
Abstract
Objective:
The primary aim of this secondary analysis was to determine whether cardiac autonomic neuropathy independently predicted adverse cardiac outcomes in asymptomatic individuals with type 2 diabetes. Additional aims include the determination of the correlation of standard autonomic testing measures and power spectral analysis of heart rate variability, and the association of diabetes-related and cardiac risk factors with cardiac autonomic neuropathy measures.
Methods:
Cardiac autonomic neuropathy was assessed at the study entry into the Detection of Ischemia in Asymptomatic Diabetics study, using autonomic heart rate and blood pressure testing, and power spectral analysis of heart rate variability. All participants were prospectively followed for the composite clinical outcome of cardiac death, acute coronary syndromes, heart failure, or coronary revascularization.
Results:
Over 5 years of follow-up, 94 of 1119 (8.4%) subjects developed symptomatic cardiac disease. In unadjusted bivariate analyses, abnormalities in several cardiac autonomic neuropathy tests, including lower Valsalva and Standing Heart Rate Ratios, higher resting Heart Rate, greater systolic blood pressure decrease on standing, and lower low-frequency power, were predictive of symptomatic disease. Independent predictors of poor cardiac outcome were a lower Valsalva Heart Rate Ratio, non-Black ethnicity, longer diabetes duration, higher glycated hemoglobin (HbA1c), insulin use, reported numbness in the extremities, higher pulse pressure, family history of coronary artery disease, and higher waist-to-hip ratio. Clinical factors independently associated with a lower Valsalva Heart Rate Ratio were insulin use, clinical proteinuria, higher pulse pressure, use of angiotensin-converting enzyme inhibitor and non-Black ethnicity.
Conclusion:
Cardiac autonomic neuropathy predicted adverse cardiac outcomes in asymptomatic type 2 diabetes without known cardiac disease. Clinical variables may help to identify patients who might have cardiac autonomic neuropathy and warrant consideration for autonomic testing.
Introduction
Despite advances in contemporary therapy and lower mortality rates from cardiovascular disease (CVD), individuals with type 2 diabetes mellitus (DM) continue to have almost twice the risk developing CVD. 1 Coronary artery disease (CAD) is often silent and only detected at an advanced stage, sometimes with sudden cardiac death as the first manifestation. 2 In spite of this apparent hazard for individuals with diabetes, recent findings in the Detection of Ischemia in Asymptomatic Diabetics (DIAD) study indicated that routine screening is not justified in the absence of cardiac symptoms. 3 All individuals with type 2 diabetes should receive aggressive, multifactorial CAD risk factor modification and careful surveillance for symptomatic cardiac disease. However, this goal is not consistently achieved in clinical practice. 4 Thus, improved identification of high-risk patients might provide both providers and patients with additional motivation to achieve treatment goals.
The DIAD study was primarily designed to assess the predictive value of screening for inducible ischemia in asymptomatic individuals on the subsequent development of serious events, including myocardial infarction (MI) and cardiac death. 5 The results demonstrated a 22% prevalence of inducible myocardial ischemia with stress myocardial perfusion imaging (MPI). 5 The presence of cardiac autonomic neuropathy (CAN) was not only associated with MPI abnormalities, but was also a significant predictor of DIAD’s primary outcome, MI and cardiac death at 5 years.3,6 However, the limited number of these events precluded multivariate assessment of any independent impact of CAN. The relationship of CAN and other prognostic factors to a wider array of symptomatic cardiac events, including acute coronary syndrome, heart failure, or coronary revascularization in the DIAD cohort, has not been explored previously. These latter events were compiled as secondary outcomes because they have significant impact on patients with type 2 diabetes. In terms of predictive models, they also increase the number of outcome events and the power of the analysis to identify predictors of clinically important adverse cardiac outcomes.
Previous studies support the association between CAN and future adverse cardiac events.3,7–15 In these studies, the prevalence of CAN and its association with CAD events varied widely, due in part to differences in patient characteristics, type of diabetes, and inclusion of those with known CAD. Different methodologies used to diagnose CAN, variances in cut points defining an abnormal response, and whether one or more abnormal tests were required may have contributed not only to the wide range of estimates in prevalence of CAN, but also to its association with CAD events.
Most previous studies that have analyzed CAN as a predictor of risk in asymptomatic patients with diabetes have used standard autonomic testing based on the heart rate (HR) or blood pressure (BP) response to various maneuvers, including Valsalva, deep breathing, handgrip or standing. Alternate methods of assessing autonomic balance, based on frequency and time domain analysis of heart rate variability (HRV), have been useful in predicting outcome in CVD.12,16–20 Heightened sympathetic and reduced parasympathetic tone have been correlated with low-frequency (LF) and high-frequency (HF) power, respectively, in individuals with diabetes.7,17,19,21 However, few previous studies have assessed whether HRV analysis is predictive of adverse cardiac outcomes in asymptomatic individuals with diabetes.22,23
The primary objective of this secondary analysis was to determine whether CAN independently predicted adverse cardiac outcomes in asymptomatic individuals with type 2 diabetes. As the relationship between the various measures of cardiac autonomic dysfunction in individuals with type 2 diabetes is poorly understood, additional aims explored the correlation of standard autonomic testing measures and power spectral analysis of HRV, as well as the association of diabetes-related and cardiac risk factors with CAN measures.
Methods
Study procedures, including Institutional Review Board (IRB) approval, have been described in detail in previous publications. 5 The DIAD study recruited patients from diabetes and primary care practices at 14 centers throughout the United States and Canada between 2000 and 2002. Inclusion criteria were (1) type 2 diabetes, with onset at or after the age of 30 years and no history of ketoacidosis and (2) age 50–75 years. Exclusion criteria were (1) angina pectoris or equivalent symptoms; (2) stress test or coronary angiography during the 3 years prior to entry into the study; (3) history of MI, heart failure, or coronary revascularization; (4) electrocardiographic (ECG) evidence of Q-wave MI, significant ischemic ST segment or T-wave changes, or complete left bundle branch block; (5) any clinical indication for stress testing; (6) active bronchospasm precluding the use of adenosine for imaging; (7) pregnancy; and (8) severe co-morbidity, such as malignancy, affecting short-term life expectancy.
At enrollment, a resting 12-lead ECG was recorded and blood and urine samples were obtained for laboratory testing. Recent fundoscopy reports by an eye care professional were evaluated for the presence and stage of diabetic retinopathy. Medical history and physical examination were performed. Subjects were tested for diabetic neuropathy (monofilament and vibration sensation and reflex testing). All participants were followed by telephone contact every 6 months for 5 years to assess the development of cardiac events—cardiac death, acute coronary syndromes, heart failure, and revascularization—which were subsequently adjudicated after review of the medical records. 3 If more than one event occurred in a subject, the time of the first event was considered in the analysis. DIAD subjects (n = 1123) were randomized to either undergo MPI (n = 521) or follow-up only (n = 522). Of these, four did not complete the first 6 months of follow-up and so were excluded from the present analysis.
Cardiac autonomic testing
Cardiac autonomic function was assessed using both standard HR- and BP-based tests 24 and power spectral analysis of HRV. All subjects had fasted overnight and had not taken any medications. After a 10-min period of rest, a standardized autonomic testing protocol was administered to all participants. Prior to CAN testing, three supine BP readings were obtained 1 min apart, and these were averaged to establish baseline systolic and diastolic BP values and resting arterial pulse pressures. The Valsalva maneuver was considered contra-indicated in patients with proliferative retinopathy or recent eye surgery (n = 40). In addition, 90 tapes were completely unreadable.
In the first 699 DIAD participants, three HR-based tests were assessed using standardized, non-automated methodology: (1) HR changes during deep breathing (HR-DB) at a rate of six breaths per minute performed for 5 min; the first minute of deep breathing was used in the HR-DB analysis, with the expiratory–inspiratory difference in beats, as well as the ratio, averaged over the six cycles; (2) Valsalva HR Ratio: the Valsalva maneuver was executed by having the subject perform forced expiration at 40 mmHg for 15 s. The ratio of maximal HR during the Valsalva and the lowest HR immediately after the maneuver was calculated. Two maneuvers were performed and the readings averaged; and (3) Standing HR Ratio: the ratio of HR (longest and shortest R-R intervals) at approximately the 15th and 30th beat after standing up from a recumbent position. Data from these three tests were analyzed from a Marquette Holter monitor system (GE Healthcare, Waukasha, WI). Absence of markers on the tapes indicating the start and end of a maneuver did not allow for analysis of all three tests in all subjects. Valsalva HR Ratio readings were available in 571 (82%) and Standing HR Ratio in 625 (89%). In order to have a consistent method, we obtained HR-DB and the ratio HR-DB data from Holter recordings in all subjects; usable data were available in 929 (83%) of subjects.
In the subsequent subjects (after 1 October 2001), the automated Anscore Health Management System® (Boston Medical Technologies, Wakefield, MA) was used, which provides verification that adequate tidal volume and ventilatory rate have been achieved during 1 min of deep breathing and that adequate pressure is maintained during the Valsalva. 25 Assessment of HR-DB, using the Holter system, was also assessed during timed deep breathing over 5 min with verbal cues in these 420 subjects, and these data were used in addition to Anscore® data. For HR-DB, Anscore® data only yielded a ratio and not the absolute difference in beats between respiratory cycles. Anscore®-based ratios of HR-DB readings were obtained in 308 (73%), Valsalva HR Ratio in 256 (61%), and Standing HR Ratio in 382 (91%). The discrepancy in yield between the two methods was likely the result of the rigorous quality control safeguards imposed by the Anscore® system. Overall, Valsalva HR Ratio by either Holter or Anscore® method was available in 827 (74%) and Standing HR Ratio in 1007 (90%).
Resting HR was obtained from Holter tapes during 10 min of rest prior to the CAN testing in all subjects. Standing (BP-STD) and handgrip (BP-HG) BP readings were obtained in all subjects. For the BP-STD, the BP was taken immediately upon standing up from a recumbent position. Data were available in 1113 (99%) subjects. Subjects rested for 5 min prior to the BP-HG test, with three sitting BP recordings taken prior to the sustained handgrip maneuver. These results were averaged to compare with the diastolic blood pressure (DBP) during HG. Each subject was asked to maximally squeeze the handgrip dynamometer; 30% of this amount was calculated and subjects were instructed to maintain this level for as long as possible up to 5 min. BP-HG readings were obtained at 1-min intervals during the handgrip. If systolic blood pressure (SBP) rose to > 210 mmHg or DBP > 110 mmHg, testing was stopped for safety reasons. BP-HG data were available in 979 (87%) subjects.
Power spectral analysis of HRV during 10 min of rest was obtained from Marquette Holter monitor tapes. All tapes were visually scanned by a trained technician for editing and overwriting, including verification of labeling of QRS complexes and ectopic beats. Using a GE MARS utility workstation, the Marquette HRV Tool software was used to obtain LF power, HF power, and the LF:HF power ratio readings. Data for LF (0.04–0.15 Hz) and HF (0.15–0.40 Hz) power were obtained in amplitude (ms2) and the LF:HF ratio calculated; all power spectral analysis data were log transformed due to their skewed nature in the data analysis; ms2 values are shown in tables. Power spectral analysis data were available for 795 (71%) subjects.
Statistical analysis
CAN data were double entered at the DIAD Core Center at Yale University School of Medicine via Statistical Analysis System (SAS) INSIGHT (Cary, NC). Anscore® data were merged with CAN and other DIAD data. All analyses were conducted using SAS (Version 9.3). CAN results were analyzed either using their exact value or using the lowest quartile cut point for the three HR-based measures. All continuous variables were assessed for a departure from linear trend, and categorized into quartiles, with an additional level added for missing values, for example, when the acquisition of cardiac autonomic function data was incomplete due to inability of the patient to perform the test, contraindication to Valsalva because of the presence of proliferative retinopathy, or technically inadequate recordings. Bivariate analyses, using chi-square and t-tests, were used to identify potential predictors of CAD events. After testing the proportionality assumption, Cox proportional hazards regression analysis was then utilized to determine hazard ratios (HRs) in relation to cardiac events. Hazard ratios were calculated comparing those individuals in the lowest quartile for HR-based autonomic tests and for the highest quartile for pulse pressure, which we considered as being abnormal, to all other subjects, including those with missing data since risk was not elevated in any of these other categories. Spearman correlation coefficients (rs) or t-tests (data not shown) were used to determine the association of CAN measures with one another and with type 2 diabetes-related (duration, treatment, control and microvascular complications) and CAD risk factors. Moderate relationships were considered with rs > 0.40. Preliminary bivariate analyses using t-tests and chi-square analyses were used to assess the association of being in the lowest quartile of Valsalva (<1.37 with the Anscore Health Management System® and <1.17 with Holter), as this was found to be an independent predictor of having a CAD event, and type 2 diabetes-related and CAD risk factors. This was followed by multivariate logistic modeling. A backward selection strategy was used for both Cox and logistic modeling, including all variables identified in the bivariate analysis with a p ⩽ .10, adjusting for potentially confounding factors and assessing for possible interactions. The association of sociodemographic characteristics (age, sex, ethnicity, income, level of education, and marital status) was assessed in all analyses and only reported where significant.
Results
Predictors of cardiac events
Clinical characteristics, results of cardiac autonomic function testing, and symptomatic cardiac events in 1119 DIAD patients are shown in Table 1. Over a mean 4.8 years of follow-up, there were 94 secondary outcome events (acute coronary syndrome, heart failure, coronary revascularization) and 32 primary outcome events (MI and cardiac death). As several subjects had more than one event, the actual total number of subjects with an event was 94, for an overall event rate of 8.4%. Bivariate comparisons in patients without and with the development of symptomatic CAD for the primary and secondary combined events are shown in Table 2. Several factors were identified, including those related to diabetes control, retinopathy, neuropathy, and autonomic dysfunction.
Patient characteristics (n = 1119).
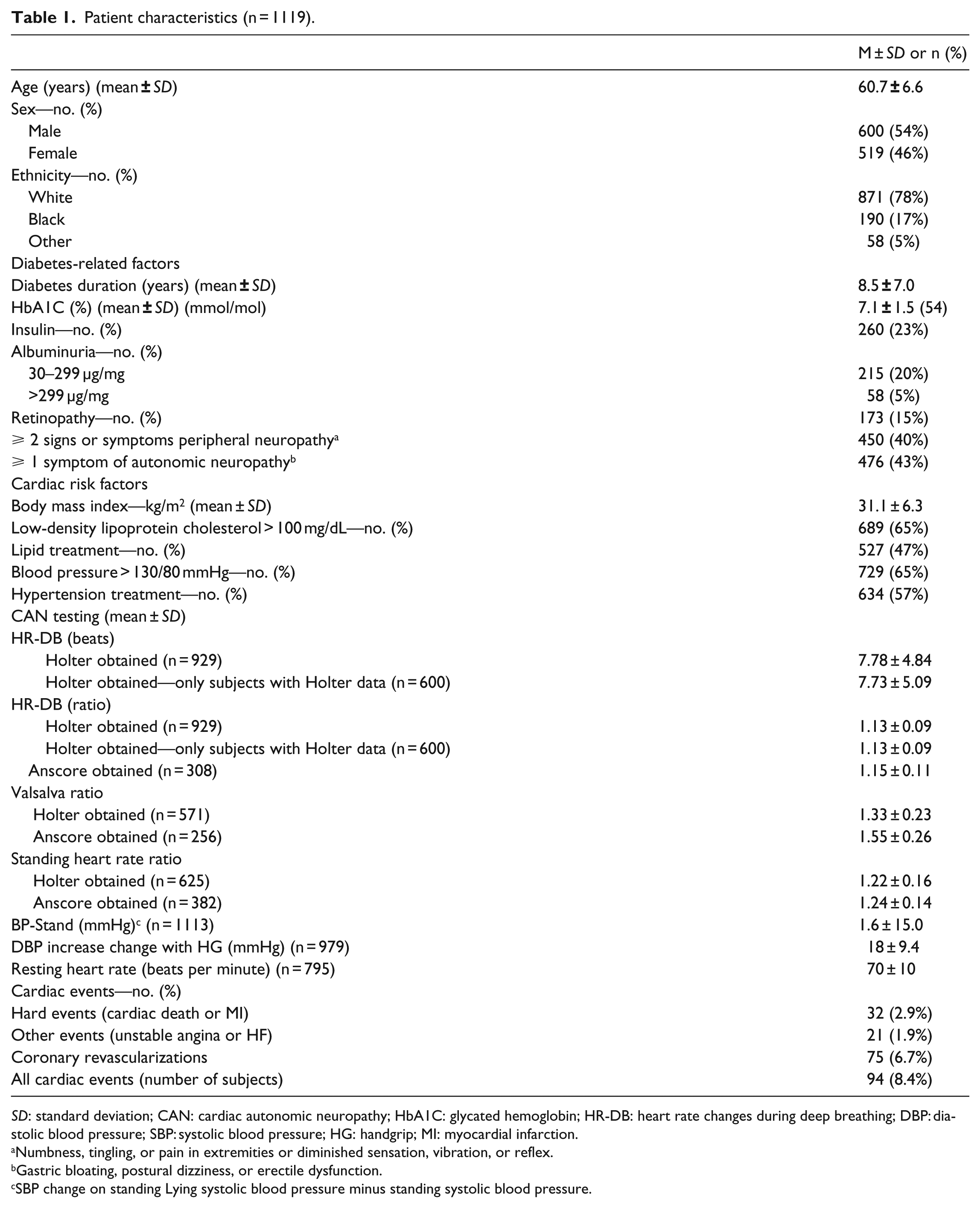
SD: standard deviation; CAN: cardiac autonomic neuropathy; HbA1C: glycated hemoglobin; HR-DB: heart rate changes during deep breathing; DBP: diastolic blood pressure; SBP: systolic blood pressure; HG: handgrip; MI: myocardial infarction.
Numbness, tingling, or pain in extremities or diminished sensation, vibration, or reflex.
Gastric bloating, postural dizziness, or erectile dysfunction.
SBP change on standing Lying systolic blood pressure minus standing systolic blood pressure.
Factors associated with CAD events (n = 1119).

CAN: cardiac autonomic neuropathy; HbA1C: glycated hemoglobin; HR-DB: heart rate changes during deep breathing; CAD: coronary artery disease; DBP: diastolic blood pressure; SBP: systolic blood pressure.
Numbness, tingling or pain in extremities; diminished sensation, vibration or reflex.
Gastric bloating, postural dizziness, or erectile dysfunction.
Lowest quartile of Valsalva is ⩽1.37 with Anscore or 1.17 with Holter.
Lowest quartile of Standing heart rate is ⩽ 1.14 with Anscore or 1.11 with Holter.
SBP change on standing. Lying systolic blood pressure minus standing systolic blood pressure.
In unadjusted bivariate analyses in relation to cardiac events (Table 2) lower Valsalva (p = .0005) and Standing (p < .0001) HR Ratios, higher resting HR (p = .02), a greater SBP decrease on standing (p = .007) and lower LF power (p = .009) were associated with a CAD event. In multivariate Cox proportional hazards regression analysis, adjusting for other important prognostic and potentially confounding factors, the CAN measure that remained an independent predictor of events at 5 years was the lowest quartile of Valsalva HR Ratio (HR = 1.60; 95% confidence interval (CI) = 1.02, 2.50; p = .04).
Other predictors of events were, patient report of numbness in the extremities (HR = 1.98; 95% CI = 1.31, 3.00; p = .0012); non-Black ethnicity (HR = 2.41; 95% CI = 1.12, 5.21; p = .02); duration of type 2 diabetes (HR = 1.07 per year; 95% CI = 1.04, 1.10; p < .0001); HbA1c (HR = 1.26 per 1% increase; 95% CI = 1.10, 1.44; p = .0006); insulin use (HR = 0.53; 95% CI = 0.31, 0.91; p = .02); highest quartile (⩾ 60.3 mmHg) of arterial pulse pressure (HR = 2.11; 95% CI = 1.37, 3.24; p = .0006); family history of CAD (HR = 1.66; 95% CI = 1.04, 2.64; p = .03); and an increasing waist-to-hip ratio (HR = 1.04 per .01 increase; 95% CI = 1.01, 1.07; p = .0034).
Inter-relationship of CAN measures
The HR-DB obtained via Holter method was moderately associated with Valsalva HR Ratio (Holter rs = .43; p < .0001; n = 560; Anscore® rs = .29; p < .0001; n = 219) and the Standing HR Ratio (Holter rs = .34; p < .0001; n = 610; Anscore® rs = .28’ p < .0001; n = 313). The Standing HR Ratio obtained by Holter was moderately correlated with the Valsalva HR Ratio (Holter rs = .47; p < .0001; n = 557; Anscore® rs = .27; p < .0001; n = 249). The two BP-based tests were only weakly (rs = −.09; p = .005; n = 978) associated with one another. The Valsalva HR Ratio obtained by the Holter method was weakly correlated with the BP response to standing (rs = −.19; p < .0001; n = 569). In addition, the Standing HR Ratio was weakly associated with BP response to standing (Holter rs = −.27; p < .0001; n = 24; Anscore® rs = −.15; p = .004; n = 381) and BP-HG (Holter rs = .17; p = .0001; n = 521; Anscore® rs = .23; p < .0001; n = 359).
For the power spectral HRV analysis, LF and HF power were moderately–strongly correlated both with one another (rs = .74, p < .0001, n = 795) and with the three HR-based tests (rs = .28–.54; p < .0001) as measured by either the Holter or Anscore® methods, while only weakly correlated with BP-HG (LF rs = .14; p = .0002; n = 712; HF rs = .13; p = .0007; n = 712). The LF:HF ratio was weakly–moderately correlated with LF (rs = .25; p < .0001; n = 795) and HF (rs = −.41; p < .0001; n = 795) power, but only weakly correlated with the Standing HR Ratio (Anscore® rs = .12; p = .03; n = 296) and the Valsalva HR Ratio (Holter rs = .17; p = .0004; n = 439). The resting HR was weakly associated with Valsalva HR Ratio (Holter rs = −.12; p = .01; n = 439; Anscore® rs = −.13; p = .05; n = 208), the Standing HR Ratio (Holter rs = −.34; p < .0001; n = 489; Anscore® rs = −.31; p < .0001; n = 296), BP-HG (rs = −.18; p < .0001; n = 712), and LF:HF (rs = .14; p = .0001; n = 795), but moderately correlated with LF (rs = −.47; p < .0001; n = 795) and HF (rs = −.53; p < .0001; n = 795) power. Overall, the Standing HR Ratio was the measure most consistently associated with HR- and BP-based measures, as well as with measures of power spectral analysis of HRV.
Predictors of CAN
In assessing the association of CAN measures with potential risk factors, SBP, arterial pulse pressure, and duration of type 2 diabetes demonstrated the strongest and most consistent relationships across all measures of CAN (Table 3). Higher HbA1c and triglyceride levels were weakly associated with lower power spectral analysis of HRV levels and higher resting HR. Measures of adiposity were also weakly associated with power spectral analysis of HRV measures, but not with HR- or BP-based tests.
Correlations (rs) and associated p values between measures of autonomic function and diabetes-related and CAD risk factors.

CAD: coronary artery disease; BMI: body mass index; BP-HG: change in diastolic blood pressure during sustained handgrip; BP-STD: change in systolic blood pressure from lying to standing; HbA1C: glycated hemoglobin; Cr: creatinine; DBP: diastolic blood pressure; HDL: high-density lipoprotein cholesterol; HF: high-frequency power; HR-DB: expiratory-to-inspiratory difference in beats during 1-min timed deep breathing from Anscore®; LDL: low-density lipoprotein cholesterol; LF: lower frequency power; LFHF: ratio of LF:HF power; Stand HR: heart rate response at 30th and 15th beat after standing from Anscore®; BP-STD: SBP change on standing; PP: pulse pressure; SBP: systolic blood pressure; TG: triglycerides; Valsalva: change in heart rate during Valsalva maneuver from Anscore®; WHR: waist-to-hip ratio.
Given that the lowest quartile of Valsalva HR Ratio was the sole CAN measure independently associated with the development of symptomatic cardiac events, independent factors associated with a blunted Valsalva HR Ratio were assessed. Table 4 shows the factors associated with an abnormal Valsalva HR Ratio (i.e. lowest quartile) in bivariate analysis. Several factors related to diabetes, arterial blood pressure, and obesity were identified. However, in multivariate logistic regression, the following were independently associated with the lowest Valsalva HR Ratio quartile: non-Black ethnicity (odds ratio (OR) = 1.90; 95% CI = 1.19, 3.04; p = .007); insulin use (OR = 1.44; 95% CI = 1.01, 2.04; p = .04); clinical proteinuria (OR = 3.32; 95% CI = 1.78, 6.19; p = .0002); increased pulse pressure (OR = 1.02 per 1 mmHg increase; 95% CI = 1.005, 1.03; p = .005); and use of angiotensin-converting enzyme (ACE) inhibitors (OR = 1.45; 95% CI = 1.06, 1.98; p = .02).
Factors associated with the lowest quartile of Valsalva ratio.

SD: standard deviation; HbA1C: glycated hemoglobin; DBP: diastolic blood pressure; HDL: high-density lipoprotein cholesterol; HF: high-frequency power; LDL: low-density lipoprotein cholesterol; LF: lower frequency power; PP: pulse pressure; PVD: peripheral vascular disease; SBP: systolic blood pressure; TG: triglycerides; CAD: coronary artery disease; ACE: angiotensin-converting enzyme; CAN: cardiac autonomic neuropathy; HR-DB: heart rate changes during deep breathing; BP-Stand: SBP change on standing.
Lowest quartile of Valsalva is ⩽1.37 with Anscore or 1.17 with Holter.
Numbness, tingling, or pain in extremities; diminished sensation, vibration, or reflex.
Gastric bloating, postural dizziness, or erectile dysfunction.
Discussion
In the present investigation, we have extended the analysis of the DIAD study to include both the primary (MI and cardiac death) and secondary cardiac events (ACS, heart failure, and coronary revascularization). This more comprehensive analysis increased the number of outcomes from 32 (primary events) to 94 (8% over 5 years) and provided the statistical power to perform multivariate analysis and for the first time to identify potentially important clinical predictors of risk in this population. Although DIAD was conducted from 2000 to 2007, the subjects, as in most randomized trials, were well-controlled and diabetes-related therapies have not changed substantially since this time, thus making the findings relevant today.
Our results confirm the importance of CAN as an independent risk predictor in patients with type 2 diabetes, previously also suggested through assessment of the HR response to adenosine infusion in DIAD subjects randomized to stress testing. 6 The overall results of this analysis highlight specific factors that will help to identify asymptomatic patients with type 2 diabetes, who are more likely to have CAN, placing them at risk for a subsequent symptomatic cardiac event.
CAN has been theorized to play a role in asymptomatic ischemia and silent MI in individuals with DM,8,9,15 although the mechanistic link between the two remains uncertain. However, both CAN and asymptomatic myocardial ischemia have been associated with adverse cardiac outcomes,10,13,14 even in the absence of DM21,23 and was found to be an independent predictor of mortality following MI. 23 However, previous studies examining CAN in individuals with asymptomatic myocardial ischemia have been limited by varying methods to detect disease, widely different inclusion and exclusion criteria, variable risk factors studied, and frequently, small sample size yielding limited study power to perform multivariate analyses. Nevertheless, our rates of cardiac events are similar to the Valensi et al. 7 series (10.3% during 3–7 years of follow-up), in which CAN was found in 39% and inducible ischemia in 31% of their patients. In that study, CAN, as assessed through three HR response measures, was associated with an elevated risk of CVD events (OR = 4.3; 95% CI = 1.1–17.3; p = .04). In contrast, in the Milan Study on Atherosclerosis and Diabetes, CAN assessed by a composite score of HR-DB, Standing HR Ratio, and BP during standing was not associated with cardiac events (occurring in 5.7% of the original cohort). 15 Using a composite score might have contributed to the lack of association in that prior study. In preliminary analysis, we did not find score-based approaches13,26,27 to be associated with either prediction of myocardial perfusion abnormalities or with cardiac outcomes. The common criterion for an abnormal HR-DB response is less than an 11-beat difference between expiration and inspiration, and using this cut point, 67% of DIAD subjects were classified as having an abnormal response, and thereby influenced a score-based approach. Use of actual, individual values allowed us to more precisely identify the specific test abnormality associated with adverse outcomes.
Power spectral analysis of HRV has been used in several large population-based studies.22,23 In the Framingham study, all measures of HRV except for the LF:HF ratio were associated with all-cause mortality, with LF demonstrating the strongest relationship to mortality (HR 1.7; 95% CI = 1.37, 2.09). 23 More recently, in Action to Control Cardiovascular Risk in Diabetes (ACCORD), CAN; as assessed through QT interval, the standard deviation of normal R-R intervals (SDNN), and resting HR, along with the presence of peripheral neuropathy; was associated with all-cause and CVD mortality; those subjects with CAN were 1.55–2.14 times more likely to die as compared to those without CAN. 12 Our findings are unique in that previous studies have not included both types of autonomic testing in assessing cardiac events. It is important to note that power spectral analysis of HRV values was low in the DIAD population, reflecting the older age of our subjects with type 2 diabetes, as compared to previous studies. These low-power spectral analyses of HRV values may have limited their ability to predict CAD events in our study.
CAN in the presence of several measures of long-term diabetes control—longer duration, higher HbA1c (controlled for insulin use), and the presence of extremity numbness, a symptom of somatosensory peripheral neuropathy, along with a higher waist-to-hip ratio were all strongly and independently associated with a subsequent cardiac event. The independent predictive value of HbA1C is particularly noteworthy, since DIAD subjects overall had relatively well-controlled diabetes. These findings underscore the importance of the need for long-term control of blood glucose.28–30
Our finding regarding the association of wide arterial pulse pressure with both cardiac events and measures of CAN is particularly important and supports the need for BP control in patients with diabetes. Several recent studies have also demonstrated an independent association between pulse pressure and events.31–35 In subjects with type 1 diabetes in the EURODIAB Prospective Complications study, pulse pressure was a strong risk marker for mortality (HR = 1.33; 95% CI = 1.13–1.58), along with peripheral (HR = 1.88; 95% CI = 1.06, 3.35) and autonomic (HR = 2.4; 95% CI = 1.32, 4.36) neuropathy. 31 It has been hypothesized that autonomic dysfunction may contribute to CVD through its influence on arterial stiffness. 36
Our results show that various HR- and BP-based and power spectral analysis measures were correlated in subjects with type 2 diabetes without symptomatic CAD, consistent with previous investigations.17,23 However, associations between HR-based results and power spectral analysis of HRV have infrequently been reported. HF power reflects parasympathetic tone similar to the three HR-based autonomic tests, consistent with our observation that they were moderately associated. In contrast, BP-based tests are largely reflective of sympathetic tone; a weak association was only found between BP-HG and either LF or HF power. The LF:HF ratio has been postulated to be a crude indicator of sympathovagal balance, but we did not observe a significant association between LF:HF and BP-based autonomic tests. There also has been recent interest in the use of resting HR as a prognostic factor, with faster, fixed HR seemingly an adverse prognostic marker reflective of CAN.37–39 However, resting HR was not independently associated with cardiac outcomes in the present analysis. Furthermore, resting HR was only weakly associated with the Standing HR Ratio and BP-HG, and moderately associated with LF and HF power, as noted by others. 23
Although testing for CAN has been advocated, 8 in reality, cardiac autonomic function testing is not routinely performed in clinical practice. CAN testing may be performed with relatively simple, inexpensive, and widely available tools, that is, ECG monitoring and BP assessment, but the maneuvers require considerable patient participation, as well as examiner skill and time. It is therefore important to identify those individuals who may be at greatest risk of CAN, in order to reserve testing for selected individuals. Despite methodological differences, consistent with our findings, in prior cross-sectional analyses, CAN was associated with the following factors: older age;20,40,41 longer diabetes duration;40,41 low high-density lipoprotein levels; 42 higher SBP or DBP or hypertension; 42 elevated urinary albumin excretion;41,42 and the presence of retinopathy, nephropathy, macrovascular disease or peripheral neuropathy.40,43 Unlike previous studies, we did not find a strong association with higher HbA1c,40,43 body mass index (BMI),41,44 triglycerides, 42 or with female sex; 42 however, multivariate analyses have not been widely conducted.
The study has several limitations, particularly regarding measurement of CAN. The higher yield of usable test results in the Holter group likely resulted from few tests being deemed unacceptably performed by the study co-ordinators supervising the testing. While all co-ordinators were instructed in proper performance, a strict protocol was followed during testing, and ongoing assessment was made of adequacy of the Holter recordings by the Yale team, it may have been difficult for co-ordinators to assure adequate subject performance. However, any tapes that had missing markers denoting the start and finish of a specific test or were that deemed questionable were not included in the analysis. The built-in controls of the automated Anscore® system would not provide a test result if specific criteria were not met. In addition, differences in the subjects themselves may have contributed to the differences between the two methods. Subjects who underwent Holter testing were more likely to have had a history of hypertension (p = .0002), a family history of CAD (p = .04), smoke (p = .01), be on a beta-blocker (p = .004), have clinical proteinuria (p < .0001), and have a longer duration of diabetes (p = .0002); they were less likely to have signs of peripheral neuropathy—tingling (p < .0001) or pain (p = .04). Although some of these factors may have contributed to differences observed between the two methods, most of these factors were controlled for in the multivariate analysis.
The decision to utilize the automated Anscore® system mid-way through the study resulted in large differences in the Valsalva HR Ratio as compared to those readings obtained without the system, thus requiring use of quartiles in the analysis. The use of quartiles accounted for the differences between the two methods and provides some guidance in clinical practice where automated testing is still not widely used. The low number of cardiac events precluded analysis stratified by type of autonomic testing used. While the use of quartiles allowed us to control for the testing differences, the amount of missing data, although similar to that in other studies due to challenges of autonomic testing, is another concern. The missing data were likely missing at random, the result of poor quality recordings, as well as inability to perform the maneuver. Subjects with missing data did not have an elevated risk of a cardiac event and so this category was combined with the other three quartiles and compared to those in the lowest quartile in the analysis. The Standing HR Ratio was similar when comparing the automated and non-automated methods, as was the ratio during HR-DB. Most of the previous work with autonomic function testing has not utilized automated measures, making it difficult not only to compare values in our population, but raises concerns regarding the precision of non-automated testing in general.
Additional study limitations include the use of short, 10-min recordings for assessment of HRV, rather than 24-h recordings. Assessing 24-h recordings for power spectral analysis of HRV has not been routinely used in large, clinical studies. However, as this method does not rely on active patient participation, it may provide a more feasible means to identify individuals with CAN. Further study is needed.
Individuals at high risk of CAN, as well as of adverse CAD events, may be readily identified from routinely collected clinical data. All providers caring for individuals with type 2 diabetes need to recognize the importance of both CAN and asymptomatic cardiac disease. Screening for both peripheral and autonomic neuropathy, along with assessing arterial pulse pressure, may identify a higher risk group of patients who might be candidates for more intensive CAD risk factor reduction.
Footnotes
Acknowledgements
Participating Investigators: DIAD Investigators Group.
DIAD Study Principal Investigator and Chair: Frans JTh Wackers, MD (School of Medicine, Yale University, New Haven, CT, USA).
Co-Principal Investigators: Lawrence H Young, MD, Silvio E Inzucchi, MD (School of Medicine, Yale University, New Haven, CT, USA), Deborah A Chyun, RN, MSN, PhD (School of Nursing, New York University, New York, NY, USA)
Study Co-ordinator: Janice A Davey, MSN, APRN (School of Medicine, Yale University, New Haven, CT, USA)
Clinical Centers:
University of Montreal: Raymond Taillefer, MD; Sylvain Prévost, MD; Carole Benjamin, CNMT; Andre Gagnon CNMT.
MedStar Research Institute: Robert Ratner, MD; Maureen Passaro, MD; Evelyn Robinson, RN; Amy Smith.
Hartford Hospital: Gary V. Heller, MD, PhD; Deborah Katten, RN, MPH.
Tulane University: Vivian Fonseca, MD, Richard Campeau, MD, Rhonda Fontenot, RN; Sunil Asnani, MD.
University of Alabama: Ami E. Iskandrian, MD; Fernando Ovalle, MD; Mary Beth Hall, RN; Misty Collins, RN.
University of Virginia: Eugene Barrett, MD, George Beller, MD; Wendie Price, RN; Denny Watson, PhD.
Soundview Research Associates: Samuel Engel, MD; Mindy Sotsky, MD; Stella Carolan, RN, Angela Martin, APRN.
University of Rochester: Steven Wittlin, MD, Ronald Schwartz, MD; Mary Kelly, RN.
University of North Carolina: Elisabeth Fasy, MD; Jean Dostou, MD; Leigh Gosnell, RD; Joe Largay, PA-C, Michelle Duclos, MPH; John Buse, MD, Steven Falen, MD.
Midwest Cardiology Research Foundation: Dennis Calnon, MD; Connie Zimmerman, ARRT.
Maine Cardiology Associates: Mylan Cohen, MD; Jennifer Powers, RN.
Cardiology Consultants: Neil Filipchuk, MD; Marie Small, RN; Melina Krulc, RN.
Kansas City Cardiology: Timothy Blackburn, MD; Eric Hockstad, MD; Terry Plesser, RN.
Yale University Radionuclide Core Laboratory and Data Coordinating Center: Donna Natale, CNMT, Roberta O’Brien.
Advisory Board and Data Safety and Monitoring Board: Barry L. Zaret, MD; Robert S. Sherwin, MD; Ralph I. Horwitz, MD.
Trial Registration ClinicalTrials.gov identifier: NCT00769275.
Authors’ contributions
Drs Chyun, Young, Wackers, and Inzucchi had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Drs Wackers, Young, Chyun, Inzucchi, and Zaret contributed to the concept and design of the study. The DIAD Investigators were involved in the recruitment of patients and acquisition of data. Drs Chyun, Wackers, and Young carried out the analysis and interpretation of data. Drafting of the manuscript was done by Drs Chyun, Young, and Wackers. Drs Wackers, Young, Chyun, Heller, Iskandrian, Inzucchi, and Ms Davey contributed to the critical revision of the manuscript for important intellectual content. Statistical analysis was done by Dr Chyun. Adjudication of cardiac events was carried out by Drs Young, Wackers, and Chyun, and adjudication of stroke events was carried out by Dr Karen Furie. Dr Wackers, Ms Davey, and Ms Natale provided administrative, technical, or material support. Study supervision was done by Dr Wackers and Ms Davey. Deborah A Chyun is the guarantor of the study.
Declaration of conflicting interests
DIAD is an investigator-initiated study. The industrial sponsors had no role in the design or conduct of the study, in the collection, analysis or interpretation of data, or in the preparation of the manuscript.
Funding
This work was performed with the support of the General Clinical Research Centers at Yale University (National Institutes of Health M01-RR-00125), University of Rochester (NIH 5M01-RR-00847), and Tulane University (NIH 6M01-RR-05096). The DIAD was supported by grants from Bristol Myers-Squibb Medical Imaging (North Billerica, Massachusetts, USA) and Astellas Pharma (Deerfield, Michigan, USA), who also provided Technetium-99m Sestamibi (Cardiolite®) and Adenosine (Adenoscan®) for study patients.