
Abstract
This article describes a practical approach to assessing compromised teeth using a process called ‘SHEEP scoring’ which is an acronym based on the categories of
Only when both sides understand the significant problems that already exist, should a ‘
Learning Objectives
To describe a prognosis and restorability scoring system for any compromised tooth in five relevant categories and be able to use those totalled scores to give an easy-to-understand ‘percentage chance’ for that tooth, well in advance of offering some treatment, or none
To help patients in their decision-making processes by communicating their tooth’s realistic prognosis, as part of the discussions for validity of consent reasons
Introduction
The assessment and management of compromised teeth is a routine part of general dental practice. Occasionally, dental practitioners may be uncertain about a compromised tooth in terms of the predictability of some intervention. This can place them in a precarious position when communicating information to the patient about their existing problems and predictability of prognosis with – or without – treatment. This article presents a practical approach to assessing compromised teeth using a ‘SHEEP scoring’ system (see following section). That should be done as a separate process and well in advance of offering any intervention. This analytic exercise helps busy clinicians to categorise various risk factors which can influence the prognosis of compromised teeth well before offering any ‘theoretically possible’ treatment. Rather than defaulting to some arbitrary but available, subjective, quick ‘solution’, undertaking an appropriate analysis first is a prudent approach to modern risk management. Partly due to increasing consumerist behaviours, many patients regard the identification of any problem before having any treatment as being ‘a diagnosis’. Any problem found after some well-intentioned treatment (that perhaps does not go as well as the patient expected) might be regarded by that ‘consumerist’ patient as ‘an excuse’– regardless of how unrealistic their unexpressed expectations of success might have been at the outset.
Presenting a logical assessment of their existing dental problems first helps patients to understand their issues well before they make any decisions. From the ethical and legal perspectives, patients need to understand their “material risks” as an essential part of the detailed discussions required for valid consent.1,2 The potential patient is given a readily understandable analysis of their problems first, and offered a ‘best-clinical-guess percentage chance’ of the likely outcomes of different approaches which should enable them to make better-informed choices about their realistically available options.
This consensual approach usually fosters a mutually collaborative patient–clinician relationship, particularly when this involves seeking a ‘satisficing’ outcome. “Satisficing” means aiming to achieve an outcome that is ‘sufficient to be satisfactory’ for both the patient and the clinician. A satisficing approach takes account of the real-life constraints of time, operator skills and financial means that are actually available, rather than one seeking out a largely theoretic or supposedly ‘ideal /gold standard’ or an academic or ‘maximalist’ outcome.3-5
The ‘SHEEP scoring’ system in assessing compromised teeth
The term ‘SHEEP scoring’ describes one practical system for ‘guesstimating’ early on the existing problems of any compromised tooth.
The acronym ‘SHEEP’ is made up of the first letters of
Scoring is done for each component of the SHEEP acronym, grading each category using a scale of one to ten, with one representing the lowest point (i.e. dreadful) and ten as the best (i.e. excellent).
Each tooth in question is given a score out of ten.
Grading each tooth in the order of the five described SHEEP categories and then totalling those scores in each gives an overall score out of fifty.
That cumulative score is multiplied by two to give an overall ‘percentage score’ for the tooth as things currently exist.
Working out that scoring first can help a busy clinician to quickly assign a prognosis to a tooth, in a way that is easy for patients to understand, before offering any possible treatment. Those options might range from doing nothing, to instituting effective preventive strategies, through to speculative endodontics, or on to undertaking a rapid extraction with, or without, a possible replacement. Obviously, things might change after extensive, time-consuming, speculative investigation, when more would be known, but this proposed SHEEP scoring exercise is done as a
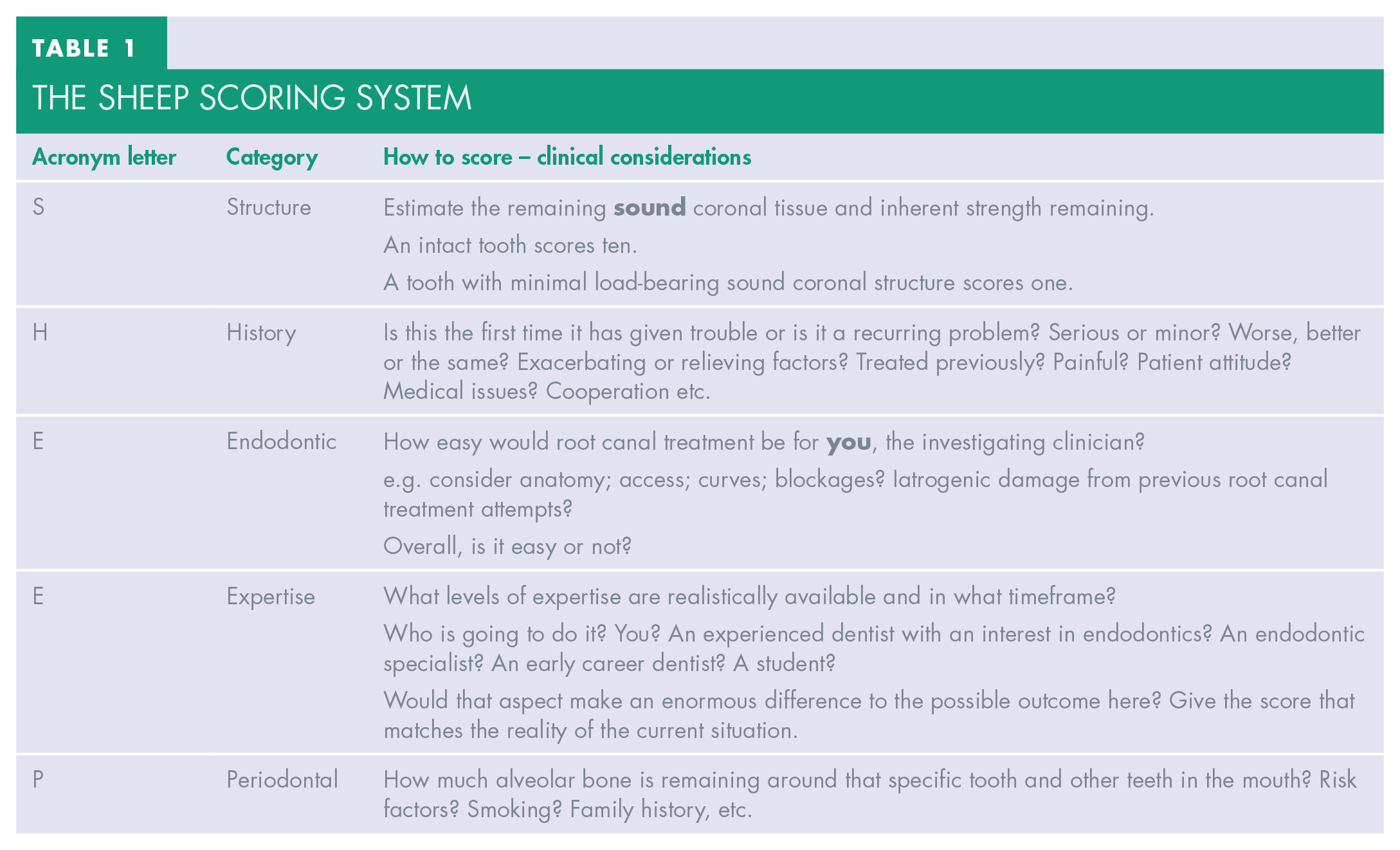
Table 1 shows the considerations for the SHEEP scoring system in action, remembering that:
each tooth in question is given a score out of ten
ten (10) is the top mark
one (1) is the bottom mark
The SHEEP scoring system
‘Rules of thumb’ and ‘heuristics’
‘Heuristics’ is a posh term in psychology for what most people would call ‘rules of thumb’. 3 Heuristics are shortcuts that our minds take in solving problems, in order to make acceptable decisions quickly given the time, resources and other constraints involved. We apply heuristics frequently in real-life situations, but not necessarily when it comes to dentistry. By using this SHEEP scoring system, the heuristic process is enabled and one can calculate – quickly and well in advance of offering any treatment – the likely outcome for any already compromised tooth in a way that most patients can immediately understand, in order to help them in their decision-making processes.
Calculating the SHEEP score takes around two minutes per tooth once all the relevant information has been obtained, and that totalled percentage SHEEP score usually leads easily into appropriate discussions with that potential patient.
Making a contemporaneous record in the patient’s notes of the numbers assigned in the different categories to produce that percentage score is a valuable way of demonstrating to that patient at any time in the future (and to any other potentially interested parties) that relevant discussions took place in advance of offering treatment – or no treatment – as chosen by the patient at that time.
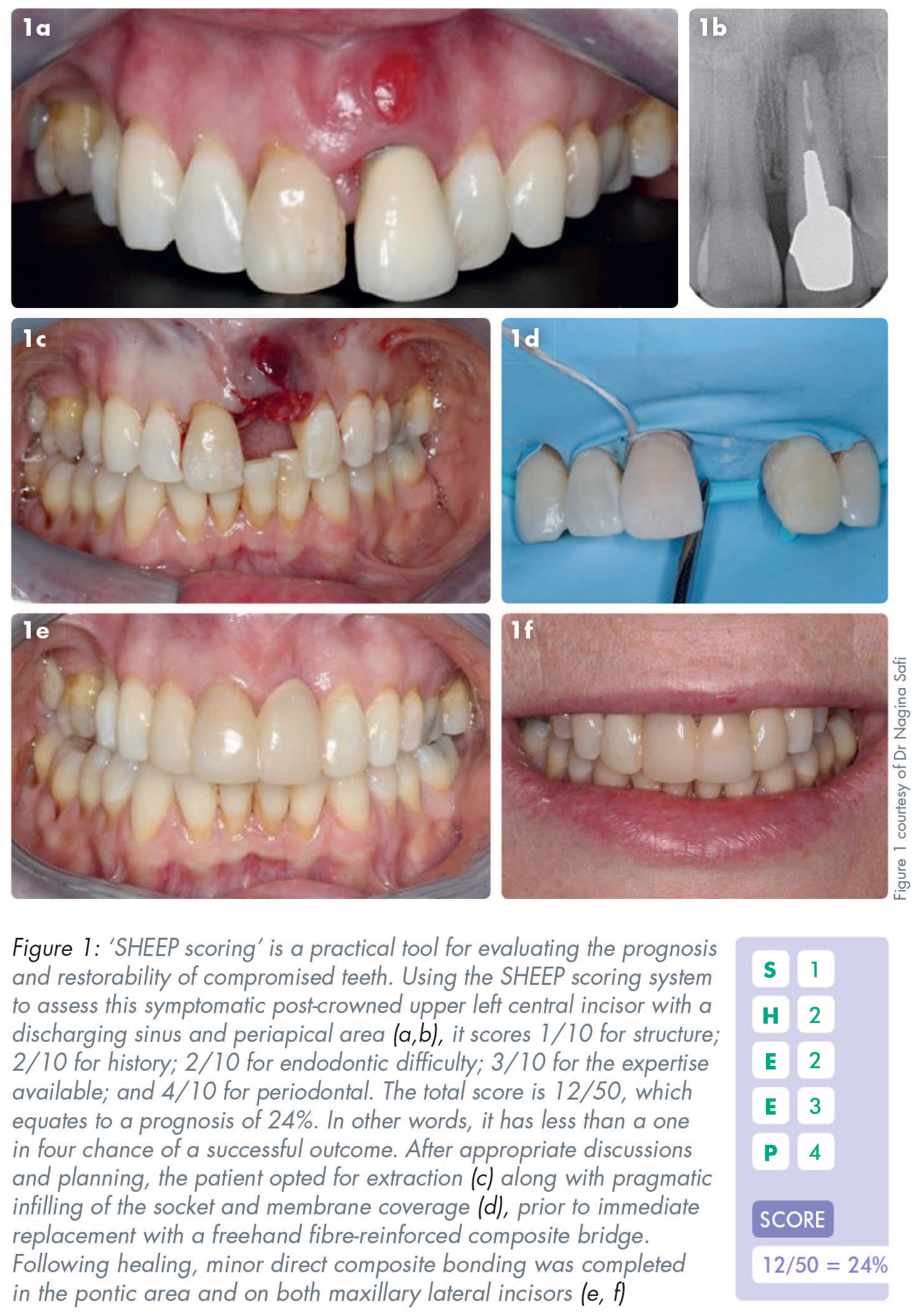
The clinical example in Figure 1 shows how the SHEEP scoring system can assist in discussions before decision making.
Order of assessment in S HEEP scoring: S tructure
The residual coronal tooth structure is assessed first. A score of ten is assigned to a completely intact, sound tooth. Marginal ridges maintain a tooth’s ring structure and overall integrity, which is critical to maintaining the tooth’s inherent strength. Consequently, a tooth that has one or more marginal ridges missing – regardless of aetiology – will be given a lower score for its structure, depending how much load-bearing sound coronal structure is now ‘guesstimated’ to be present. Incidentally, a guesstimate is a portmanteau word composed of guess and estimate. It involves giving an approximation or one’s ‘best clinical guess’ rather than it being a verifiable measurement done after extensive investigation. 6
Clinical and radiographic examination can be used to guesstimate the extent of the remaining sound tooth left. The presence of radiopaque areas within the tooth structure on the appropriate radiograph indicates metal or other restorative materials, and its size usually gives a good idea of the likely extent of the remaining sound tooth structure.
Porcelain-fused-to-metal (PFM) full crown preparations can remove up to two-thirds of the tooth structure, whereas gold crowns (partial or full) usually result in the removal of about one-third of the structure.7,8
The preparations for full coverage fixed-fixed PFM bridgework often remove more than two-thirds of the teeth to get one common path of insertion.
A post crown usually means that minimal sound coronal structure remains.
Apart from post crowns, full crown preparations for veneered zirconia, or porcelain bonded to metal (PBM) or other substrates, require the most destructive of the euphemistic ‘preparations’ for them.
The more extensive the root filling appears radiographically, the less sound load-bearing structure that is likely to remain.
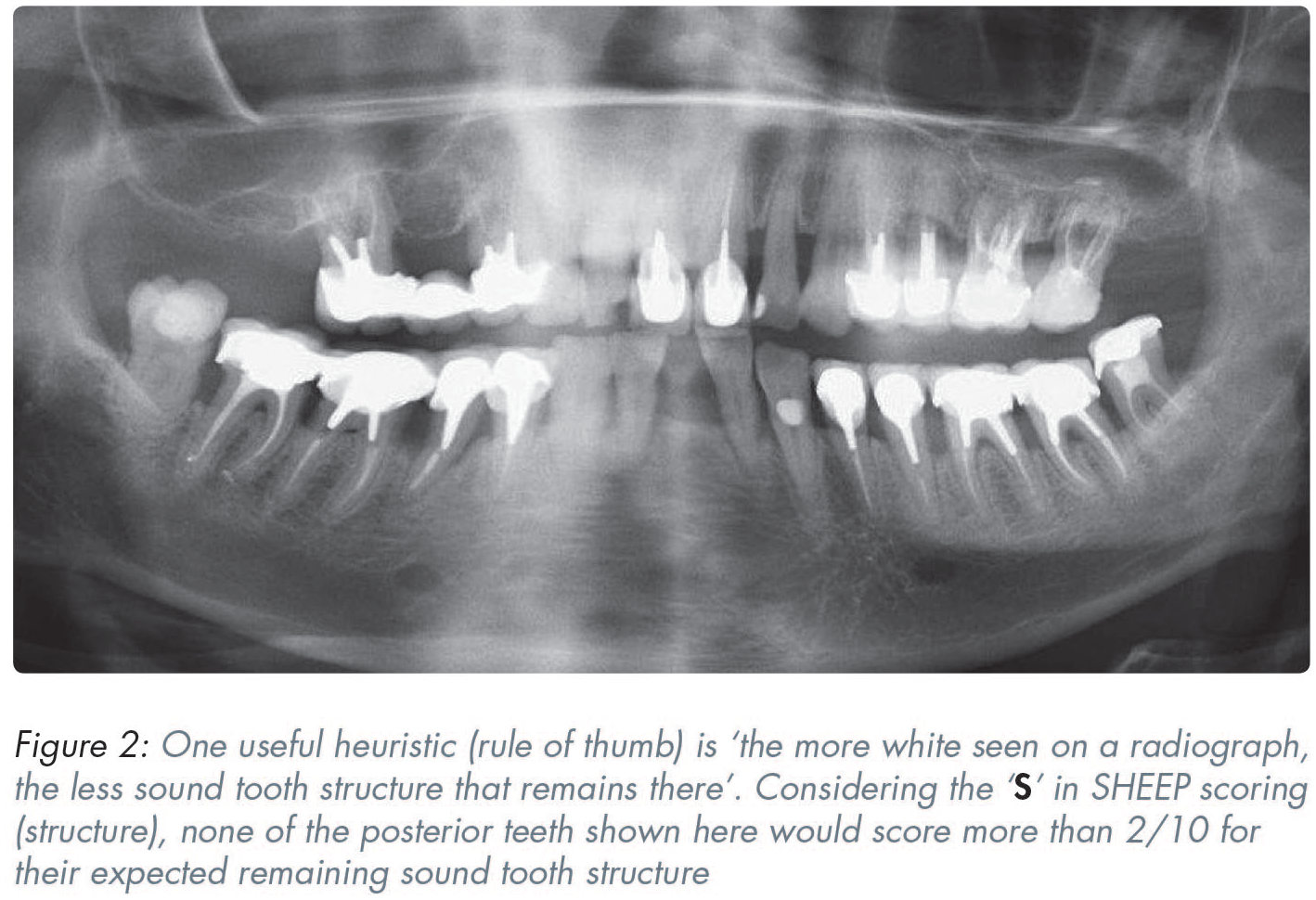
Curved root-filled canals often mean that there may well be less sound coronal tissue left (Figure 2).
If a tooth has had reasonable-looking endodontic treatment already, then the size of the endodontic access cavity, the size of the root filling, the presence of a periapical area(s) and/or knowledge of who has done it, can all help to guesstimate what is likely to be left of the coronal structure.
Examples of ‘guesstimating’ the ‘S’ in SHEEP scoring
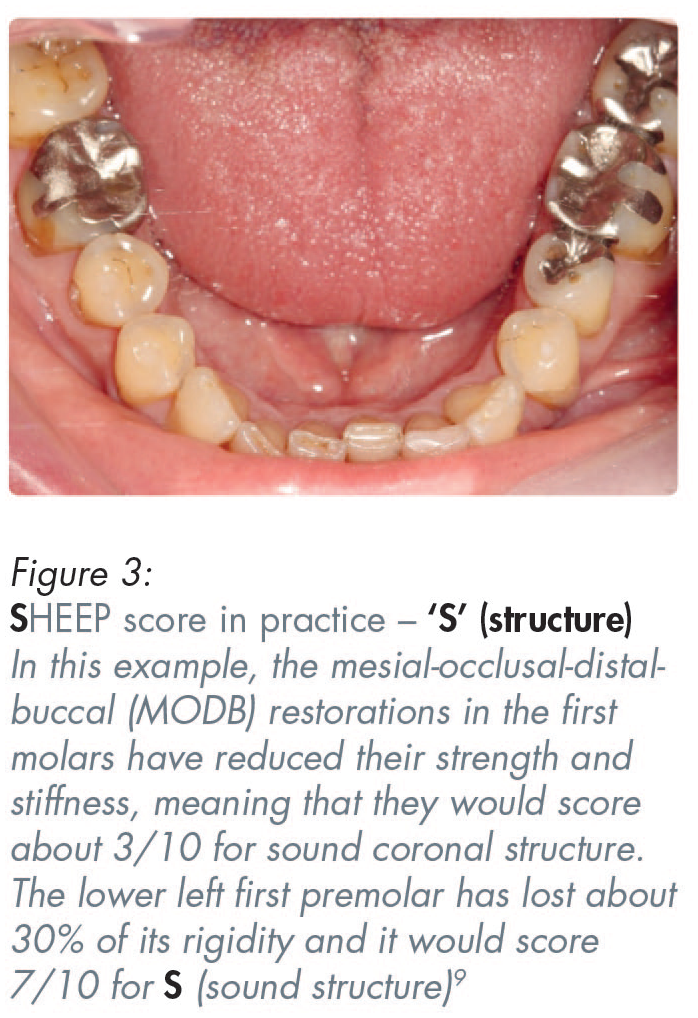
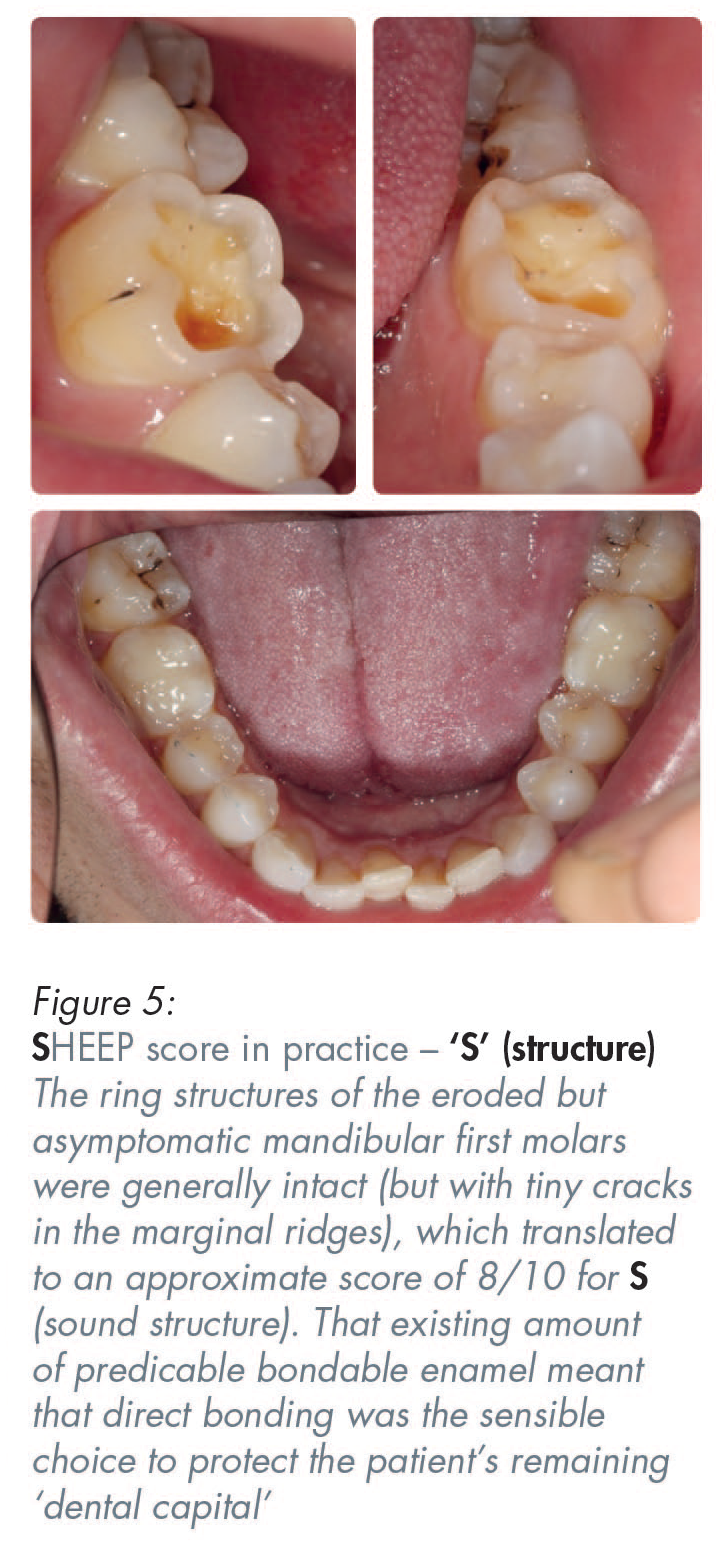
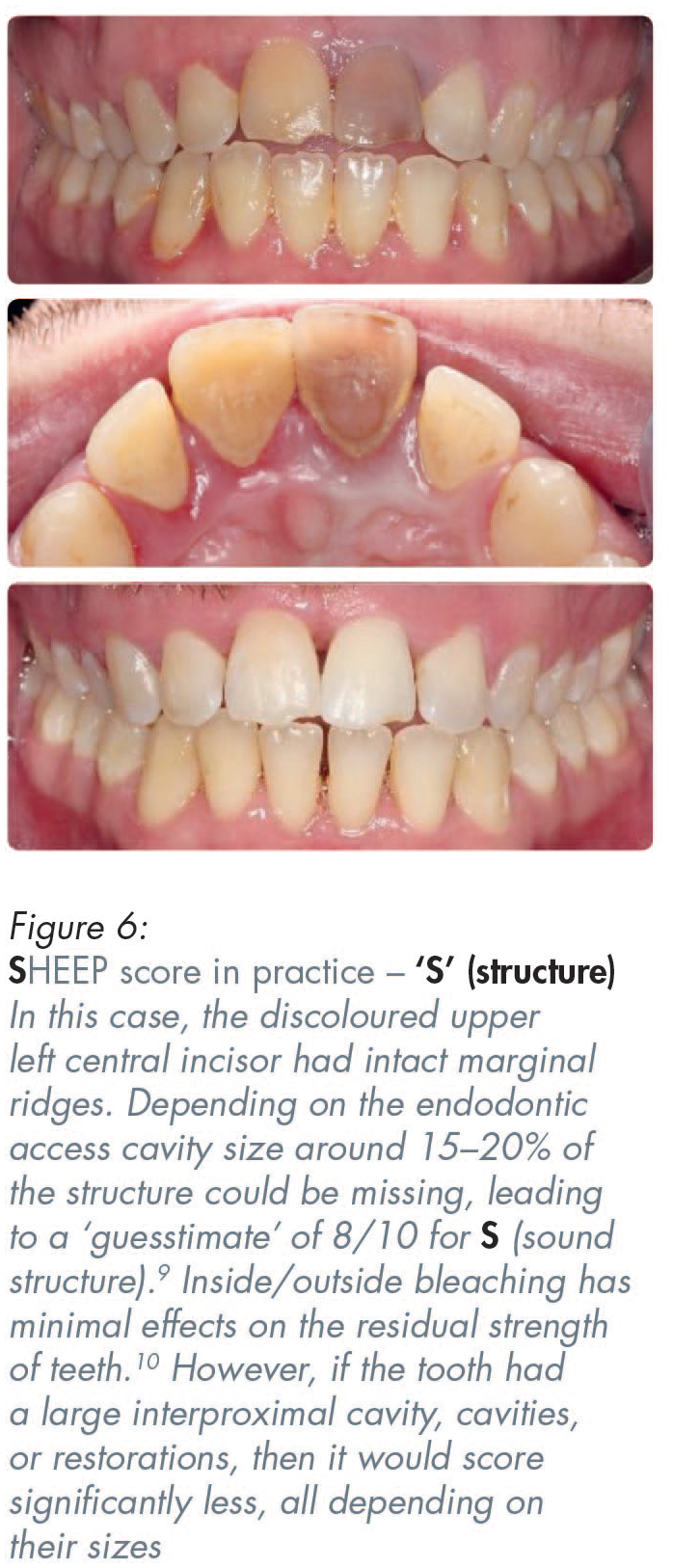
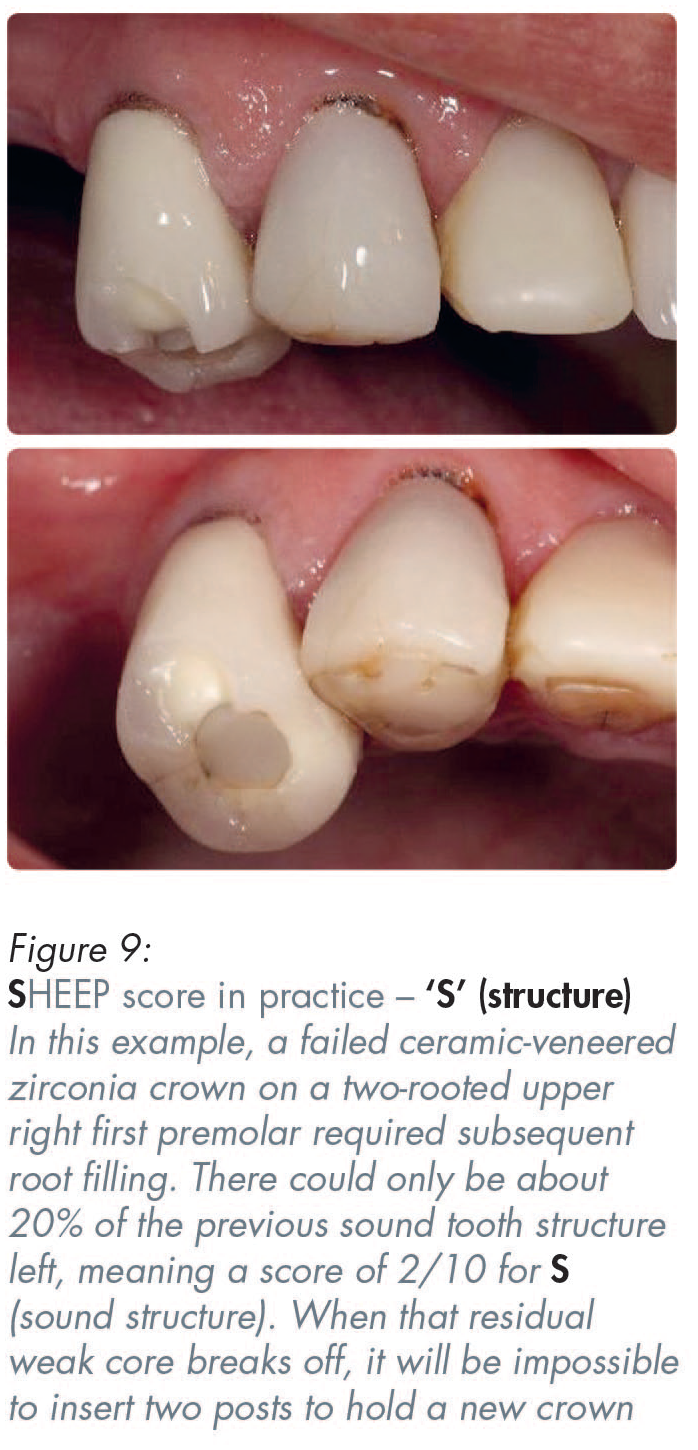
Figures 3–9 show practical examples of how the ‘S’ in SHEEP scoring (sound structure) can be guesstimated.
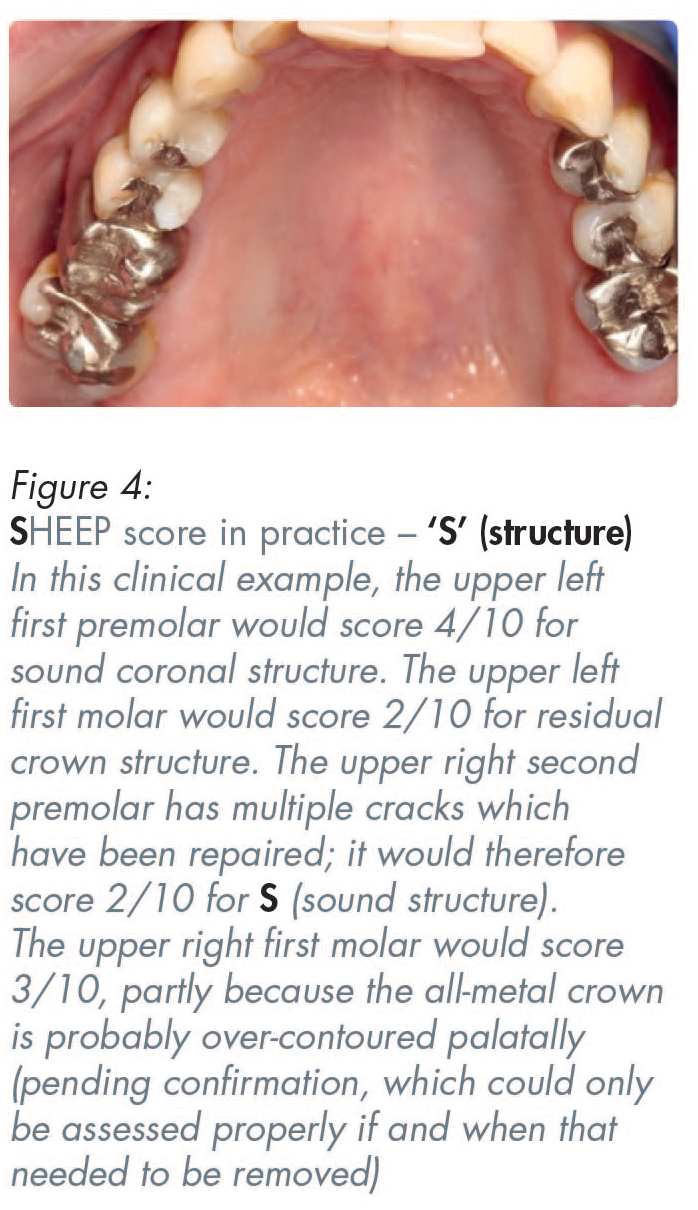


A zirconia full coverage crown, if made by scanning crown on a molar tooth, if made by digital intra-oral scanning, could score five out of ten (5/10) for ‘S’ (sound structure). That is because more destruction of the sound tooth must be done to create a rounded internal shoulder, which is what is required for the scanner to be able to read the deep margins of crown preparations on back teeth. In contrast to that unnecessary additional destruction of sound tooth structure to enable the use of scanners, conventional analogue impressions for conventional porcelain-bonded crowns, or all-metal crowns, only require a tooth-structure-sparing chamfer for most of the prepared tooth, thereby resulting in less residual sound tooth structure removal.11,12
Viewed from a structural perspective, a posterior traditional three-quarter gold crown would score five out of ten (5/10). However, that score could be reduced to about three out of ten (3/10) if a full coverage ‘white crown’ (i.e. a PBM or an all-ceramic crown) is present (Figures 2 and 8). The more sound structure that is destroyed for a full coverage all-ceramic, or ceramic bonded to some substrate crown, the more likely it is that the tooth will incur some consequential pulpal problems and therefore even more structural and/or endodontic long-term problems (Figures 2, 8 and 9).12,13
When assessing remaining load-bearing structure, one should also recognise that, when many teeth are missing, there will be increased functional load-per-unit-of-area applied to the remaining teeth.
Next in the order of assessment in SH EEP scoring: H istory
There are several risk factors influencing the score which could be attributed to the score assigned for the history.
Firstly, has the problem been caused by an isolated incident, such as freak dental trauma, which is unlikely to be repeated? Alternatively, is this an ongoing issue, such as recurrent decay beneath a large restoration or an existing crown or bridge? A recurring problem should be given a much lower score out of ten because the problems are ongoing and probably due to the previous risk factors not having been modified by the patient since the previous problems with that tooth.
A detailed medical and pain history should be obtained and the patient’s attitude to that tooth and possible treatment(s) should be ascertained.
Secondly, is addiction involved, and if so, is it likely to be an ongoing concern? Common addictions creating dental problems include addiction to a high sugar containing diet, smoking, hydrochloric acid from bulimia (pH 1–2), and parafunctional habits (e.g. bruxism). Clinicians often have to manage problems pragmatically by removing decay and placing an expedient restoration without the patient necessarily addressing their addiction habits, or their ineffective interdental or intra-crevicular cleaning. Unfortunately, such failures by the patient allows the ‘decay/filling/new decay’ cycle to continue until more invasive treatments, such as crowns, with or without some endodontic therapy, or extractions, then become necessary.
Thirdly, what is their smoking history? Smoking poses a significant indirect risk for developing dental caries, primarily through its impact on salivary flow, leading to xerostomia (dry mouth). A dry mouth is often very uncomfortable, causing smokers to drink fluids frequently to lubricate their mouth. However, these fluids lack the protective calcium and phosphate ions found in saliva. If those drinks or accompanying snacks contain even small amounts of sugar, that frequent sugar exposure, when coupled with the smoking-induced reduced salivary defence, can lead to recurring caries around the restoration(s) and that is often in more difficult-to-access areas of those already weakened teeth. Similarly, other patients with a dry mouth for different reasons may choose to drink highly acidic carbonated soft drinks, or acidic energy drinks, which can lead to progressive erosion of the teeth following frequent exposure, often resulting in the weakening of the teeth.
Fourthly, check the history of medications. Many commonly prescribed medications (which are often “anti-something” drugs for various conditions) can cause xerostomia and thereby indirectly increasing the risk of further dental caries, often around existing restorations, particularly in older patients. Older patients often manage their uncomfortable dry mouth by frequently sipping lubricating drinks that lack the protective properties of saliva and may well contain small amounts of fermentable carbohydrates/sugars, thereby heightening their risks for developing new carious lesions. 14
Order of assessment in SHE EP scoring: E ndodontic difficulty
Out of a maximum of ten, a score of ten (10/10) is assigned to a simple anterior tooth case involving a seemingly normal-sized canal system with reasonably easy access in a cooperative patient. A score of one (1/10) is assigned to a compromised tooth when one expects very serious anatomic, access or procedural difficulties.
Most teeth would be awarded an endodontic score of somewhere between 2–10 (see Figures 2, 10–13).
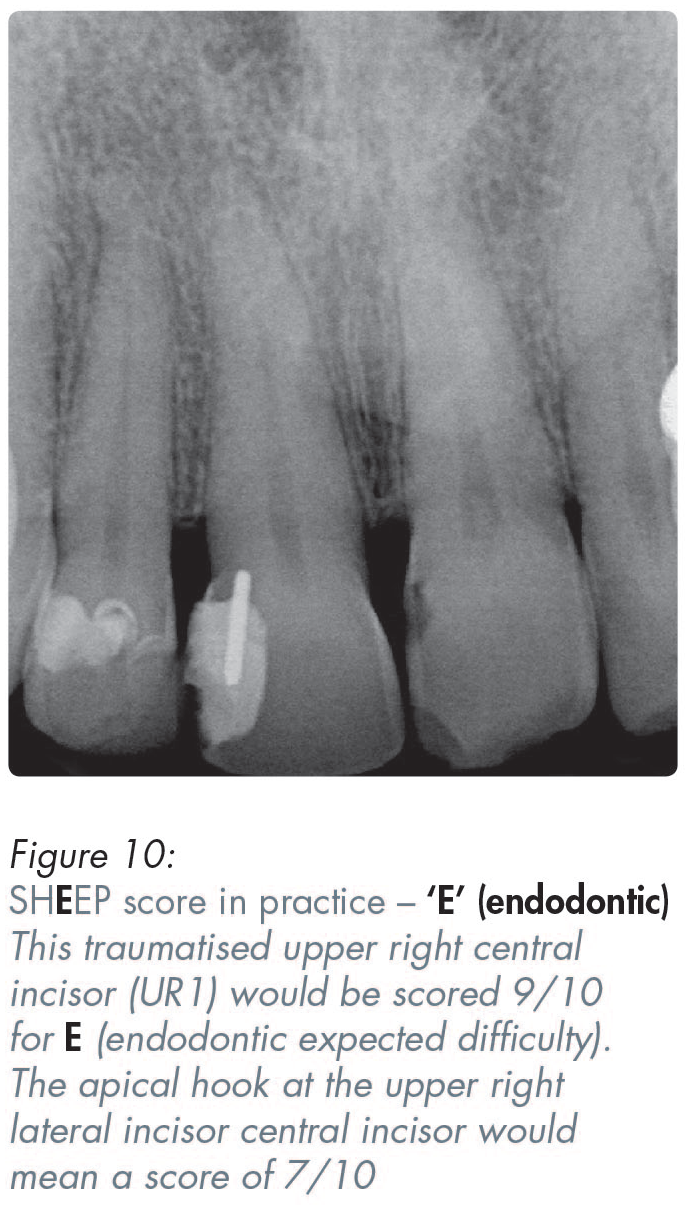
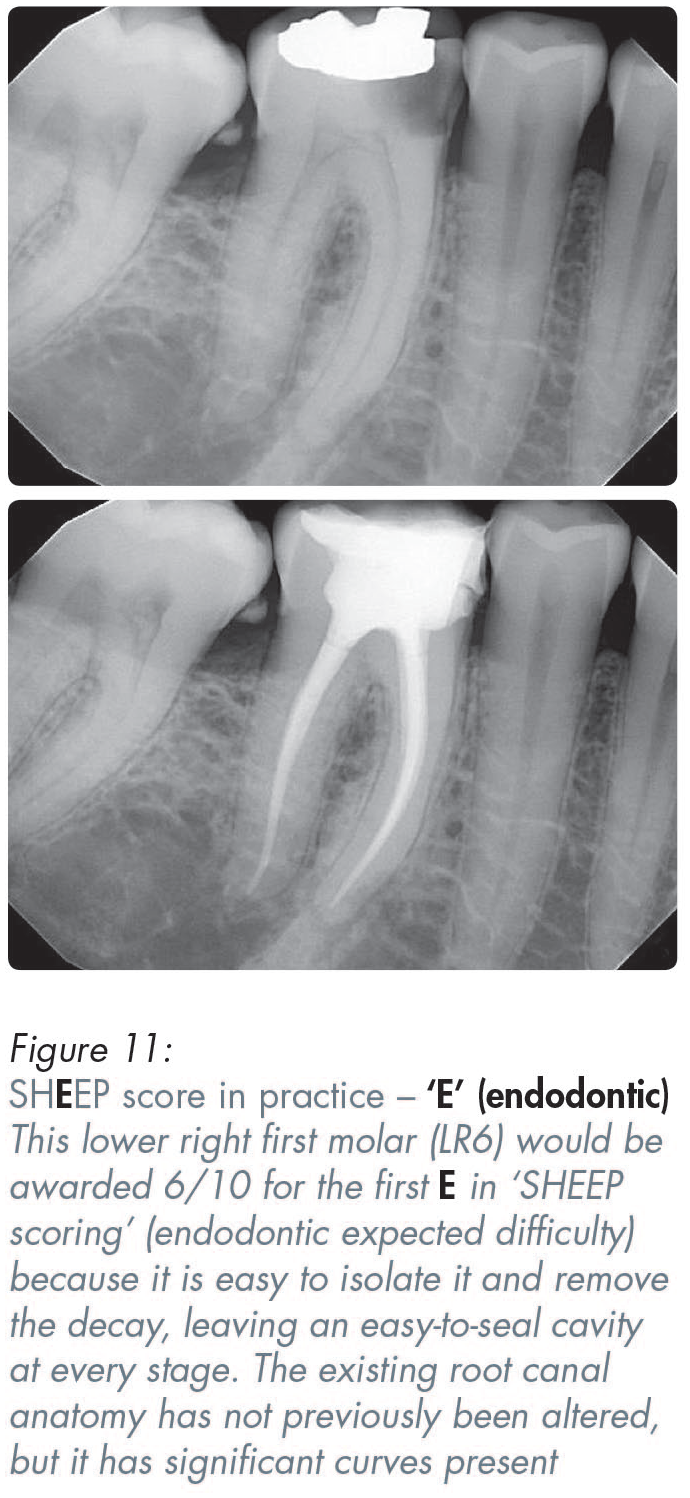
Important things to note include the visibility of the canals (i.e. whether they are wide or narrow, straight or curved), as well as the presence or absence of periapical radiolucencies, including their number and size (Figures 2, 10–13).
The integrity of the coronal seal is important at all stages of treatment – before, during and after endodontic therapy. The phrase “the coronal seal is the real deal” underscores the critical importance of the coronal seal as a major determinant of likely long-term endodontic success.15,16 It is important to evaluate early on whether the coronal seal has been compromised by restoration leakage or by decay contaminating the root canal system. Note how long this has been a problem, and if access to the root canal system has already been compromised by a post, a Nayyar core or some other bonded core which would need to be removed to gain access to the canal system.
The history of symptoms and signs (e.g. pain, sinus tract, swelling) should be correlated with the radiographic findings. In a previously root-treated tooth, it is important to consider the timing and provider of any existing root fillings, the extent and quality of the obturation (e.g. obvious voids, over-extension or under-extension), and any persistent periapical lesions, especially if the root filling appears adequate. Additionally, the radiographic appearance of other previously root-filled teeth may offer insight into the patient’s healing potential, meaning whether they are likely to be a “good healer” or a “poor healer”. Various preoperative factors have been identified that can influence the outcome of root canal treatment.16,17
Further considerations include the likelihood of encountering procedural challenges such as existing canal blockages or likely perforations. Practical aspects of patient management should also be evaluated, including that the patient’s attitude to that tooth, their cooperation, nervousness, or their desire (or likely tolerance) for prolonged treatment sessions, and any limitations in their mouth opening.
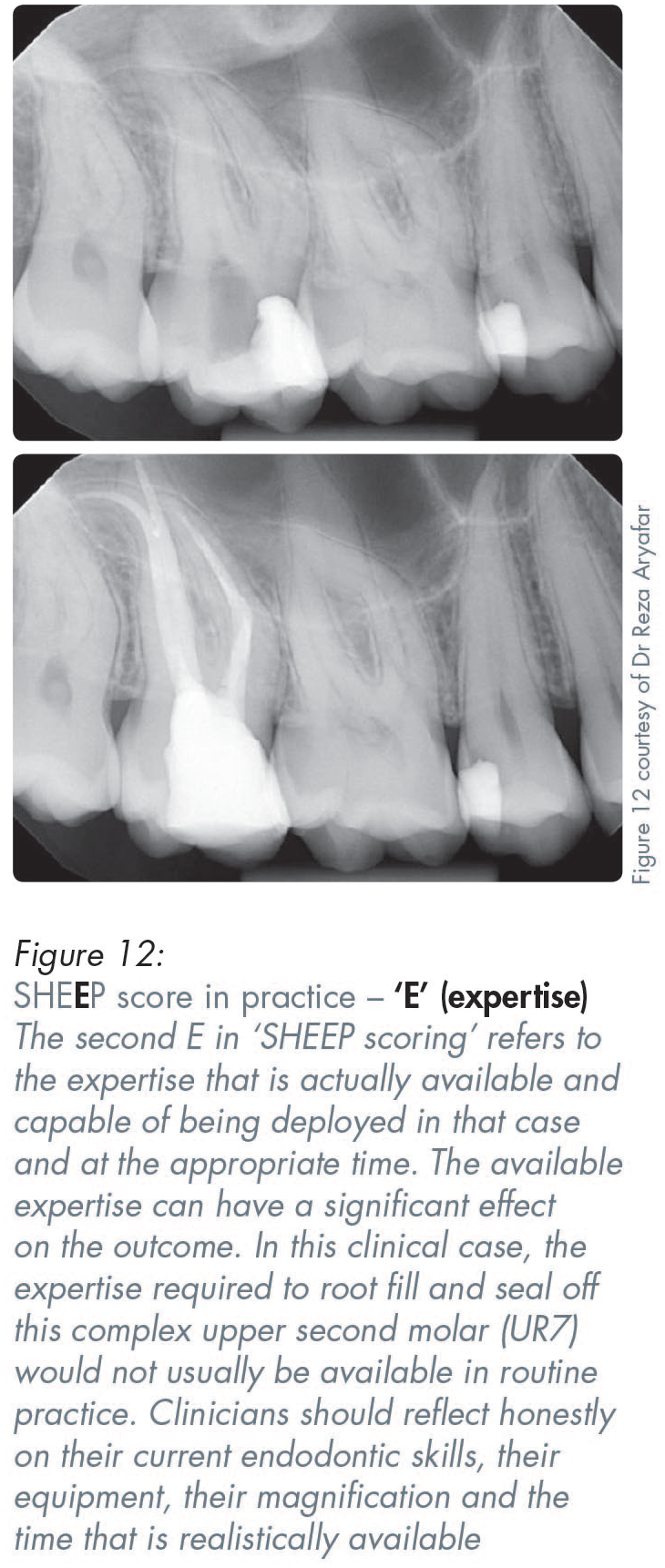
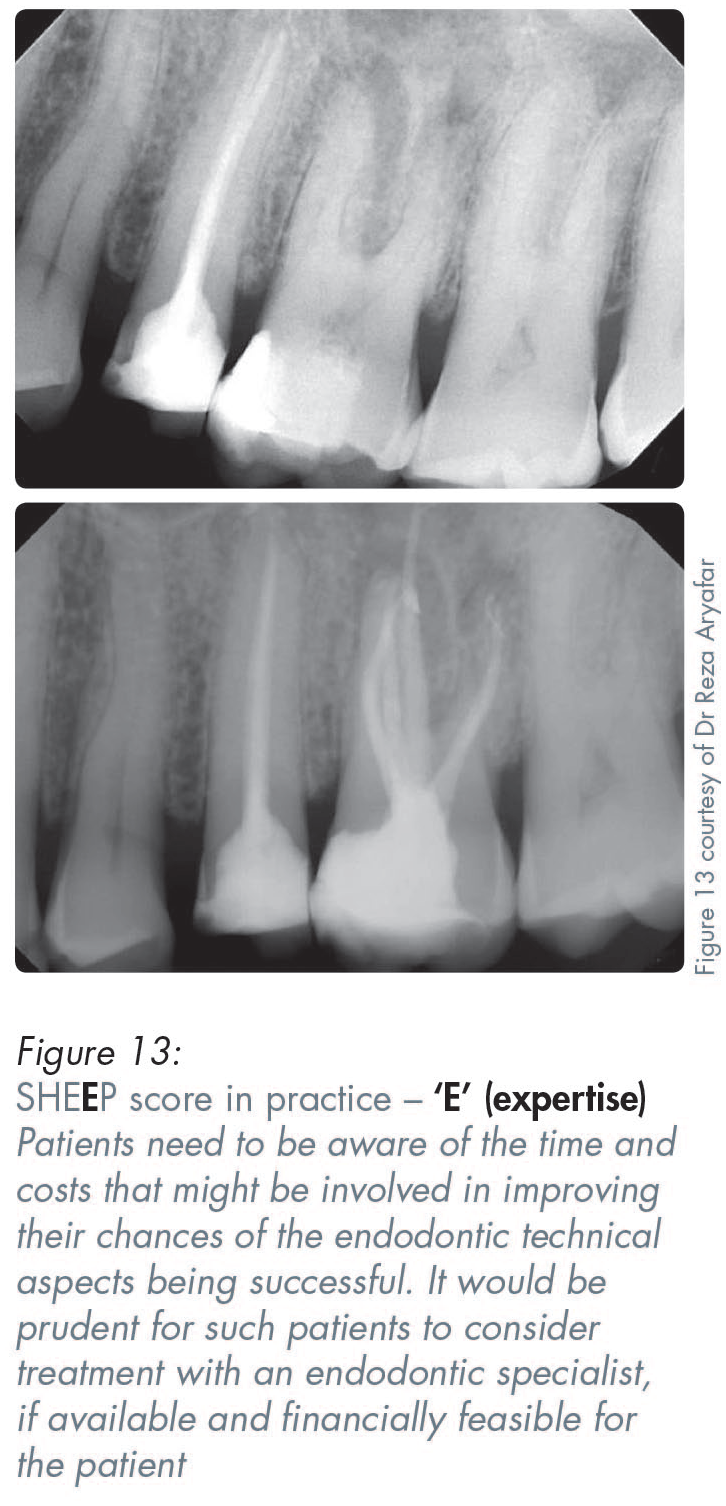
Order of assessment in SHEE P scoring: E xpertise
This involves an honest appraisal of the clinician’s practical endodontic expertise and whether a specialist endodontist is readily available in the required timeframe to do the treatment.
A self-assessment scale is used, wherein a score of 10/10 indicates that an unhurried minor deity in endodontics, surrounded by all their toys, will be doing the endodontic treatment. A score of 1/10 represents endodontic treatment being undertaken by a novice without magnification or good endodontic instrumentation. The greater the endodontic expertise that is realistically available (meaning not just theoretically available in a wishfully imagined utopia), the higher the score that might be awarded.
While a specialist endodontist might well enhance the chances of technical endodontic success, particularly in anatomically challenging cases, even the most skilled endodontist cannot regenerate lost coronal structure. That is why the residual tooth structure must be evaluated first. Even if the endodontic procedure itself is technically successful, one major concern is whether that residual tooth structure would now withstand future normal, or parafunctional, occlusal forces.
If the residual sound structure is very weak, consideration should be given to the root-filled tooth being preserved primarily to maintain alveolar bone and proprioception from the periodontal ligament, and/or keeping the important associated soft tissue support in an area of high aesthetic importance. Other strategies could include retaining the root as an overdenture abutment, or intentionally just covering it with glass ionomer cement, or submerging it in order to avoid an extraction, thereby reducing the risk of medication-related osteonecrosis of the jaw (MRONJ) or of osteoradionecrosis in an at-risk patient, or perhaps deliberately maintaining the bone around it as a potential site for future implant placement.
Order of assessment in SHEEP scoring: P eriodontal
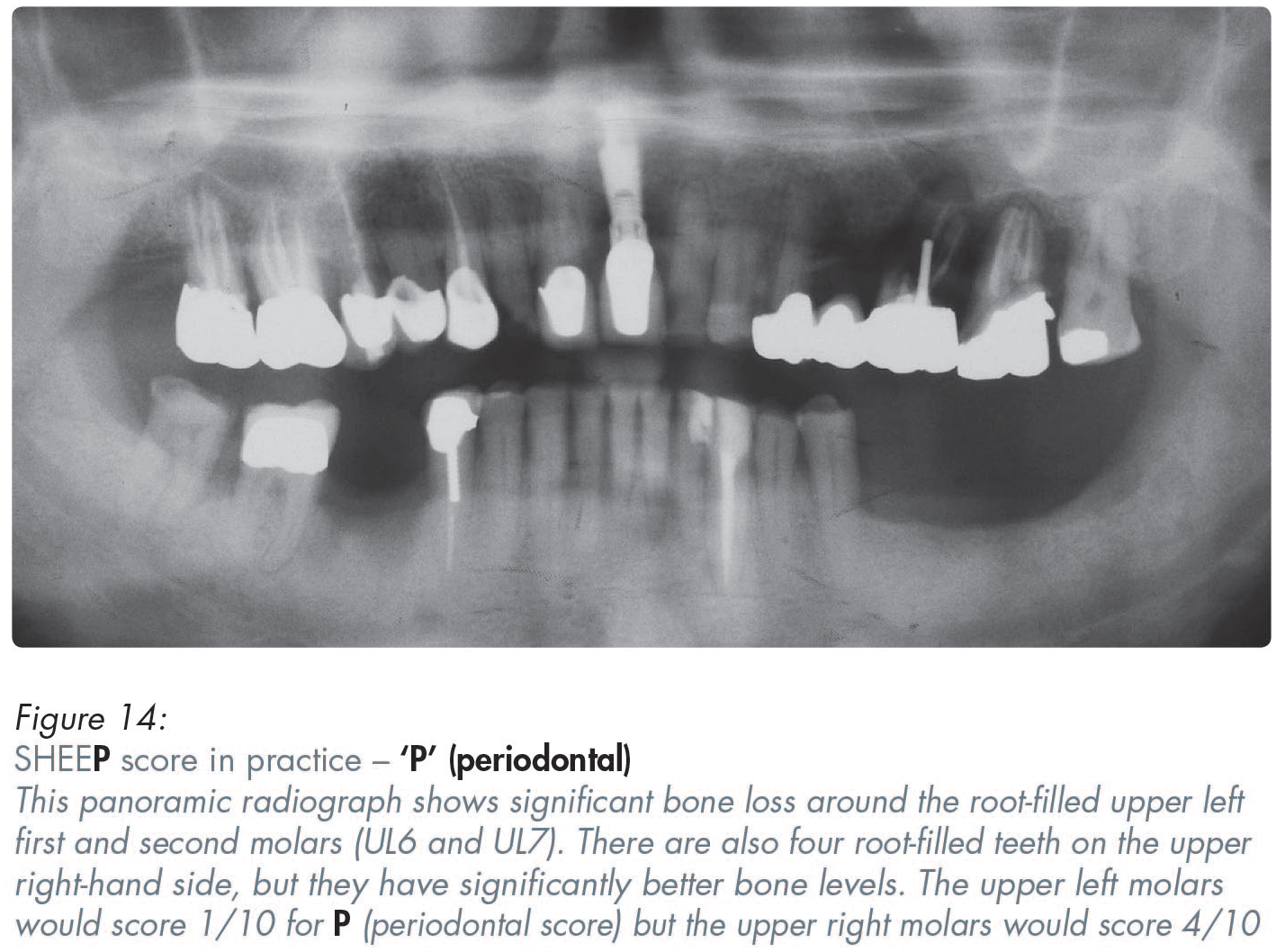
In assessing the ‘P’ in SHEEP scoring, emphasis is placed on the amount of supporting bone left around that tooth and elsewhere in the mouth, as judged from radiographic examination. A score of ten out of ten (10/10) indicates full support, while a score of one (1/10) indicates that the tooth is at risk of imminent exfoliation (Figure 14).
One pertinent question related to the ‘P’ in SHEEP scoring (meaning periodontal status) is whether the tooth is likely to be lost mainly due to periodontal factors? If that is likely, then the less bone left, the lower the score allocated. An assessment of the patient’s interdental cleaning, genetic and any other ongoing risk factors will impact on the score that is assigned.
Smoking cessation is critical for patients with significant susceptibility to periodontal diseases, especially if they have a family history of serious periodontitis. It has been known for more than 25 years that 53% of periodontitis cases are attributable to smoking, with 42% linked to current smokers and 11% to former smokers. 18 Even if the patient quits smoking, relapse in smokers is common. Unfortunately for them and their teeth, individuals with addictive personalities often shift from one addictive substance or behaviour to another, such as transitioning from smoking to vaping which has, at present, unknown long-term periodontal consequences. Vaping is certainly not risk-free from a long-term oral health or dental disease perspective, but it might well be better than smoking for lung and cardiac reasons. There is a new, very worrying, trend emerging in ‘never smoker’ young adults now vaping. 19
Smoking addiction and relapse also pose serious risks for dental implants, especially in poor quality or grafted bone, and can significantly compromise implant prognosis. When a former smoker relapses, this poses longer-term risks for their implants. Some smokers manage to give up temporarily for the assessment, surgical and healing phases, but any serious relapse can significantly compromise implant prognosis, and any loss of load-bearing implants can then throw extra loads onto already weakened teeth. 20
Exceptions when assessing ‘P’ in SHEEP scoring
If the compromised tooth is well-supported by bone and there is little bone loss elsewhere, it might be at minimal risk of being lost for
Where periodontitis is not the main risk, then excluding the periodontal assessment – ‘P score’ – from the SHEEP calculation often provides a more realistic prognosis, because that individual ‘P score’ would not be clinically relevant to that tooth’s long-term outlook (Figures 10–13). In such cases, where there is no realistic chance of the tooth being lost from periodontitis alone, then the scores from just the first four letters of the SHEEP acronym (i.e. only the structure, history, endodontic and expertise scores) should be totalled to give a combined score out of
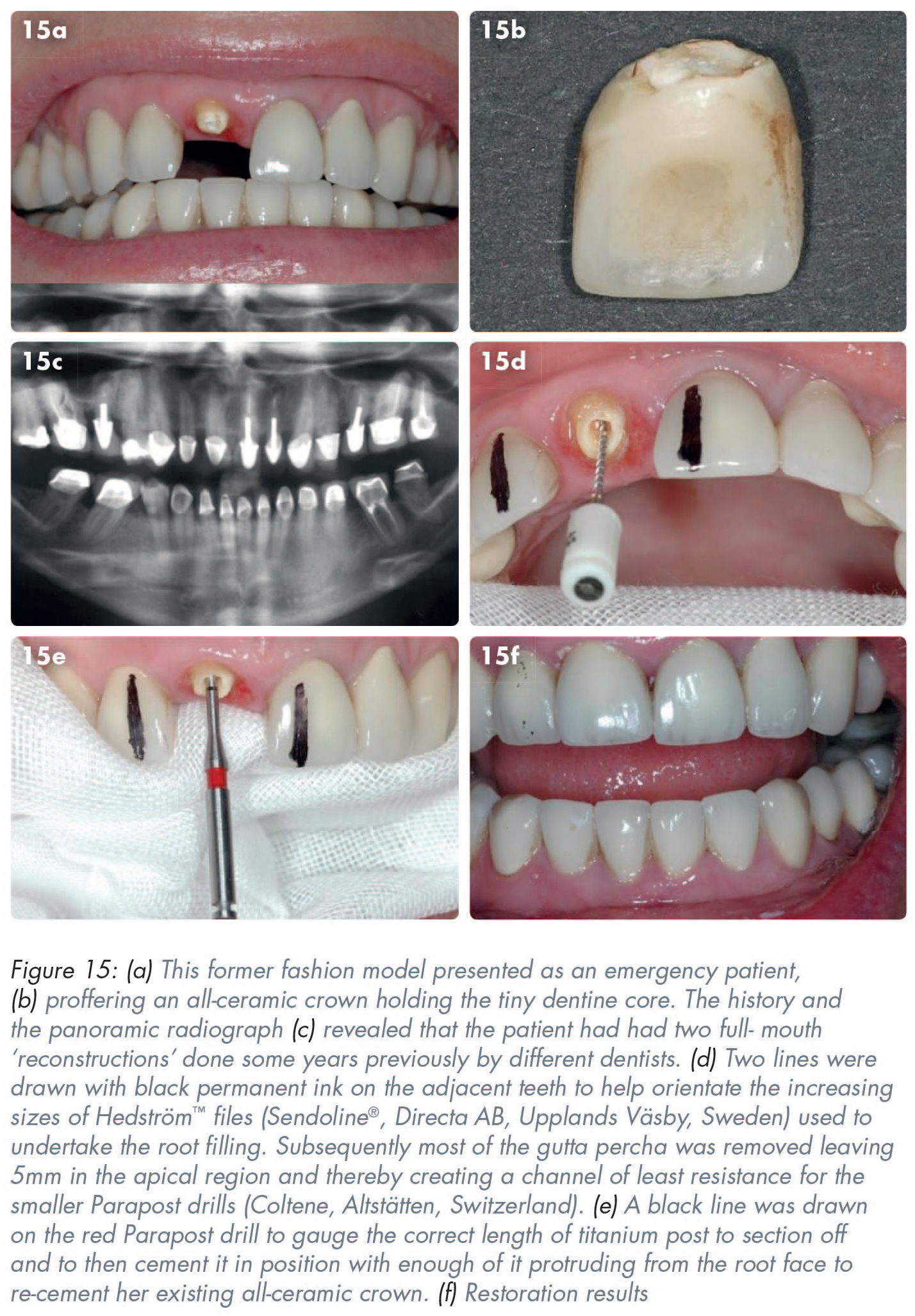
In assessing the case shown in Figure 15 – and well before detailed discussions or potential consent being given by the patient, or acceptance by the clinician to treat the patient – restorability SHEEP scores were calculated:
However, because the upper right central incisor would not be lost for periodontal reasons alone the
At that point both the clinician and the patient had choices about how to proceed, with both parties now knowing those odds. Different people choose differently when faced with similar situations, partially depending on their resources and risk appetite. Edward de Bono’s Six Thinking Hats approach was called upon here. 21 That logical approach recognises that hard facts do matter, but so do emotions (on both the part of the patient and the clinician), as does creative thinking, and having a well-developed sense of potential dangers before undertaking some theoretically possible treatments. . . or none.3-5,7-9,16-18,21 Following discussions about the problems and the lack of guarantees, and partly because the patient was due to attend an important wedding imminently, the tooth was root-filled immediately and most of the gutta percha removed leaving 5mm apically. An appropriate length and diameter of a titanium Parapost (Coltene, Altstätten, Switzerland) was cut off and cemented before then drilling out the fractured dentine core, etching the internal aspect of that all-ceramic crown with hydrofluoric acid, silanating it and then re-cementing it. (Incidentally, the restoration was still there at review nine years later).
Conclusion
Based on over 40 years of experience, this SHEEP scoring assessment tool is appreciated greatly by many patients due to it being readily understandable. Producing a ‘bottom line summary’ takes about two minutes per tooth once the relevant information has been obtained. Most patients’ understanding of their existing problems is improved by showing them images of their teeth while explaining how those images probably correlate with their history and any relevant clinical and radiographic findings. However, summarising all that relevant information quickly and understandably as a ‘percentage chance’ separately and well before committing either side to anything, is a sensible, modern approach to clinical risk management in dental practice.