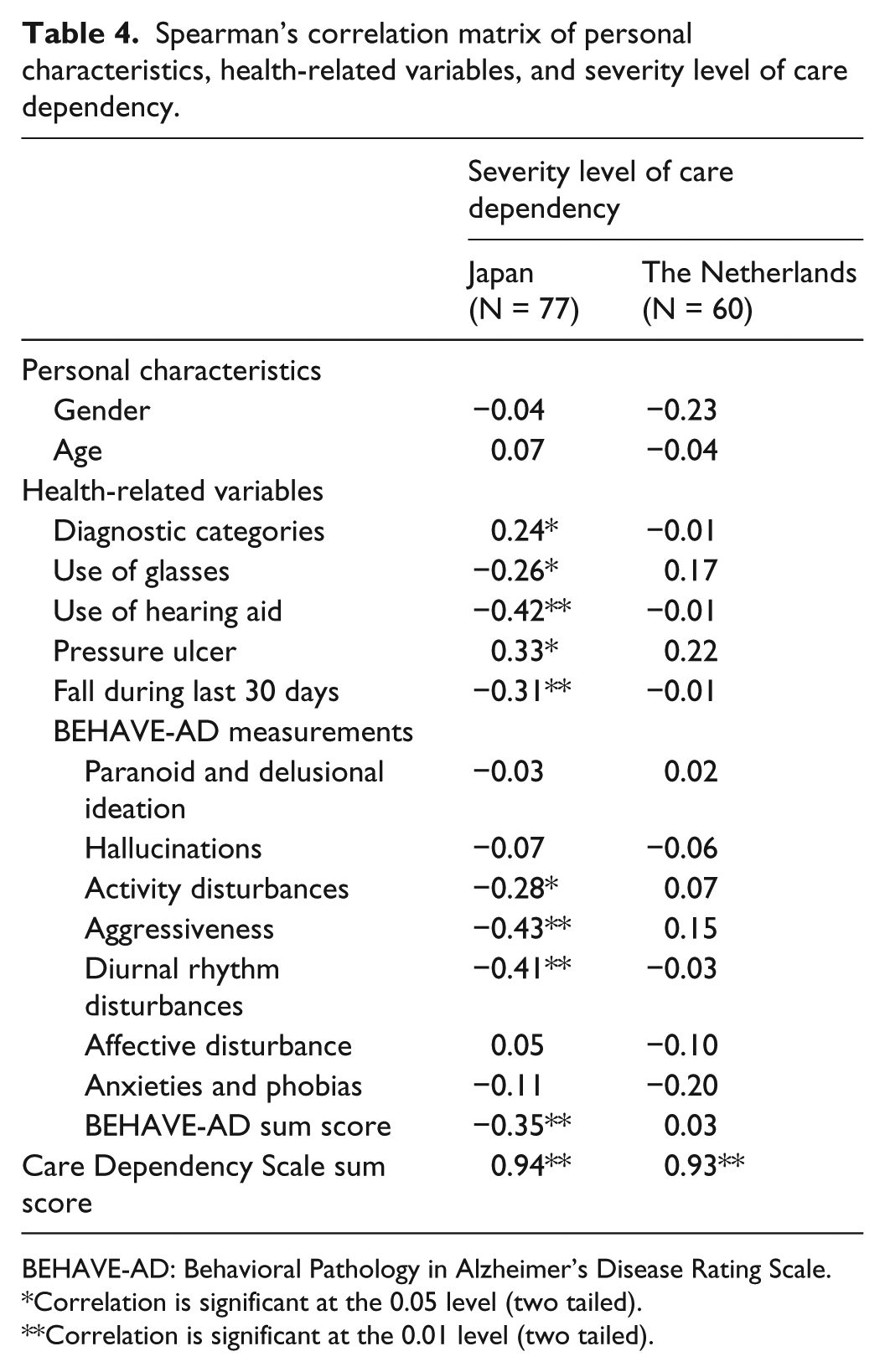
BEHAVE-AD: Behavioral Pathology in Alzheimer’s Disease Rating Scale.
Correlation is significant at the 0.05 level (two tailed).
Correlation is significant at the 0.01 level (two tailed).
Study limitations and implications
The results of this study must be interpreted within the context of the following limitations. Limitations include the use of a small convenience sample of patients with Alzheimer’s disease, the cross-cultural design used to obtain data from two countries, and the lack of measures about the institutional and cultural context between both countries. Sample characteristics also show a significant difference on age and disease (one physical-oriented and one mental-oriented patient populations). Furthermore, it is unknown whether the severity of care dependency precedes behavioral problems or is in response to existing behavioral problems. Although these limitations make it difficult to compare both patient populations, based on corresponding MMSE profiles and using the framework of daily human needs, there is a need to create two similar groups.
Therefore, additional research with a longitudinal design is required for a better understanding of the relationship between severity of care dependency and behavioral symptoms. For further studies, it is also recommended to obtain more similar sample groups and to add hospital and nursing home characteristics, additional health-related variables, and mode of care as factors for investigation.
Conclusion
Despite its limitations, this is the first study assessing the interdependence between the care dependency status and behavioral problems of elderly hospital or nursing home patients. This study demonstrates that there is no interdependence between the severity level of care dependency and personal characteristics of patients with Alzheimer’s disease in both countries. Regarding the interplay of health-related variables on the severity level of care dependency, a difference in interdependence was found between both countries.
Caring for patients with Alzheimer’s disease with dementia-associated problems is challenging for caregivers who starts with a thorough assessment to gather data for planning successful interventions. Questionnaires such as CDS and BEHAVE-AD may help nurses and other health-care professionals to get insight into the factors for influencing the onset and reducing care dependency and behavioral symptoms.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest in this work with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.