
Abstract
Silver diamine fluoride (SDF) and atraumatic restorative treatment (ART) are treatment modalities that are minimally invasive and used for the prevention and control of dental caries. The amalgamation of these two techniques has led to the development of silver modified atraumatic restorative treatment (SMART). In this approach the carious lesion is restored with glass-ionomer cement (GIC) after SDF application. SMART effectively arrests caries without removing additional tooth structure, making it a promising option for caries management in children who lack cooperative ability.
This article reviews the literature on SMART, the evidence regarding its applications in dental practice, its advantages, drawbacks, the scope for research, and clinical use.
Keywords
Learning Objectives
To overview the literature on SMART including the clinical procedure
To understand the current evidence on the clinical effectiveness of SMART and the use of techniques for its better effectiveness in clinical practice
Introduction
Techniques for managing dental caries have advanced well beyond “drilling and filling”, which only partially addresses disease. 1 Minimal intervention dentistry (MID) focuses on the medical management of dental caries that involves risk assessment, early diagnosis and interception, and conservative approaches to caries removal and restoration. 2
Silver diamine fluoride (SDF) is a cariostatic compound that can be utilised following the MID principles for arresting caries in cavitated lesions. 1 Atraumatic restorative treatment (ART), another MID treatment modality, has gained acceptance over the years for caries control. This procedure has been recommended to restore carious lesions in young, uncooperative children with multiple carious lesions. 3 The amalgamation of these two minimally invasive techniques has led to the development of a paradigm-shifting concept called silver modified atraumatic restorative treatment (SMART). This approach restores a carious lesion with glass-ionomer cement (GIC) after initial SDF application. 1
This article reviews the literature on SMART, the evidence regarding its applications in dental practice, its advantages, drawbacks, and future scope for research, and clinical use.
Role of SDF in SMART
SDF is a clear, odourless solution comprising silver, fluoride, and ammonium ions, with ammonia as a stabilising agent, used at a concentration of 38%. It has a high fluoride ion concentration of 44,800 parts per million (ppm). 4 Application on the carious tooth causes a series of chemical reactions resulting in tooth desensitisation and arrest of the carious lesion via occlusion of the dentinal tubules, remineralisation, bacterial mortality, and suppression of dentine collagen degradation. 5 Silver ions directly inhibit the growth of bacteria by rupturing their membranes, denaturing their proteins, and blocking their DNA replication. 5 Fluoride causes remineralisation through the production of fluorapatite and has antibacterial action in an acidic environment, which is synergistic with silver ions. As a result, the dentine becomes more resistant to biofilm formation, thus preventing further caries progression. 6
SDF is used to cause the arrest of carious lesions in uncooperative paediatric patients, individuals with special health care needs, and medically compromised patients where pharmacological behaviour management techniques are not opted for by the parents/carers or are contraindicated.5,7 A significant downside of SDF is that it stains the demineralised areas in which it is in direct contact. The stains usually do not emerge immediately, and it may take a few hours to appear. 8 Applying potassium iodide (KI) after SDF removes excess silver ions, producing insoluble silver iodide precipitate, reducing the silver ions penetrating dentinal tubules. The use of glutathione is another alternative to reduce the staining effects of silver ions. 9
From the currently available research, it is still being determined whether or how frequently SDF reapplication is necessary to retain the impact of the initial application. 7 Biannual SDF reapplications result in a higher caries arrest rate than a single application, particularly in patients with poor oral hygiene.4,10
Are restorations required after the SDF application?
Though many dental carious lesions are arrested after SDF application, randomised clinical trials with long-term follow-up have shown failure to arrest some carious lesions. Multiple SDF applications are necessary for more reliable caries arrest. 5 Thus, caries arrest is dependent on patient compliance for multiple visits. Open cavities can become areas for food lodgement and plaque accumulation, especially in individuals with poor oral hygiene. 11 Lack of regular tooth brushing can result in persistent visible plaque that affects the effectiveness of carious lesion arrest.7,12
SDF application does not restore the lost structure and may not improve the masticatory function and occlusion. 13 Hence, restoring cavitated lesions after treatment with SDF can be beneficial. 11 The source of nourishment for any remaining microorganisms in the cavity is warded off by placing a restoration that bonds to the tooth structure and provides a seal.1,14 The restorative material should be such that it should synergistically enhance the remineralisation of the carious lesion due to SDF. Restoration of cavitated lesions extending to dentine after SDF application will help in tooth structure conservation and pulp vitality maintenance. 1 The restoration will also mask the colour changes due to SDF and improve aesthetics. 15
Atraumatic restorative treatment (ART)
ART is a minimally invasive procedure for restoring cavitated lesions. Hand instruments are used to remove decay, followed by restoration with fluoride-releasing adhesive materials such as GIC. The remaining pit and fissures are sealed simultaneously during the restorative procedure.3,16 The high-viscosity type of GIC (HVGIC) is the most used restorative material. They are preferred due to the ability of the material to physico-chemically bond to the tooth structure, the low co-efficient of thermal expansion, fluoride release and ability to withstand high masticatory stress due to better mechanical properties.17,18 Caries removal to firm dentine is done in medium-depth cavities, while carious tissue is removed to soft dentine for deep carious lesions to prevent pulp exposure. 14 The selective caries removal technique is thus used in ART, per the recommendations of the International Caries Consensus Collaboration (ICCC).14,19
Benefits of ART include minimal cavity preparation compared to traditional techniques, low costs, and lower anxiety levels in children and adults (more “patient-friendly”). 19 According to a systematic review, 20 restoration failure rates with ART are 1.6 times higher than conventional GIC restorations.
One of the most common reasons for the failure of ART restoration is marginal secondary caries due to marginal gaps in the restoration. 20 The high viscosity of the HVGIC can affect the close adaptation of the restorative material to the dentine surface leading to marginal gaps and microleakage. 21 Residual bacteria may remain after hand excavation, persist for over two years, and contribute to caries progression. 22
Over the years, caries removal with rotary instruments and restoration with other materials like fluoride-releasing resin-modified glass ionomers (RMGIC), glass hybrid GICs, and resin composites have been used, and these are termed modified ART restorations, as opposed to conventional ART restorations that use HVGIC for restoring the hand-excavated cavities. 19 The SMART technique is one such modified ART restoration concept that has been implemented recently.
Concept of silver modified atraumatic restorative treatment (SMART)
The antibacterial and remineralisation action of SDF combined with the fluoride release by the GIC could synergise and ensure the success of ART by minimising secondary caries occurrence. Hence, SDF application is recommended before restoration with the ART approach, despite the discolouration caused by SDF. 23
Children who do not have access to a dental facility and lack cooperative ability are candidates for SDF. Such children are not likely to return for subsequent treatment.1,23 When a patient is not likely to return for future dental visits, performing a minimally invasive restoration is preferable to no restoration. Restoring the cavitated lesions with GIC using the ART approach after SDF application can be more beneficial in these child patients, as it limits fermentable carbohydrate access and improves the chances of caries arrest by SDF. 1 The technique of SDF application prior to GIC placement helps provide restorative treatment to paediatric patients who cannot cooperate even for caries removal using hand instruments as in the ART technique, as it simplifies the treatment procedure and minimises discomfort for the patient. 23 This treatment modality has been well accepted by parents, improving parental satisfaction regarding their children’s oral health. 13
Advantages of SMART
The technique allows for minimal removal of soft caries, contributing to the maintenance of the vitality of the asymptomatic pulp and conservation of tooth structure. 1
The remaining caries is arrested owing to SDF’s antimicrobial and remineralising actions. 8 Approximately 80% of treated lesions are arrested by SDF, indicating it to be an effective method. 7
SDF application takes minimal time and it is easy to apply. It is a safe treatment option. Clinical trials involving more than 3,800 participants showed no significant adverse events following SDF application. 7
Cavities can be restored after minimal cavity preparation, making it a painless patient-centered technique. A cavity seal is achieved by restoring with GIC which chemically bonds to the tooth structure. The restoration cuts off the nutrient source for the bacteria that may remain beneath the restoration.1,13
Enhanced remineralisation is achieved due to the synergistic action of SDF and GIC. Fluoride and strontium ions released from GIC and fluoride from SDF have a synergistic effect on remineralisation. 8
The SMART technique
Currently, no standardised protocol is available for this technique. However, there are two strategies based on the time at which the ART restoration is done (see Figure 1): 24
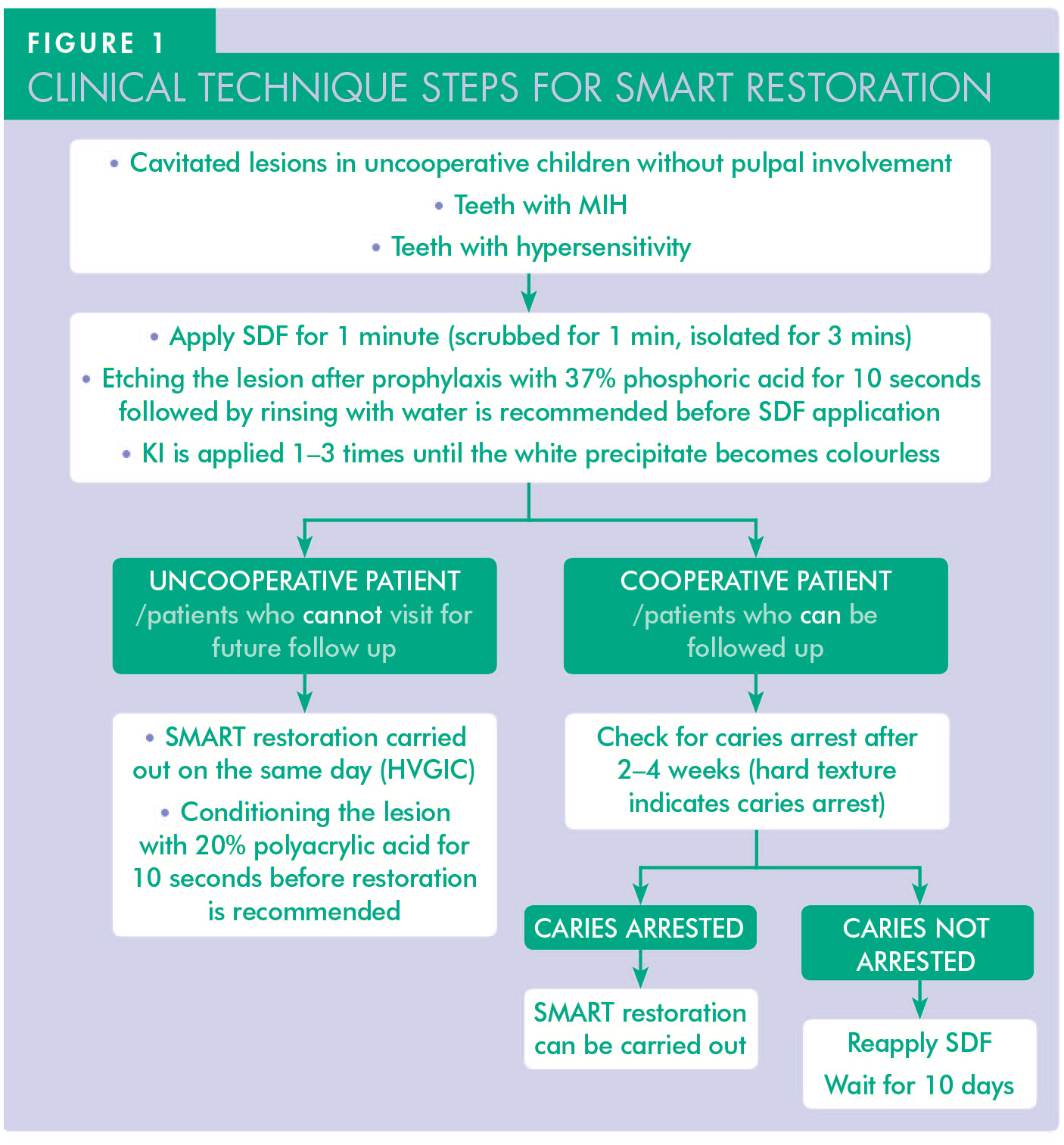
Single-visit SMART
GIC is placed in the cavity soon after SDF application. However, the restoration may turn grey, particularly if the restorative material is light-cured. The discolouration can be minimised by thoroughly debriding the cavity borders after SDF application before restoration with GIC. 25 The detailed description of the steps is as follows:
Petroleum jelly is applied to the surrounding gingiva and perioral areas to avoid unintentional staining of soft tissues due to SDF. 8
After isolation with cotton rolls, loose debris on the cavity surfaces is removed to improve the SDF’s contact with carious dentine. Carious dentine is not excavated except on the perimeter of the cavity with a spoon excavator to obtain clean cavity margins, improve the GIC bonding and minimise discolouration along the borders. 25
The lesion is washed with water and air-dried, then SDF is applied to the carious dentine for one minute using a micro brush. The application site is isolated for three minutes after the application. No fluoride varnish is applied over the SDF as it will interfere with the chemical bonding of GIC. 24
Additional steps during SDF application to enhance the action of the SDF and obtain better aesthetic results are: • Prior to SDF application, the lesion is etched with 37% phosphoric acid for 5–15 seconds, rinsed, and dried without desiccating the dentine. Etching facilitates smear layer removal and permeation of SDF into the dentinal tubules.
26
• After SDF, KI is applied to mask the colour. KI should be applied repeatedly (1–3 times) until the precipitate over the lesion becomes colourless.
8
Rinsing off the precipitate formed after KI application can improve the bond strength of GIC to dentine.
22
Alternatively, 20% glutathione can be mixed with equal amounts of SDF to reduce discolouration.
9
To remove the smear layer and activate the ion surface exchange, 20% polyacrylic acid is applied to the SDF-treated lesion for ten seconds, rinsed with water and blot dried to obtain a moist, glossy surface.8,24
Place a matrix and wedge for proximal cavities. GIC is mixed according to the manufacturer’s instructions and placed in the cavity with a plastic filling instrument, taking care not to form voids. 8
Adapt the restorative material quickly using the finger press technique; excess is carved and removed. During setting, GIC is protected from water loss or gain by application of the manufacturer’s resin coat or unfilled resin. 27
The patient is instructed not to chew on the side of SMART restorations for at least one to two hours (48 hours for more extensive restorations) or to consume a soft diet for two days. 24
Multi-visit SMART
Apply SDF once or multiple times based on lesion activity and size, then restore the affected area after a wait time of 2–4 weeks.24,28 During the interval, the surface microhardness of the lesion will increase. 26 The hard tooth surface upon probing, as opposed to the lesion’s black appearance, indicates the arrest of the lesion. 29 Reapplication should be considered in large carious lesions where the operator is unsure of complete arrest after one application. 30 Stained dentine in the marginal areas that would show through the restoration is removed, and the GIC restoration is completed in the same manner described in the single-visit technique. 23 The advantage of multi-visit over single-visit SMART is yet to be studied clinically.
HVGIC is the material of choice for SMART restorations due to its significant anticaries effect, and the finger press technique makes it easier to use than other materials. 19 Light-curable restorative materials are not recommended as they intensify the SDF staining further.8,31 The long-term release of fluoride ions from GIC supports remineralisation. 32 They can be “recharged” with ions from other sources, such as fluoride toothpaste. It has been demonstrated that GIC restorations are antibacterial and reduce the acidogenicity of biofilm due to fluoride release. 33
Bonding of SDF-treated dentine with restorative materials
Several in vitro studies have been conducted to assess the bond strength of various restorative materials to SDF-treated teeth. SDF does not influence the bonding of resin composite materials and GIC to sound dentine.5,26 However, results have been mixed when bonding to carious dentine. 5 Acid etching prior to the application of SDF is known to increase the permeability of SDF into the dentinal tubules, resulting in better caries arrest and increased dentine microhardness.26,34 Acid etching and KI application to mask discolouration do not affect the GIC bond strength to carious dentine.26,35
A systematic review on whether the application of SDF affects the bond strength of GIC to carious dentine concluded that the bonding of GIC was not affected. 36 GIC bonding is based on a chemical interaction between polyacrylic acid from glass ionomer and calcium ions from hydroxyapatite of the tooth structure. Prior application of SDF to the dentine surface causes silver deposits and silver oxide, improves GIC adhesion, as the material tends to bond to metal ions. Other reasons for better bonding are the formation of silver iodide precipitate when used with KI that blocks dentinal tubules, leading to better moisture control, and silver phosphate forming a bond with the carboxylic acid in the glass ionomer. 37 Application of SDF with glutathione is shown to have better bond strength than SDF+KI application, due to the ability of glutathione to improve collagen cross-linking and stabilisation of dentine. 9 Another systematic review was unable to make a definitive conclusion regarding the SDF application’s influence on the bond strength of GIC to dentine due to the large degree of diversity in SDF application methodologies. 38 Hence, there is a need to develop a standardised protocol for SDF application prior to restoration with the ART technique.
Effect on dentine remineralisation
Both GIC and SDF cause remineralisation of carious dentine. However, the increase in mineral density varies and occurs at different depth ranges, 39 which explains the potential for synergistic effects upon combined application. Following SDF application, the fluoride released forms calcium fluoride and fluorhydroxyapatite upon reacting with the dentine. Due to the availability of fluoride ions released by the glass ionomer, a more stable fluorapatite is formed. The combined application also increases the ratio of immobilised dentine phosphor-phoryn (DPP) to free DPP, which promotes remineralisation, leading to hypermineralisation of carious dentine. 40 Repeated applications of SDF up to two times at weekly intervals before the GIC restoration have been shown to enhance remineralisation. 28 However, the literature on long term combined SDF and GIC effects on dentine remineralisation is limited.
Indications for SMART restorations7,41
SMART restorations are indicated in the following:
patients who are lacking in cooperative ability for conventional cavity preparation and restoration such as: special needs and medically compromised patients patients who are highly anxious and fearful regarding dental treatment procedures very young children or pre-cooperative children, unable to cooperate due to emotional immaturity geriatric patients
management of dentinal hypersensitivity in molar incisor hypomineralisation (MIH)
SMART restorations, in conjunction with placement of preformed metal crowns using the Hall technique, can be a safer option for restoring carious lesions in children who would otherwise need treatment under general anesthesia. 42
Limitations of SMART restorations 42
SMART restorations have some limitations:
they cannot be used in carious lesions approaching pulp
there is a chance of transient gingival/soft tissue discolouration and irritation
they are a less aesthetic restoration due to staining by SDF
Parent/carer acceptability of SDF can be a factor while planning for SMART, as discolouration due to SDF application was acceptable to only 53% of parents in one study. 13 However, parental acceptance was better if it was for a posterior tooth, an uncooperative child, and during subsequent dental visits. 43 Hence, parental/carer education and obtaining informed consent before the procedure is important. 8
Clinical evidence on the effectiveness of SMART
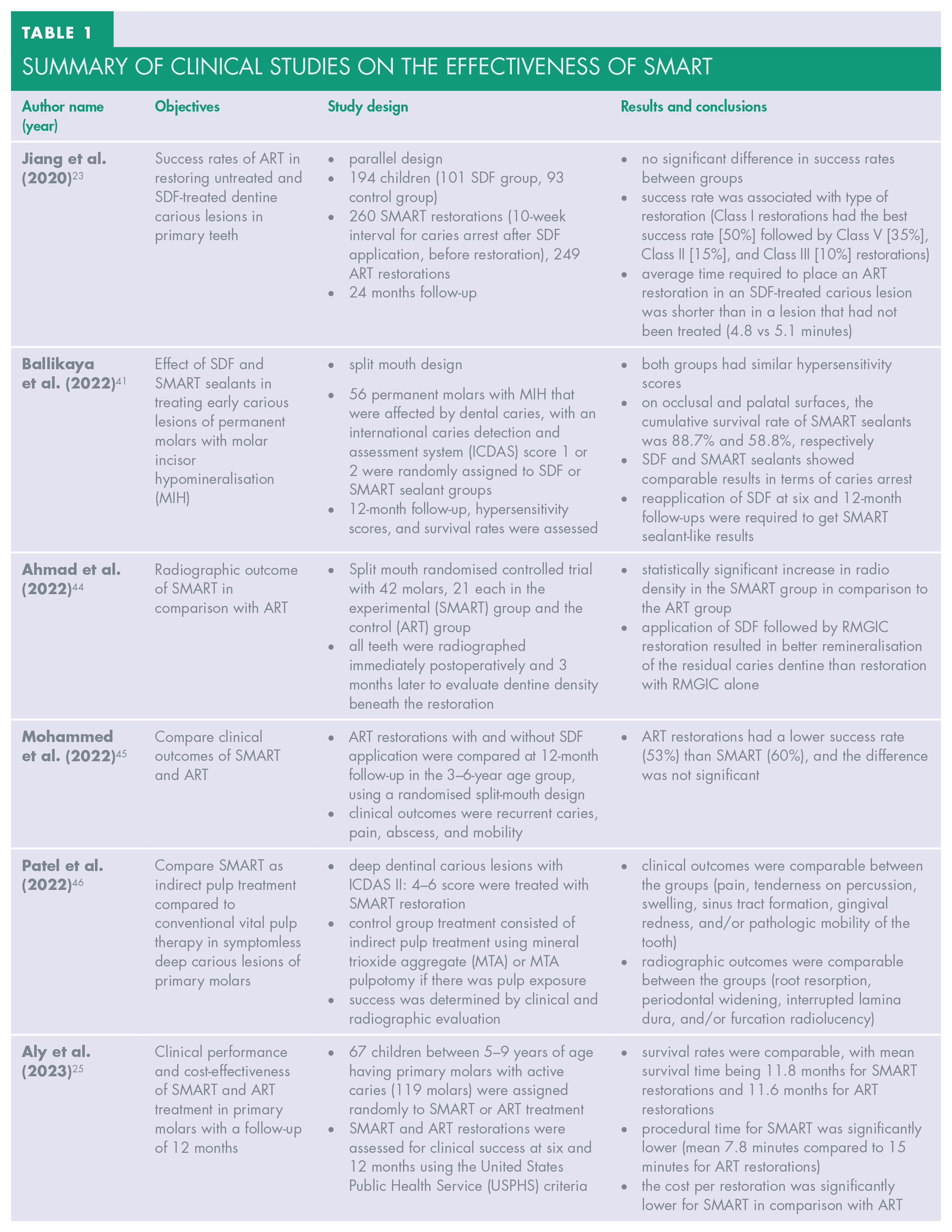
A summary of clinical studies from the literature is provided in Table 1. While two clinical trials reported no difference in success rate at two-year follow-up,26,28 radiographic evidence of better remineralisation 44 and evidence for better clinical success rate are also available. 45 Decreased restoration time and costs compared to ART have also been observed.26,28 More clinical evidence is required regarding the long-term effectiveness of SMART.
Summary of clinical studies on the effectiveness of SMART
Discussion
SMART is a modified application of the ART philosophy that permits utilising SDF to arrest carious lesions, eliminating the need for extensive caries removal. The cavity preparation is limited to obtaining clean margins with rotary or hand instruments before placing a restoration using GIC, thus deeming it minimally invasive. SMART has a combination of benefits, such as selective caries removal, cavity seal that chokes off nutrient sources for remaining bacteria, antibacterial action, desensitisation, remineralisation, and restoration of the anatomical form of the active cavitated carious lesions. Further clinical trials are needed to confirm the method’s long-term success in primary and permanent teeth. This concept requires a standardised clinical protocol. Clinical research on the masking effect of KI and glutathione on SDF staining and, hence, the aesthetic outcome of SMART is also warranted. The SMART concept can be beneficial in paediatric and geriatric dentistry to manage cavitated lesions.
Conclusion
SMART restoration effectively arrests caries without removing additional tooth structure, making it a promising option for dental caries management in individuals who lack cooperative ability. The technique masks the discolouration caused by SDF, making it a more aesthetic option than SDF application alone. Further clinical evidence on the benefits of single or multi-visit SMART restoration can lead to incorporating SMART as a patient-friendly technique in routine dental practice. It is necessary to develop a standardised protocol for the technique so that the results of the clinical studies are comparable.
Footnotes
Declaration of Conflicting Interests
The Authors declare that there is no conflict of interest.