
Abstract
The aim of this paper is to provide dental professionals with insight into how the science of behaviour change can be used to support patients to change their oral health behaviours. The paper describes how the fourth version of Delivering Better Oral Health (DBOHv4) published in November 2021, brings together the theory plus key principles and practical tools in Chapter 3 “Behaviour change”, to help front-line clinicians achieve the best effect. DBOH is freely available to all online at
Learning Objectives
To consider how behaviours during day-to-day life influence health and oral health
To review the contemporary evidence on behaviour change
To provide practical advice on how this evidence may be used by dental professionals to support patients to change their behaviours
Introduction
How healthy is your lifestyle?
Let’s start considering our own health. If someone asked you for top tips on keeping healthy, what would you suggest? What risk or protective factors would you include? Would you have listed everything in Table 1 for health in general?
Healthy behaviours for adults: general guidance on self-care
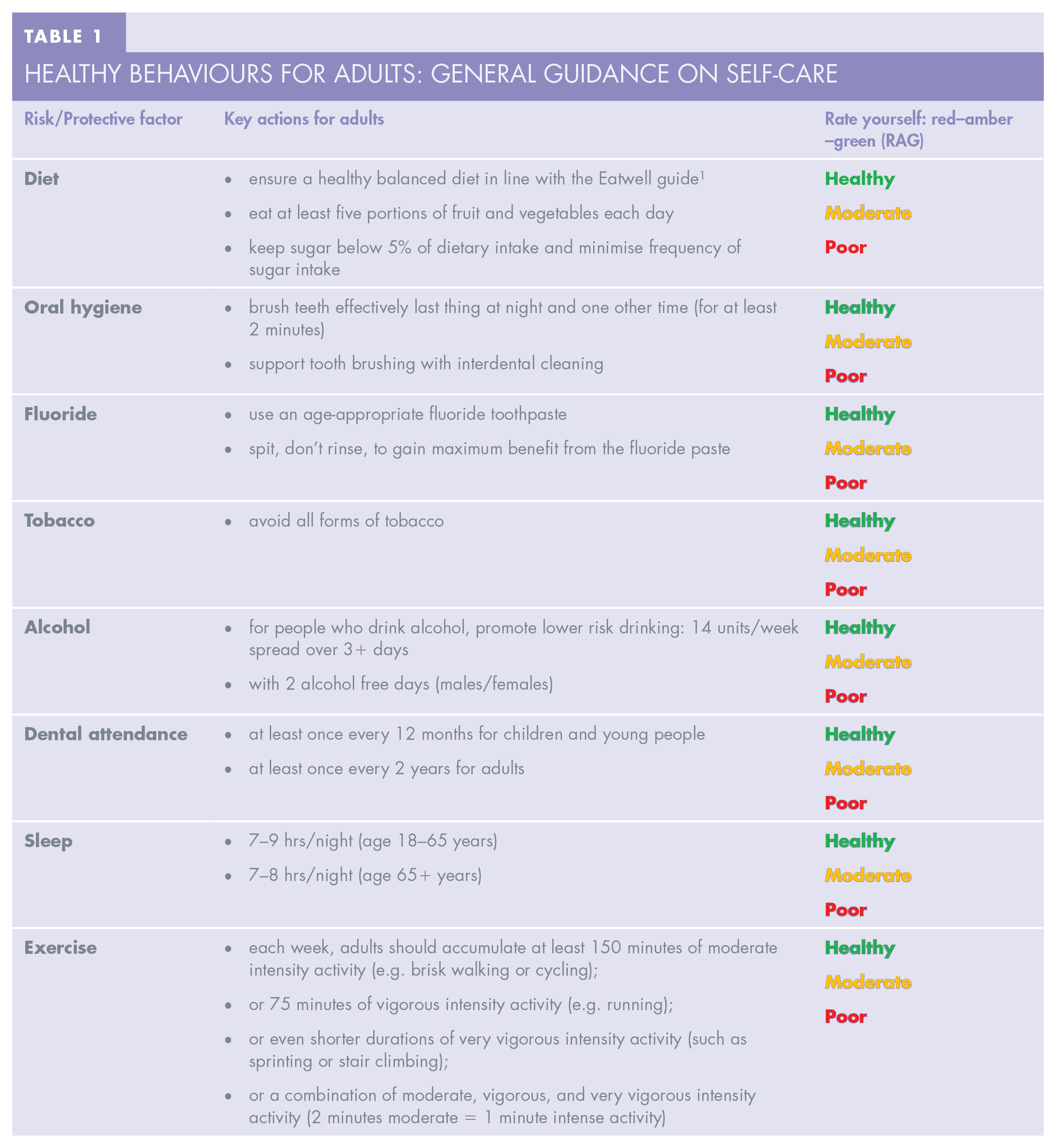
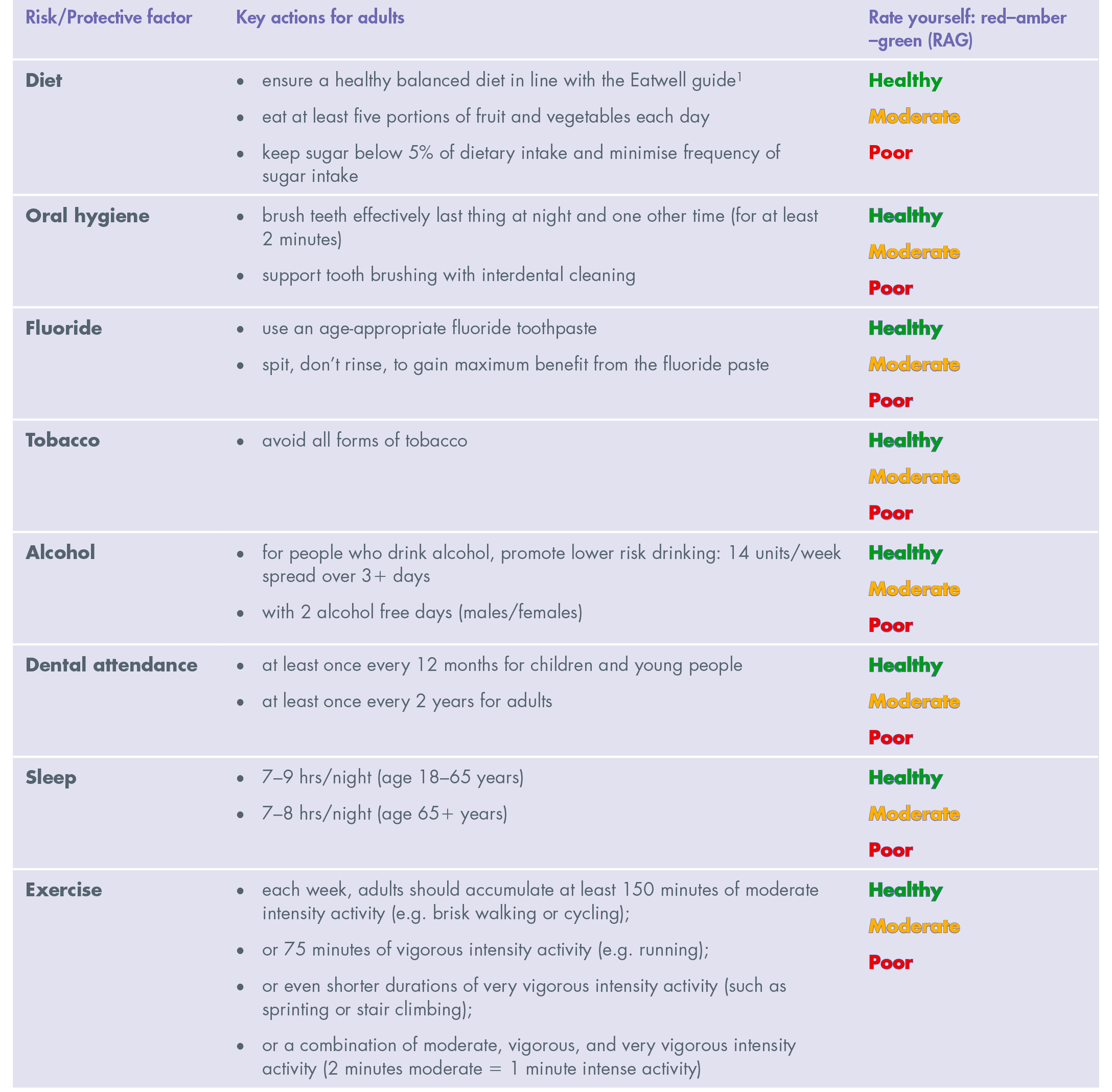
OK now, try rating yourself – red (poor), amber (moderate), green (healthy) (RAG). Be honest about whether it is part of your general lifestyle or just on an occasional “good day”.
So, where have you scored yourself “green”? Was it a behaviour you’ve maintained for years or something you’ve worked on recently? What helped you achieve and sustain it?
Where have you scored yourself as “red”? Why does this behaviour prove so difficult for you? How were you influenced by the environment you live and work in? Pressure or support from friends and family? Or advice from health professionals?
Patients face the same issues; and for many patients who may be living with more challenging circumstances these issues are magnified. People’s ability to change their behaviours are influenced by individual, social and environmental factors, with socio-economic circumstances being a major factor. We also know that the ability to change varies at different times in people’s lives. Even though we recognise how hard it can be changing our own behaviours, as dental professionals we can still feel dispirited when patients don’t change, despite our best attempts!
Contemporary behavioural science is providing us with insights into behaviour change 2 which can be invaluable to dental professionals who are working to improve and maintain patients’ oral health. Delivering Better Oral Health: an evidence-based toolkit for prevention (DBOHv4), 3 updated in November 2021, includes a chapter which applies this theory in more detail (Chapter 3: Behaviour change). 4 Version 4 involved a complete revision of the guidance in line with contemporary methodology,5,6 and a published approach 7 involving over 100 experts. The group responsible for producing DBOH, comprising national leaders of dentistry, were strongly convinced that behaviour change was so important that it required a place “up front” in the guidance document, just after the key summary guidelines in Chapter 2.
The following section of this paper summarises recent guidance on behaviour change as described in Chapter 3 of DBOH. 4
How to help patients change their oral health behaviours
Changing behaviour should be considered as a cycle, a process, not a one-off event (Figure 1). 4 Patients may be unaware of an issue, or they may have been thinking of making a change and actively planning to do so, or even have enacted change and are trying to maintain a new healthy behaviour. This is not a linear process and behaviour change may involve several attempts, so it is helpful to identify where your patient is currently and start there. Following a full patient assessment, key oral health behaviours which a patient ideally needs to tackle will be known. There may be several, so the authors suggest that you do not try to address every behaviour at once but allow yourself to be guided by your patient, based on what they feel is possible in their current circumstances and what is important to them.
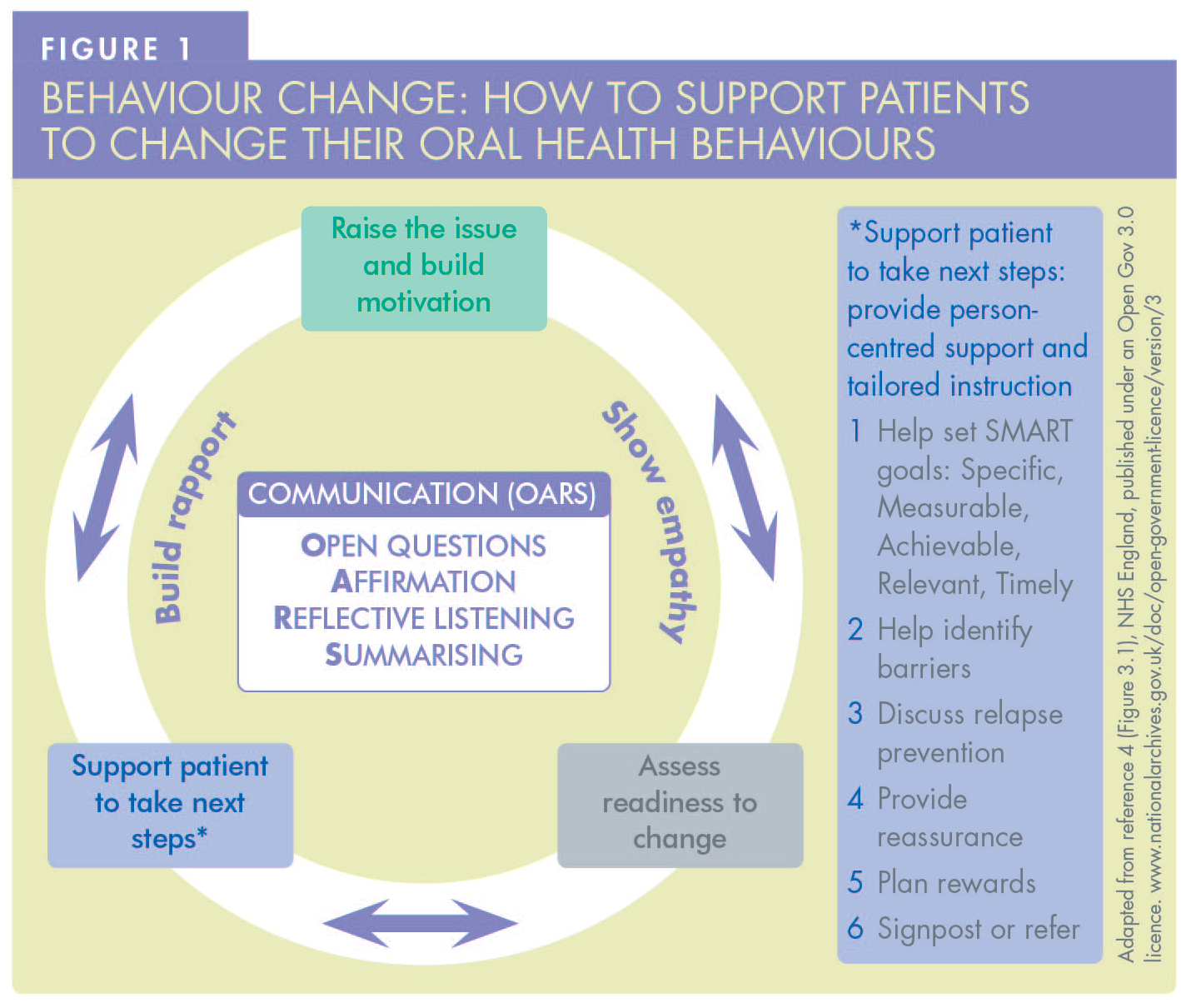
Raise the issue and build motivation
A dental professional can helpfully start a conversation by providing information about a particular behaviour to be prioritised and its link to oral and general health. They can attempt to build the patient’s motivation to change by highlighting the specific benefits of making the change for that patient. It is important to provide this information while recognising that knowledge alone is generally insufficient to bring about an actual change in behaviour.
Assess readiness to change
It is then important to assess whether the patient is ready to take the necessary action. Patients may express “resistance to change” if they feel it is too difficult or not the right time for them, particularly if they are facing stressful circumstances. If the patient shows signs of reluctance, try to keep the opportunity for further discussions at a future appointment open rather than trying to be persuasive and coming across as judgemental. If the patient feels ready to make a change, move onto the next step of providing support.
Support patients
If a patient chooses and agrees to make a change, a dental professional can support them in several practical ways (Figure 1). These may include providing person-specific advice and setting SMART goals that are specific, measurable, achievable, relevant, and timely (Table 2). Accepting that behaviour change is not linear, it is helpful to discuss potential barriers the patients foresee and what to do to overcome them. Support helpfully includes encouragement and praise at subsequent appointments to make it a positive experience. For some oral health behaviours, additional support can be provided in the form of signposting to specific tools or services.
Behaviour change tools
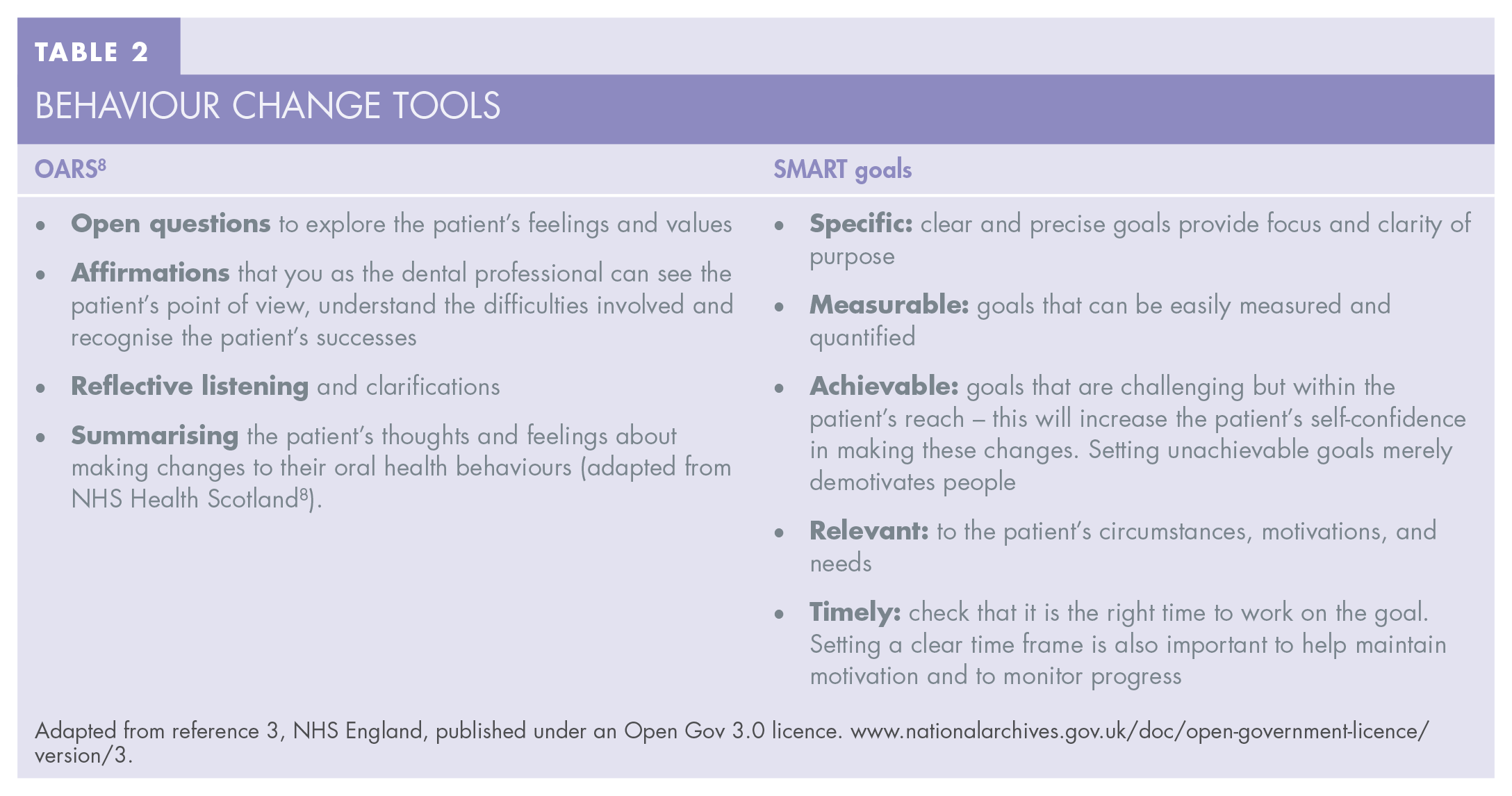
Adapted from reference 3, NHS England, published under an Open Gov 3.0 licence. www.nationalarchives.gov.uk/doc/open-government-licence/version/3.
Communication is key
Good communication skills are an essential component of this behaviour change process. This includes building rapport and empathy and using some specific techniques from the acronym OARS (Table 2), using
Chapter 3 of DBOH includes patient case studies which highlight three common scenarios (Figure 2). 9 Each one shows how using the process described above, with communication techniques based on OARS, you can raise the issue and build motivation, assess readiness to change, and support patients to take the next step.
Tools for behaviour change
The process described above provides some general principles for behaviour change, but in DBOH some specific oral health behaviour change interventions are also listed in the DBOH section headed “Resources”. 4 They cover the following areas:
oral hygiene for plaque removal in adults
behaviour change conversations with parents/carers of young children to promote supervision of tooth brushing with a fluoride toothpaste
reducing sugar as part of a healthier diet
tobacco – very brief advice pathway for smoking
alcohol – identification and brief advice.
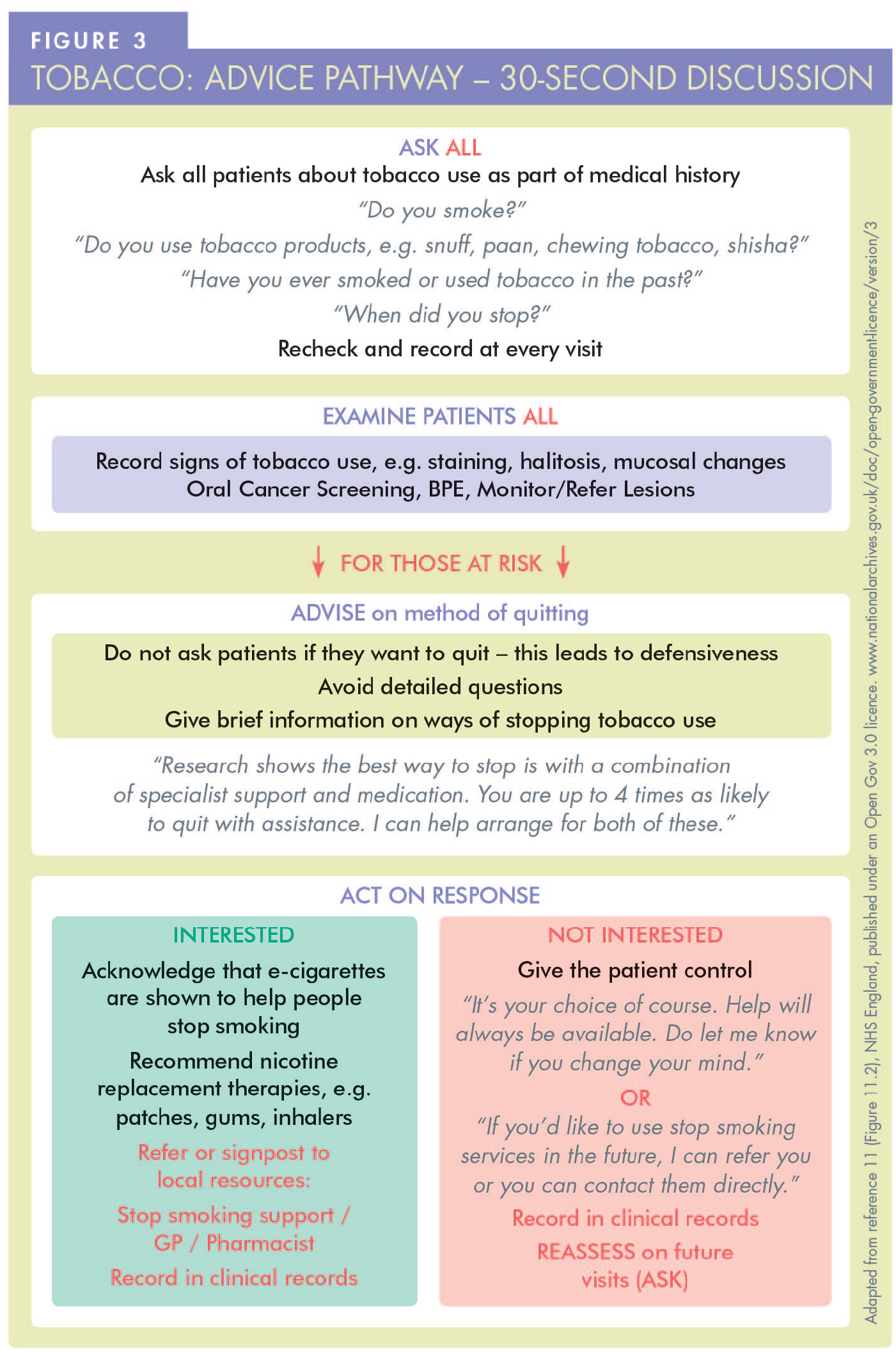
As demonstrated by some of the interventions listed above, very little time is needed. For example, very brief interventions for tobacco use from a dental team member have been shown to increase motivation and double the success of quitting. 10 This can take only 30 seconds if the careful script outlined in Chapter 11 of DBOH is used (see Figure 3). 11
To implement an ethos of behaviour change more generally in your practice, there are other resources you may consider. Dental teams can provide a supportive environment using digital technology via the practice website linking to tools, apps, and videos. In addition, the practice itself can provide breastfeeding-friendly facilities and can support campaigns such as National Smile Month, Mouth Cancer Action month, Stoptober, and Dry January. This all contributes to “Making Every Contact Count for Health”. 12 The authors trust that you will find DBOH a valuable tool in delivering high quality contemporary care for your patients and perhaps yourself.
While many of these interventions are relatively quick and the use of a skill mix can help, it must be acknowledged, however, that not all dental practices will find it easy to do so immediately. This need to implement behaviour change interventions comes at a time when delivering dental care, particularly NHS care, is more demanding than ever for dental practices. Potentially, practices which are well staffed with a range of dental team members, enjoy flexible facilities and can amend charges to cover the time involved, through operating in the private sector can adapt quickly. Under the pressure of managing NHS contracts, other practices may find it easier to take a team approach to the delivery of behaviour change. In contrast, others may not have dental nurses trained with extended skills in health education and fluoride application, or dental hygienists or therapists who can deliver all aspects of preventive care. While much of this doesn’t need to take place in a dental chair, some practices just don’t have the space for such consultations outside of the surgery, unless perhaps they can harness digital technology or expand their facilities. Practices with high demand for urgent care may find that there is little time to prioritise preventive care and support behaviour change, and yet face the realisation that if they don’t do so, their patients remain at similar risk of future disease. Thus, if the focus on prevention promised by policy makers is to become reality in the NHS sector, contract reform must reward the practices who invest their efforts on improving their patients’ oral health using these contemporary evidence-based tools. This should include the opportunity to train and develop staff, invest time in prevention to deliver better longer-term outcomes, and test innovative solutions to deliver preventive care which embraces behaviour change.
Conclusion
Supporting patients to improve their oral health behaviours is an essential part of every dental professional’s role and should be part of regular patient care. Supporting behaviour change can be challenging and time intensive, but with the application of behavioural science techniques we can ensure that the most effective approaches are used and time is spent wisely. While DBOH includes a list of useful quality-assured resources, publications, and training programmes, we know there are some behaviours, including sugar reduction, where current resources are scarce and future work is needed.
Footnotes
Acknowledgements
The authors would like to acknowledge all those who contributed to version 4 of Delivering Better Oral Health and endorse this guidance, together with UK.GOV for use of the images adapted in this paper.