
Abstract
The incidence of developing a skin cancer is increasing in the UK. The vast majority of skin cancers occur on the head and neck, linked to the increased exposure to ultraviolet light from the sun. Dental healthcare practitioners are expert at examining the head and neck, although anecdotal evidence suggests a lack of confidence in screening for and in managing skin lesions. This article briefly describes the epidemiology, key features and management of various skin lesions, in addition to practical steps general dentists can take to screen for skin cancer. It also describes the various presentations of skin cancer, including in darker skin tones, and how dentists can manage such patients.
Learning Objectives
To improve dental healthcare practitioners’ assessment and management of head and neck skin cancer
To take a thorough “skin-focused” history
To perform a head and neck skin cancer assessment
To recognise red flags of cutaneous pathology
To refer suspicious lesions appropriately
Introduction
Dental healthcare practitioners (DHPs) hold a unique role in the modern healthcare setting – for the average adult, they are the most frequently encountered healthcare professional with visits every three to 24 months. This, along with being experts in examining the oral cavity, means that dentists, dental hygienists and therapists are crucial in screening for oral cancer. Many initiatives and programmes have been set up to improve oral cancer screening during routine dental examinations whereas skin cancer screening is rarely promoted, and anecdotal experience suggests few dentists regularly examine the skin. In addition, DHPs are often unsure about how to manage their findings appropriately and where to refer patients. This article aims to briefly introduce the most commonly occurring malignant and benign skin lesions that DHPs are most likely to encounter and their management in addition to the role of the DHP.
Background
Skin lesions may be broadly categorised as malignant or benign. Malignant lesions are classified as melanoma skin cancer (MSC) and non-melanoma skin cancer (NMSC), although many subtypes and variants exist. This distinction between MSC and NMSC occurs due to the difference in treatment strategies between these groups: non-melanomatous lesions are predominantly best treated with local anaesthetic surgery, while melanoma may require multi-modality treatments including immunotherapy.
In the UK, the lifetime risk of developing a MSC or NMSC is 2.5% and 20% respectively with increasing incidence over the last few decades likely linked to increased exposure to ultraviolet (UV) and sun radiation, changes in clothing styles, ozone depletion, and an ageing population (Table 1).1-3
Risk factors for developing skin cancers
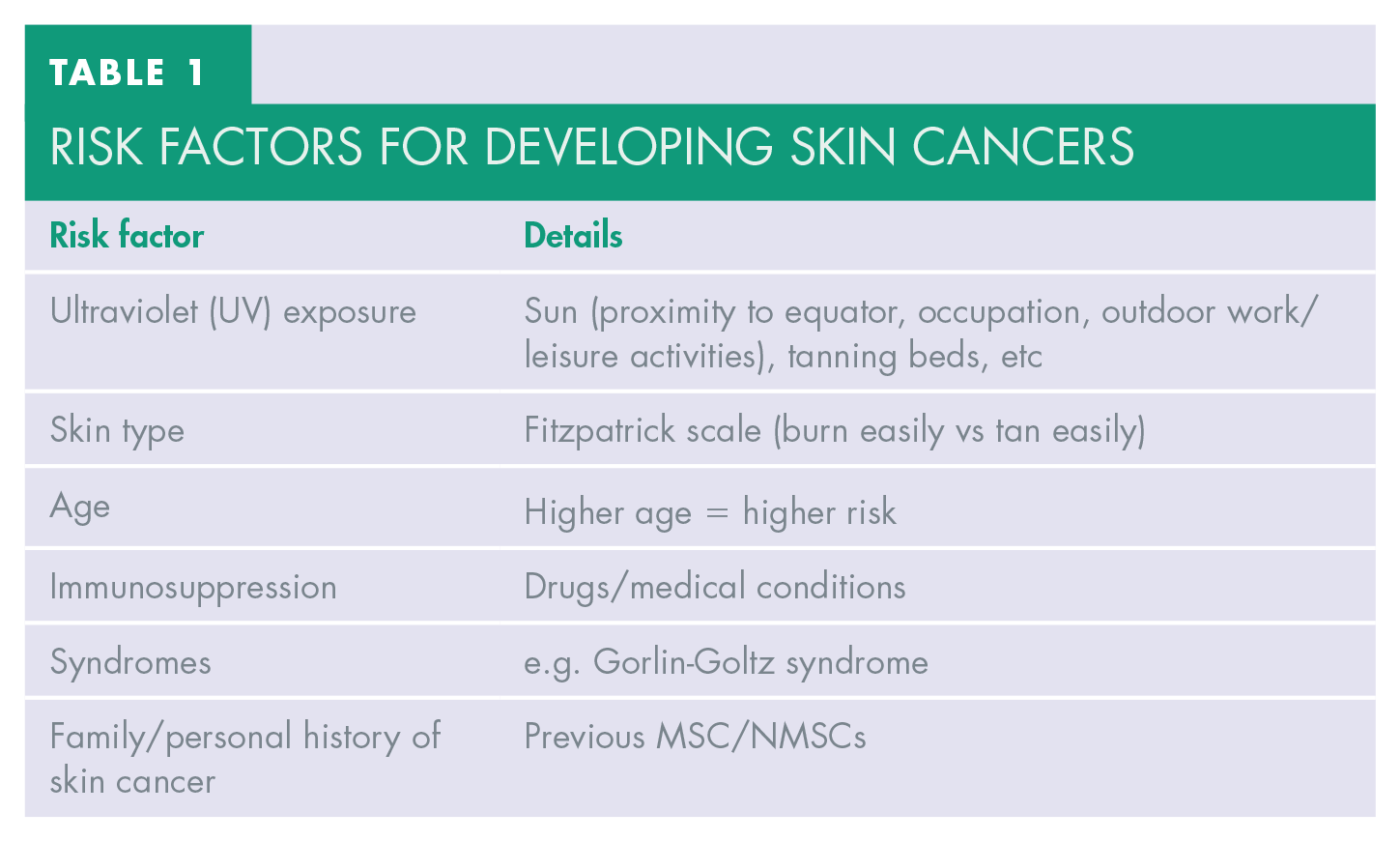
UV light, mainly of solar origin, is the greatest risk factor for the development of skin cancer in most individuals. This is affected by various aspects including geographic location, occupation, clothing choices, hobbies, and use of tannings beds. Individuals with lighter skin are at greater risk owing to lower concentrations of radioprotective melanin in the skin. The Fitzpatrick scale is a well-recognised tool which measures skin colour, tanning, and burning risk. Individuals with type I skin are at greater risk than those with type VI skin. 4 Age and immunosuppression due to medical or iatrogenic causes, i.e. use of immunosuppressive drugs or corticosteroids, are also risk factors. Syndromic causes are less common; however Gorlin Goltz syndrome is well documented for causing recurrent basal cell carcinomas. 3
Skin Cancers
Basal cell carcinoma (BCC)
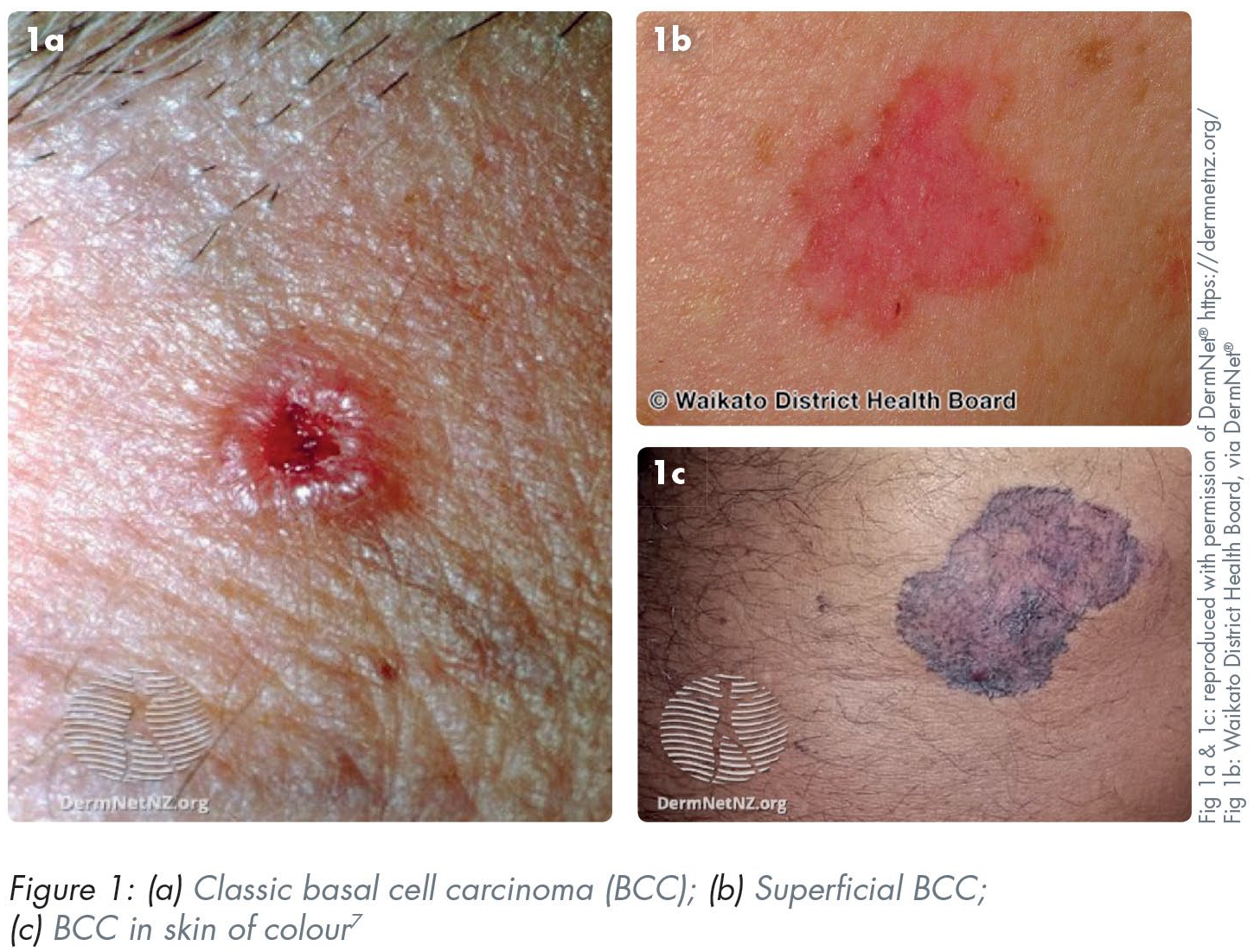
Basal cell carcinomas (BCCs) are the most common type of NMSC characterised by slow growth, local destruction, and very low metastatic potential. They arise from mutations of basal cells within the epidermis. The vast majority (85%) occur in the head and neck region meaning general dental practitioners (GDPs) will inevitably encounter them in patients attending for routine oral health screening. 5 Various BCC subtypes exist (e.g. nodular, superficial, sclerosing, and pigmented), however the most common have features including shiny, pink, or skin-coloured papules or nodules with superficial telangiectasia (Figure 1). There may be central ulceration leading to the appearance of a rolled border (“rodent ulcer”). Patients typically describe a non-healing lump or sore which grows slowly and crusts or bleeds repeatedly. 6 Early recognition and subsequent management can reduce morbidity by limiting local invasion and reducing eventual size of resection. BCCs have a risk of recurrence and as such, patients with previous BCCs should be regarded as high risk and a low suspicion threshold for referral should be held.
Squamous cell carcinoma (SCC)
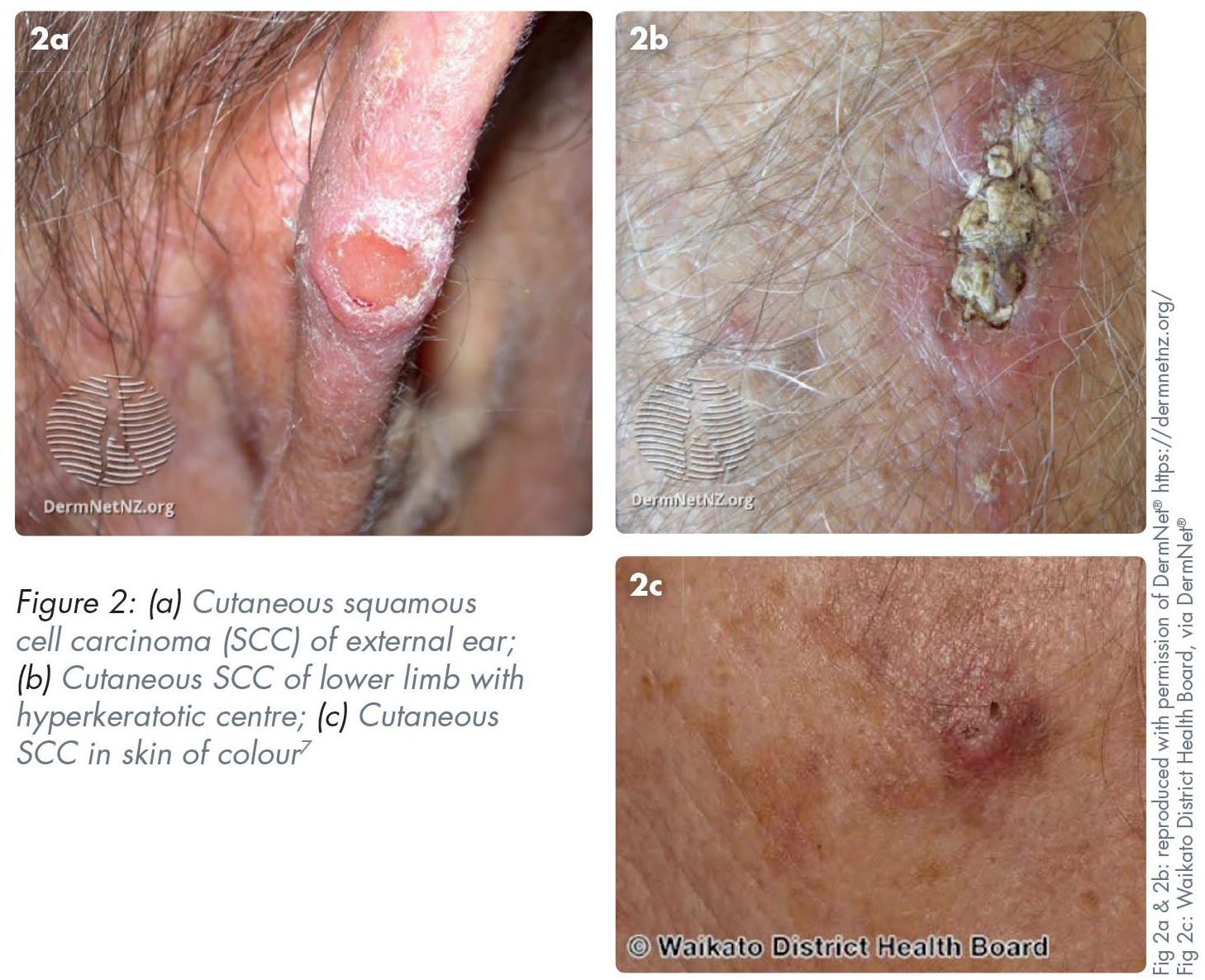
Cutaneous squamous cell carcinomas (cSCCs) are the second most common NMSC. They are more aggressive than BCCs and are characterised by rapid growth and metastatic potential. They arise from mutations of keratinocytes in the spinous layer of the epidermis and adnexal structures such as eccrine glands and pilosebaceous units. Cutaneous SCCs share similar risk factors to BCCs and are typically found on chronically sun-exposed sites such as the head and neck. 8 Cutaneous SCCs behave differently to oral SCCs and have many subtypes, however, this section will focus on invasive cutaneous SCC.
Depending on the morphological subtype, cSCC can present slightly differently; however, a patient may complain of a new lesion that is a non-healing ulcer or wound which bleeds and has grown typically over weeks to months. Clinical features often correlate with the level of differentiation. Well differentiated cSCCs may present as an indurated or firm hyperkeratotic papule, nodule or plaque with or without ulceration (Figure 2). They are typically between 5mm and 15mm in diameter. Poorly differentiated cSCCs can be fleshier with less keratosis. 9 When compared to a BCC, a cSCC can grow rapidly and, as such, prompt referral is key.
Melanoma
Melanomas are potentially life threating cancers which are predominantly cutaneous but can occur on mucosal surfaces. Although relatively rare, the incidence has been increasing in Northern European countries. 10 Exogenous and endogenous stimuli trigger the uncontrolled proliferation of melanocytes in the skin leading to the formation of malignant melanomas. The risk factors for development of malignant melanoma are similar to other skin cancers, such as UV exposure. Interestingly, research suggests that intermittent UV exposure plays a greater role in melanoma development compared to chronic exposure of a single area; the incidence of melanoma is greater in people with intermittent sun exposure (e.g. office workers) compared to those exposed to chronic UV radiation (e.g. farmers). 11 Genetics play a significant role in the development of melanoma with increased risk in patients with a positive family history or those who possess specific genetic syndromes.
Melanomas can be categorised into four different subtypes:
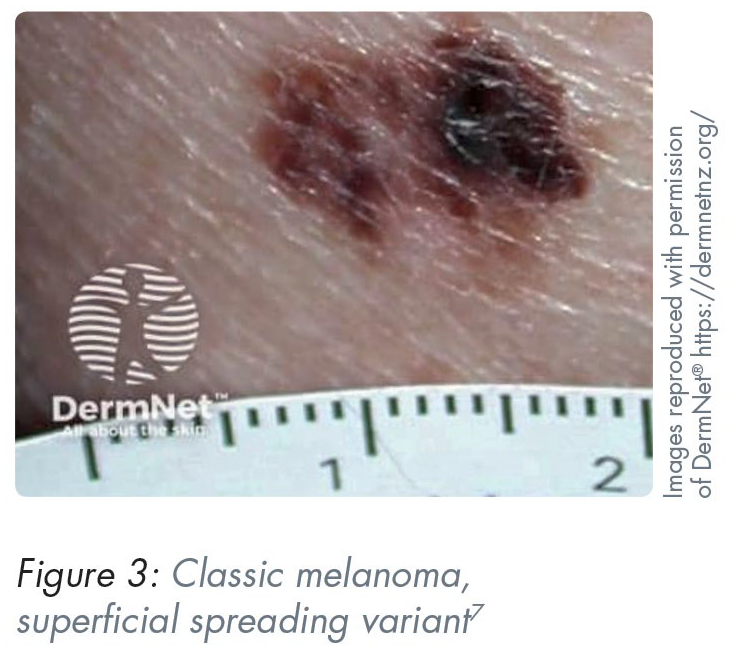
Superficial spreading (most common) – typically presents as a slow-growing flat lesion with heterogenous colour and irregular shape (Figure 3) 7
Lentigo – more common on UV-exposed regions which is why it typically presents as flat macular lesions on the face of older populations
Nodular – presents as a pigmented or amelanotic nodule
Acral – very rarely occur in the head and neck and typically arise from the acral sites such as the palms and soles (Figure 4)
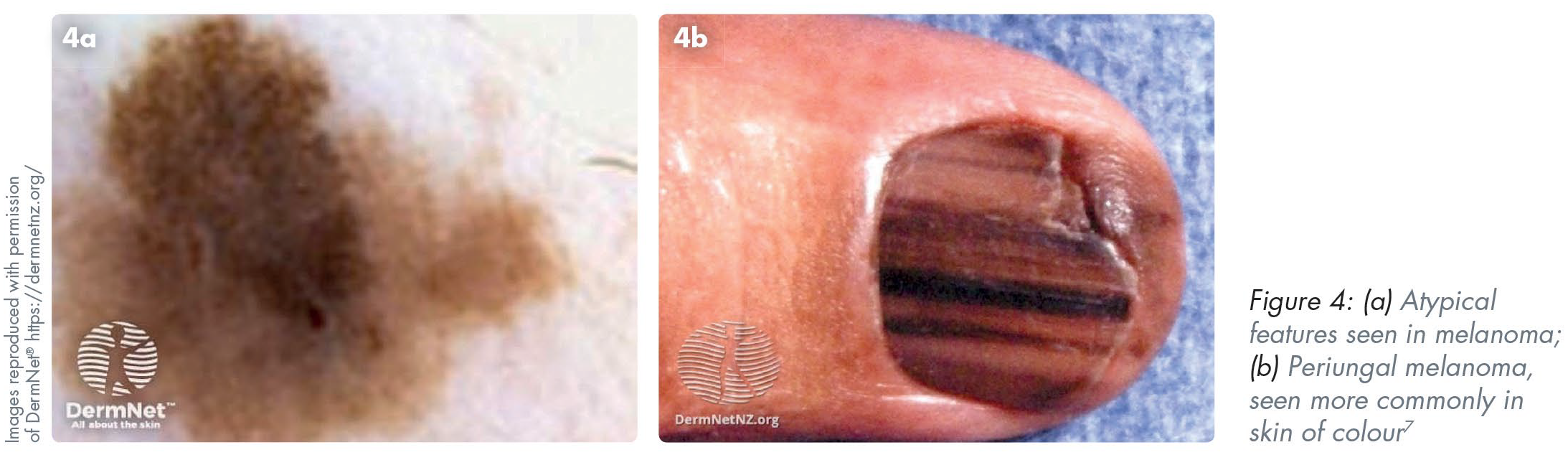
It is important for GDPs to recognise the “red flag” features of pigmented lesions to allow early referral. Despite this, most patients will likely not show any suspicious features of their long-term pigmented lesions (e.g. naevi) and can be reassured. In the UK, once identified, melanomas are typically treated surgically with some patients benefiting from systemic therapy such as immunotherapy or chemotherapy. 12
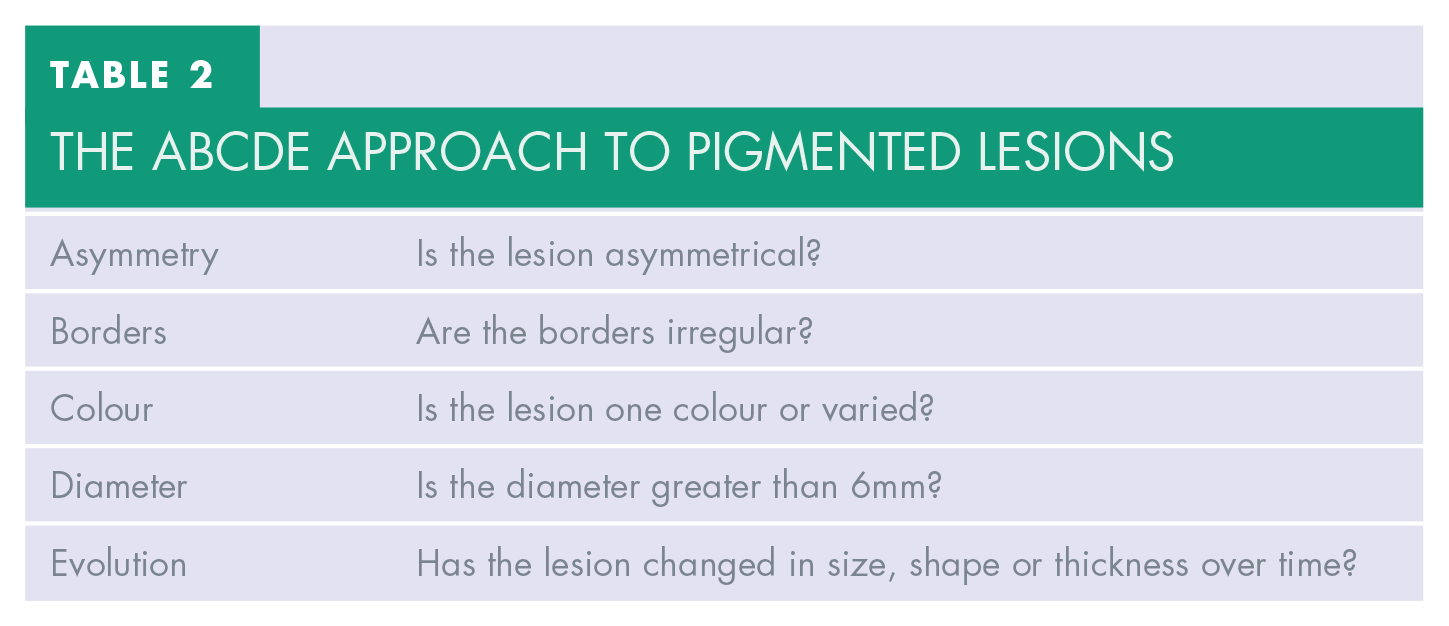
Patients and clinicians would benefit from adopting an ABCDE approach to pigmented lesions, as shown in Table 2.
The ABCDE approach to pigmented lesions
Common skin lesions
Keratoacanthoma
Although these are benign lesions, they can be clinically indistinguishable from cSCC, even to a seasoned dermatologist or skin cancer surgeon. Risk factors include fairer skin, age, and UV exposure. Typical clinical features include a dome-shaped nodule with a central keratin plug producing rolled borders (Figure 5). Any sign of suspicion should lead to an urgent referral as clinical examination alone cannot reliably distinguish between keratoacanthoma and SCCs. Typical management is surgical excision with a wide margin, as for cSCC.

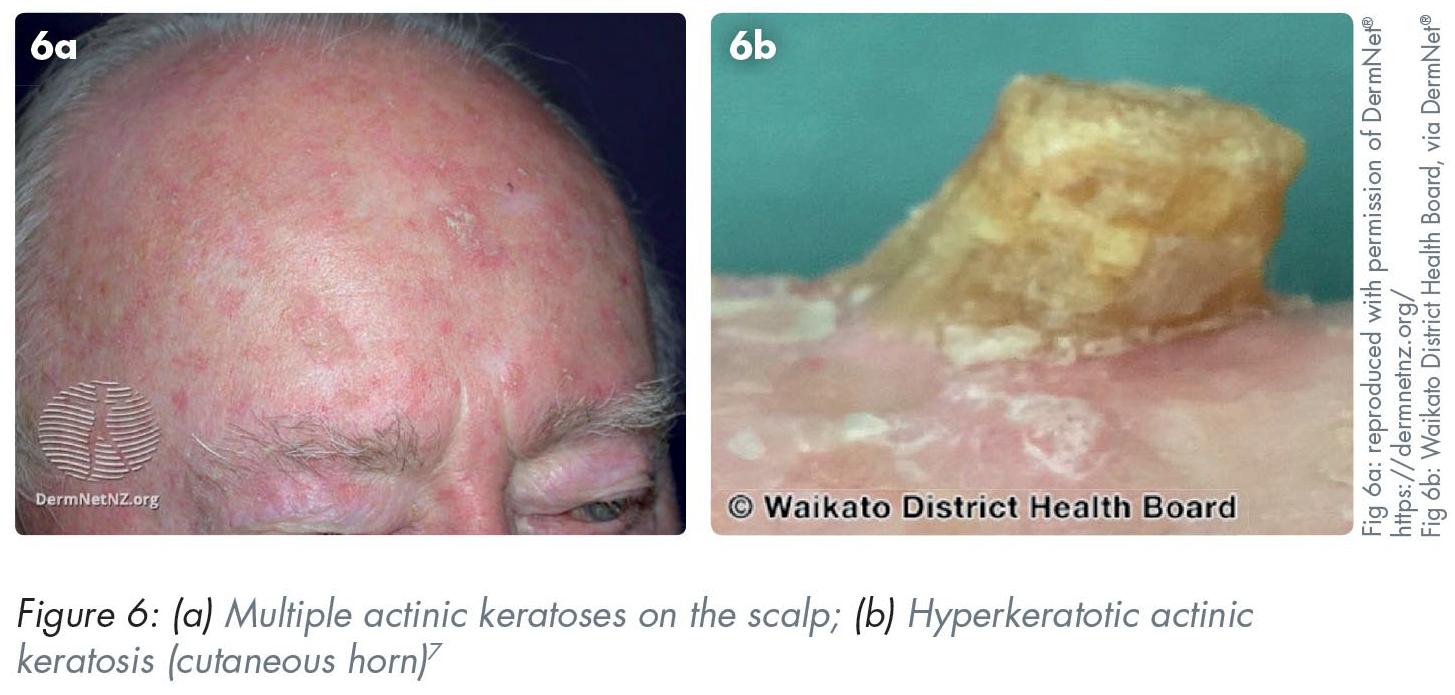
Actinic keratoses
Typically occurring on sun-exposed sites (e.g. face, scalp, and neck), these premalignant lesions may progress into SCC. Patients may complain of a scaly lesion that does not heal. Many subtypes exist including hyperkeratotic, cutaneous horns and actinic cheilitis. They typically present as discrete or confluent macules, patches or plaques of erythema with a scaly or crusting top. They can range in size from 1–2mm papules to large plaques, and many lesions, especially the cutaneous horn subtype, can have a hyperkeratotic horn (Figure 6). 13 Actinic keratoses can be diagnosed based on clinical examination alone, however at times it may be difficult to distinguish the lesion from a cSCC. Management is dependent on the location and number of the lesions, but is treated topically (e.g. cryotherapy, imiquimod cream [Aldara™, 3M Health Care Ltd., Loughborough, UK], 5-fluorouracil [Efudix®, Mylan Products Ltd., Potters Bar, UK], etc.) or if clinical suspicion of cSCC is present, surgically.
Bowen’s disease
Bowen’s disease (SCC in situ) is typically found in sun-exposed regions such as the head and neck. Classically, Bowen’s disease presents as a slow-growing, well-demarcated and erythematous scaly patch. There can be degrees of redness from pink to brighter orange shades. 14 Lesions are usually 10–15mm in diameter and can have hyperkeratotic, scaly features with irregular borders (Figure 7). Lesions are slow growing over months to years, however progression into a cSCC can happen over weeks and months. Patients may complain of a slow-growing, non-healing lesion on a sun-exposed region which has crusted. Around 80–90% of patients will have a solitary lesion.

Due to the slow-growing nature of the lesion, most patients can be treated medically with topical treatments such as cryotherapy or 5-fluorouracil cream. 14 Due to the nature of Bowen’s disease, follow up by a skin specialist is required weeks or months after treatment to assess for resolution of the lesion.
Seborrhoeic keratoses
Seborrhoeic keratoses, often colloquially referred to as “seb Ks”, are common benign skin tumours. They are typically asymptomatic and present as macules, papules or plaques with a tan or black coloured appearance. They are classically “stuck on” to the skin or have a “warty” appearance. They can arise anywhere in the head and neck region and rarely exceed 10mm in diameter (Figure 8). 15 They require no treatment, however are often removed for aesthetic reasons. Options include cryosurgery, shave excision, and curettage.
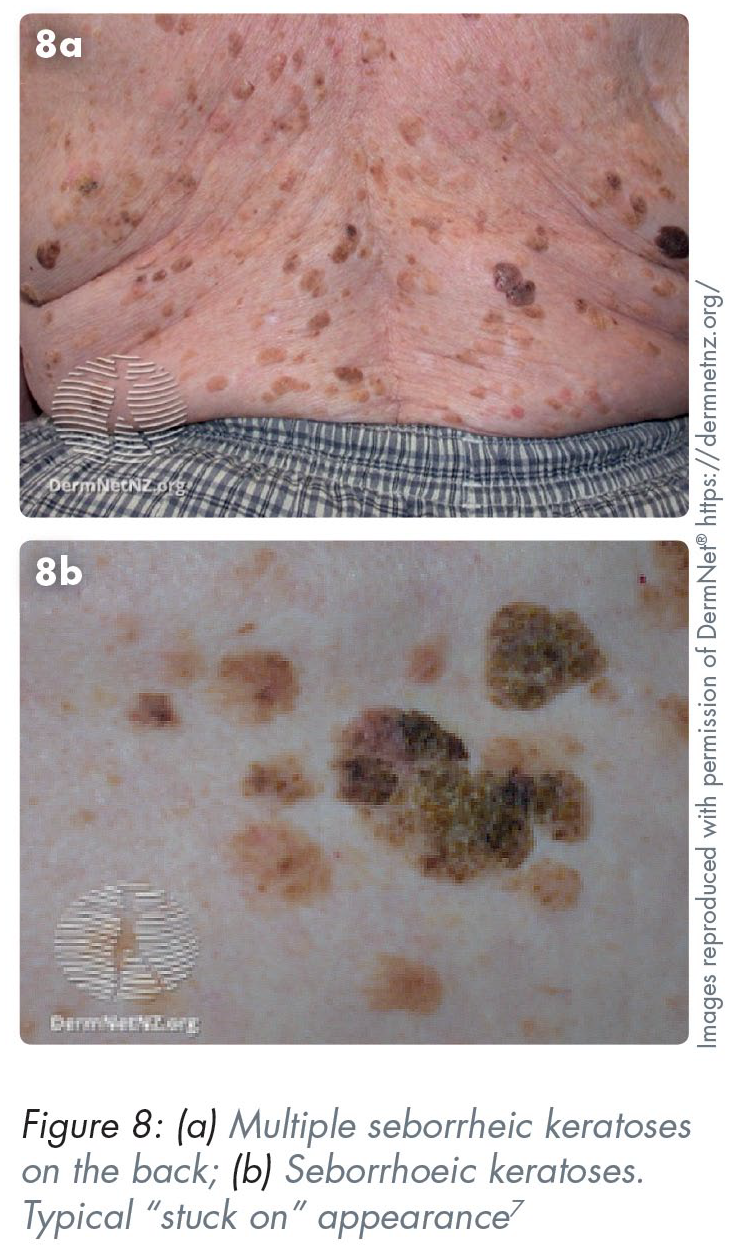
In skin of colour, seborrhoeic keratoses can present as small black or dark brown bumps that can be 1–5mm in diameter, typically seen on the face, neck, chest and upper back. This presentation is also known as dermatosis papulosa nigra with a prevalence of up to 77% in darker skin. 16
Naevi
Often known as “moles”, naevi are local proliferation of melanocytes (pigmented cells). Many are congenital however some develop over time. They are more common in fairer skin types and can occur on any part of the body with varied appearances. As with any pigmented lesion, an ABCDE approach is important (Table 2), and referral should be made urgently if suspicions of melanoma are held.
Skin tones
It is important to note the differences of appearance of these skin lesions in different skin tones, especially for GDPs working in ethnically diverse regions. Malignant skin lesions in darker-toned skin are less common compared to Caucasian skin however it is important to identify their differences in presentation. When skin cancer does present in people of colour, morbidity and mortality is usually greater, emphasising the importance of GDPs in recognising and referring appropriately when suspicion arises. 17
Management
In general, the mainstay of skin cancer management is surgical, i.e. removal of the lesion with a margin of normal tissue. The subsequent defect can either be closed primarily, with the use of local skin flaps, or skin grafts. For BCCs, surgical removal is typically curative. For SCCs, radiotherapy may be indicated adjunctively for particularly aggressive lesions. For melanomas, surgical removal is typically curative, however neck dissection for removal of involved lymph nodes may also be indicated along with chemotherapy, radiotherapy, and immunotherapy in selected cases. The role of neck dissection in melanoma is controversial. Neck dissection in metastatic melanoma can be useful to prognosticate survival but does not necessarily actually increase overall survival, and patients should be made aware of this before pursuing surgery. 18 The removal of metastatic nodes from the neck can improve quality of life by preventing metastatic disease fungating through the neck skin, which is painful, malodourous and becomes frequently infected, making the final stages of life particularly unpleasant.
Topical drugs, such as 5-fluorouracil or imiquimod, are sometimes employed for the management of actinic keratoses, Bowen’s disease and superficial BCCs. Imiquimod may also be considered for the management of very early melanomas. 19 Cryotherapy – the application of liquid nitrogen – plays a role in the management of certain superficial lesions. 20
Following treatment, regular monitoring is important to identify future recurrence and to detect any new lesions, as patients are high-risk of developing new unrelated lesions.
Role of the DHP
First and foremost, the DHP must understand and appreciate their value and importance in screening for skin cancer. As healthcare professionals, trained to understand the anatomy of the head and neck, and experienced at examining patients, DHPs are ideally placed.
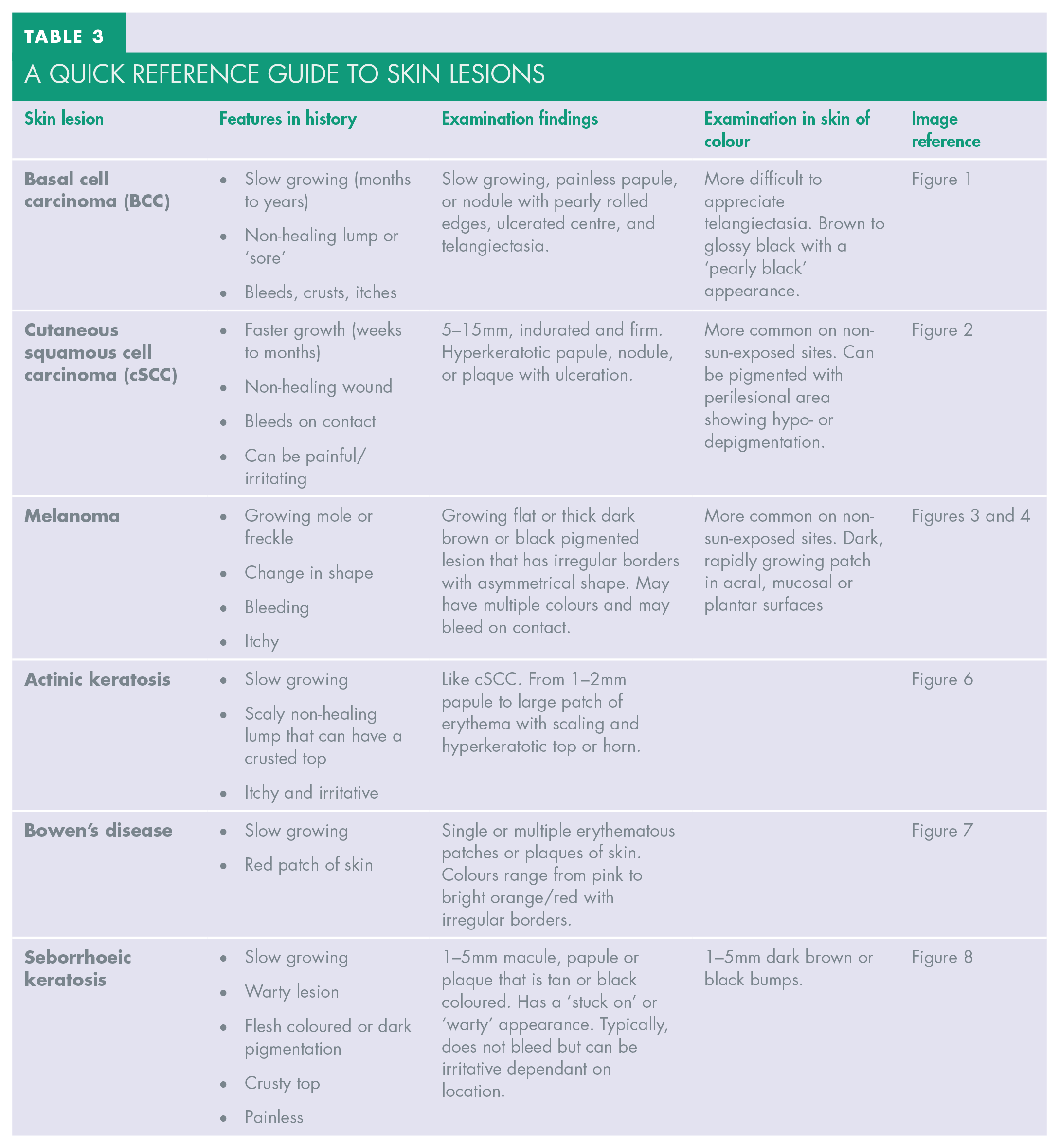
DHPs should incorporate skin cancer screening into their routine examinations, similar to oral cancer screening. This should involve assessment of the neck, face, ears, nose and scalp for any skin abnormalities. Most individuals will have lumps or regions of discolouration, and it is important for DHPs to be aware of which lesions will require further investigation and/or treatment (see Table 3). Being systematic in an examination prevents errors. Palpation of the cervical and facial lymph nodes is important to identify any nodal disease.
a quick reference guide to skin lesions
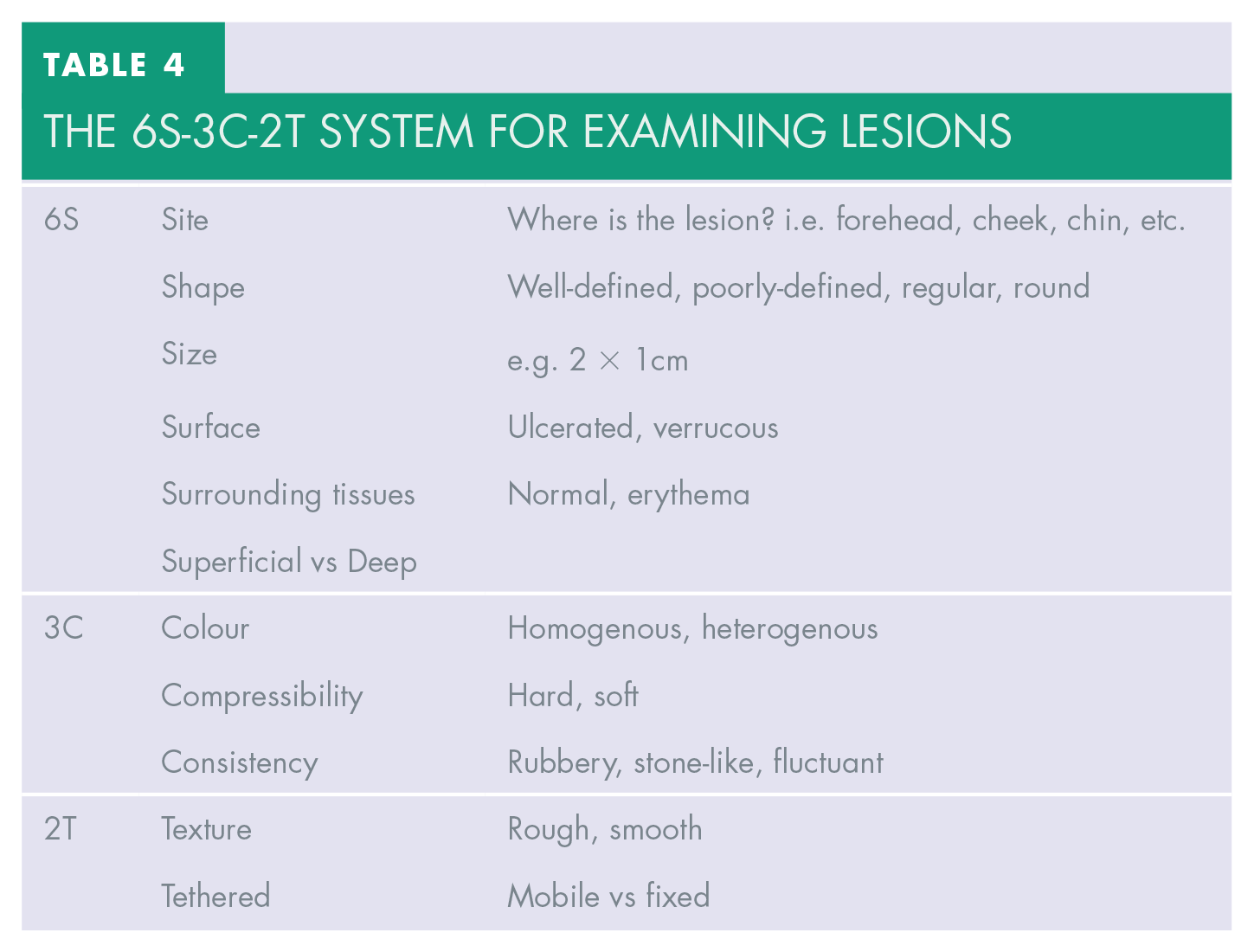
Lesions identified should be examined systemically and thoroughly. An easy-to-use system is 6S-3C-2T (see Table 4).
The 6S-3C-2T system for examining lesions
Service provision for the diagnosis and management of head and neck skin cancer is a postcode lottery in the UK. In some regions, such as East Lancashire, the service is provided by the oral and maxillofacial surgery team whereas in others, such as central Lancashire, it is provided by dermatology with plastic surgery input. DHPs should be aware of this and should refer patients to their GP if unsure about where to refer.
Conclusion
DHPs are perfectly placed to screen for skin cancer. Skin cancer screening should be regarded as integral to the DHP’s role, as oral cancer screening. Any concerns over lesions should be referred according to local service provision. If in doubt, referral to general medical practitioners is advised. DHPs should undergo targeted continuing professional development (CPD) to improve skin cancer recognition.