
Abstract
Objective:
To investigate factors which influence UK general dental practitioners (GDPs) when restoring posterior root filled teeth.
Method:
An electronic survey was designed to explore current strategies of treatment of posterior root filled teeth by UK-based GDPs working in primary care. Three vignette cases included in the questionnaire explored a variety of tooth, patient, and financial factors. The survey was distributed by email and social media platforms between December 2018 and February 2019.
Results:
A total of 528 valid responses were collected. The majority of participants (84.1%) regularly restored posterior root filled teeth with an indirect restoration. Presence of persistent symptoms post root canal treatment (RCT) completion would impact the management of 85% of the surveyed respondents. Referral to a specialist, deferral of provision of the definitive restoration, and fear of litigation were reported by the GDPs as influencing factors.
Conclusion:
This survey highlights that decision making regarding restoration of root filled teeth is a multifactorial process. Tooth, patient, and financial factors were all shown to influence the restorative management of the posterior root filled teeth.
Learning Objectives
To explore different restorative challenges faced by general dental practitioners by using a vignette survey
To determine the factors influencing general dental practitioners when restoring root filled teeth
To understand how dentists’ experience, fee structure and location influences restorative management of root filled teeth
Introduction
Root canal treatment (RCT) in the UK is predominantly provided by general dental practitioners (GDPs), with over 500,000 endodontic treatments completed annually in the NHS alone (pre COVID-19 pandemic 2018/2019). 1 A large proportion of root filled teeth usually present with significant loss of coronal tooth structure due to existing restorations and caries. Literature has shown that a higher quality of coronal restoration results in better outcomes by generating less periapical inflammation when compared with high quality endodontic treatment alone.2-4 It is therefore vital to provide a suitable coronal restoration on a root filled tooth, to increase endodontic success rates. Multiple cross-sectional surveys investigated dentists’ opinions and understanding of restoration of root filled teeth.5-8 However, these mainly focused on provision of posts and the information was obtained with closed-ended multiple choice questions, collecting limited information.
A recent systematic review by Bhuva et al. 9 reported better long-term survival outcomes for posterior root filled teeth restored with indirect cuspal coverage restorations, when compared with those restored with direct restorations. It has also been shown that multiple factors affect long term survival of root treated teeth, such as the amount of residual tooth structure left, presence of marginal ridges and tooth location.
In the UK there is currently limited data on what factors affect a dentist’s decision-making process when restoring posterior root filled teeth. Research is also lacking on the cost of endodontic treatment and how a patient’s paying status affects the choice of restoration they receive. The aim of this study was to explore and identify the factors which GDPs may take into consideration when restoring a posterior root filled tooth.
Methods
This study was a cross-sectional observational electronic survey with a 33-item questionnaire designed and hosted with Qualtrics XM 2018 (Qualtrics, Provo, UT, USA). The survey allowed answers in formats such as text entry, multiple choice, or a drop-down menu of options. Ethical approval was granted in from the University of Liverpool in 2018 (Ethics number 3921).
Following sample size calculation based on the number of dentists recorded on the General Dental Council (GDC) register, a target sample size of 381 was calculated to achieve 95% confidence interval with a margin of error of 5%. The sample size was calculated to ensure an accurate representation of GDPs. The authors’ primary aim was to investigate the factors in GDP decision making. Statistical trends were not considered in this study.
The survey was distributed by contacting GDPs working in general practice in the UK by email, and through posts on dental social media pages. The correspondence contained a copy of the invitation letter and a link for dentists to complete the survey. The collected research data were treated as confidential. The identification of the participants was anonymised. No names were collected, nor the email addresses stored. The survey was distributed from December 2018 to February 2019. Consent to take part in the study and use of the data collected for research purposes was obtained from all participants.
The survey was divided into two sections, with the first part collecting general demographic information of the GDPs. The second part of the survey consisted of three case vignettes, where a photograph of a root filled tooth was shown, accompanied by a clinical scenario. The questions related to the management of the root filled tooth. The vignette cases presented included several restorative options available for the GDPs to choose from. Direct restoration options included composite, amalgam, and glass ionomer. Indirect restoration options included metal ceramic crown, ceramic crown, metal crown, metal onlay, ceramic onlay, and composite onlay. The results were grouped into their respective categories to facilitate ease of presentation and comparison.
Descriptive statistics were used to summarise numerical data such as the distribution and participant characteristics of the study sample. Free text box answers were analysed for their answers until saturation.
Results
The total number of responses was 528, with 479 responses collected using the social media link. The remaining 49 responses were collected by email.
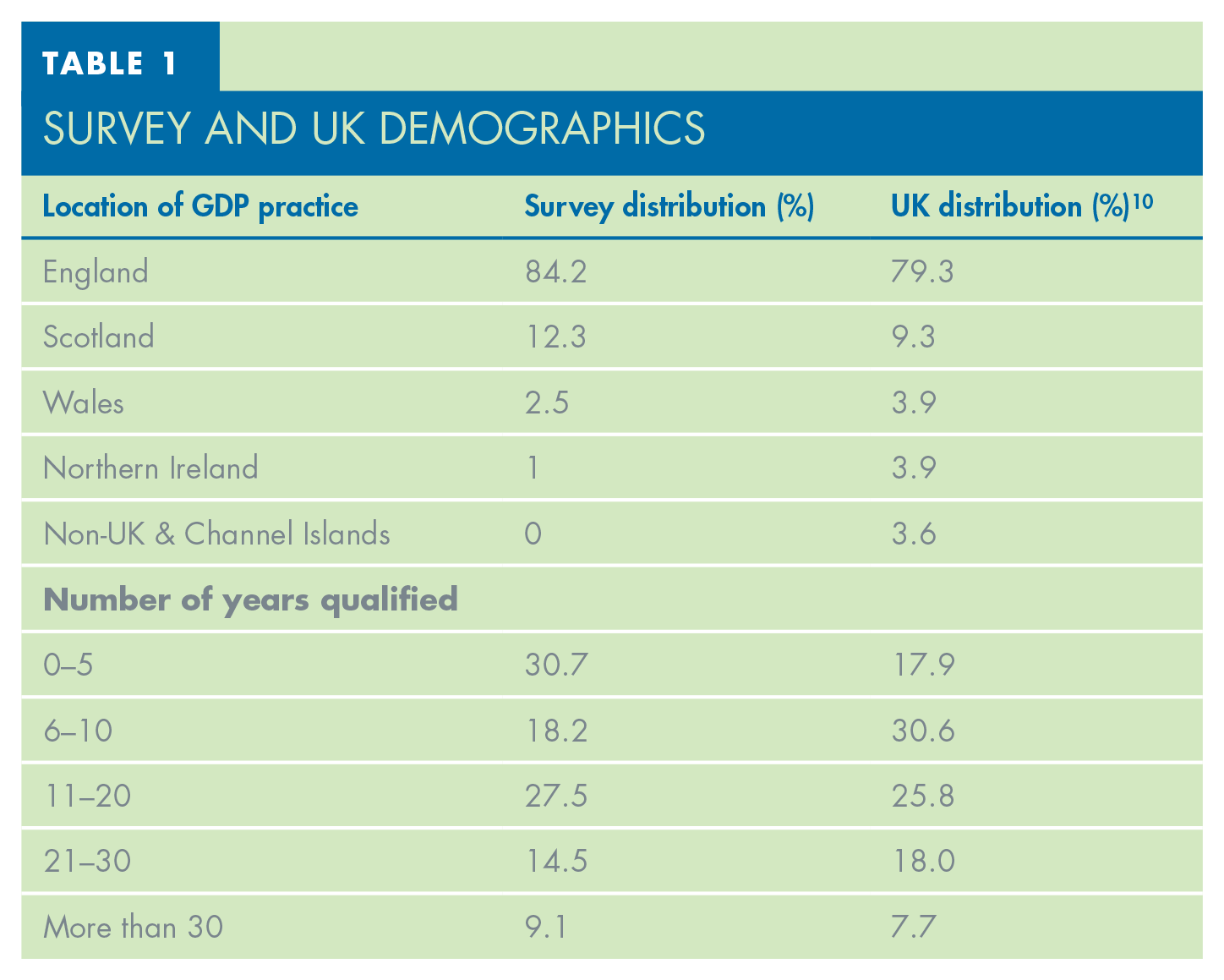
The demographics of the survey respondents can be seen in Tables 1 and 2. The majority practised in England (84.2%), followed by Scotland (12.3%), Wales (2.5%), and Northern Ireland (1%). This closely matches the GDC reported figures of UK GDPs. 10 The age of the survey participants shows a similar pattern, however a greater proportion of younger dentists participated in the survey compared to the UK demographic data. 10 Most respondents worked in full NHS practice (33.6%), followed closely by fully private practice (31.7%) and mixed NHS/private (30.4%).
Survey and UK Demographics
Summary of Demographics of Participating Clinicians
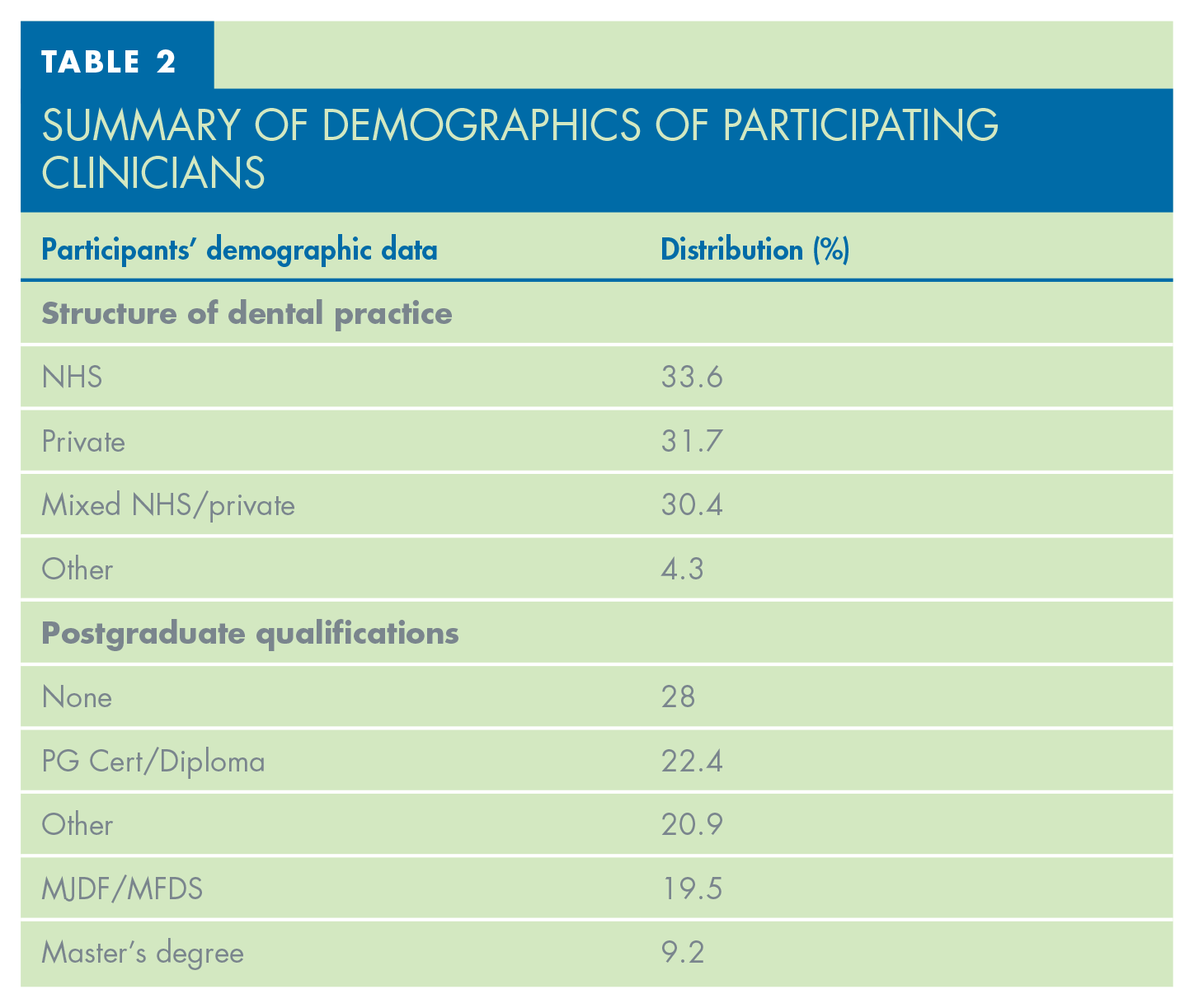
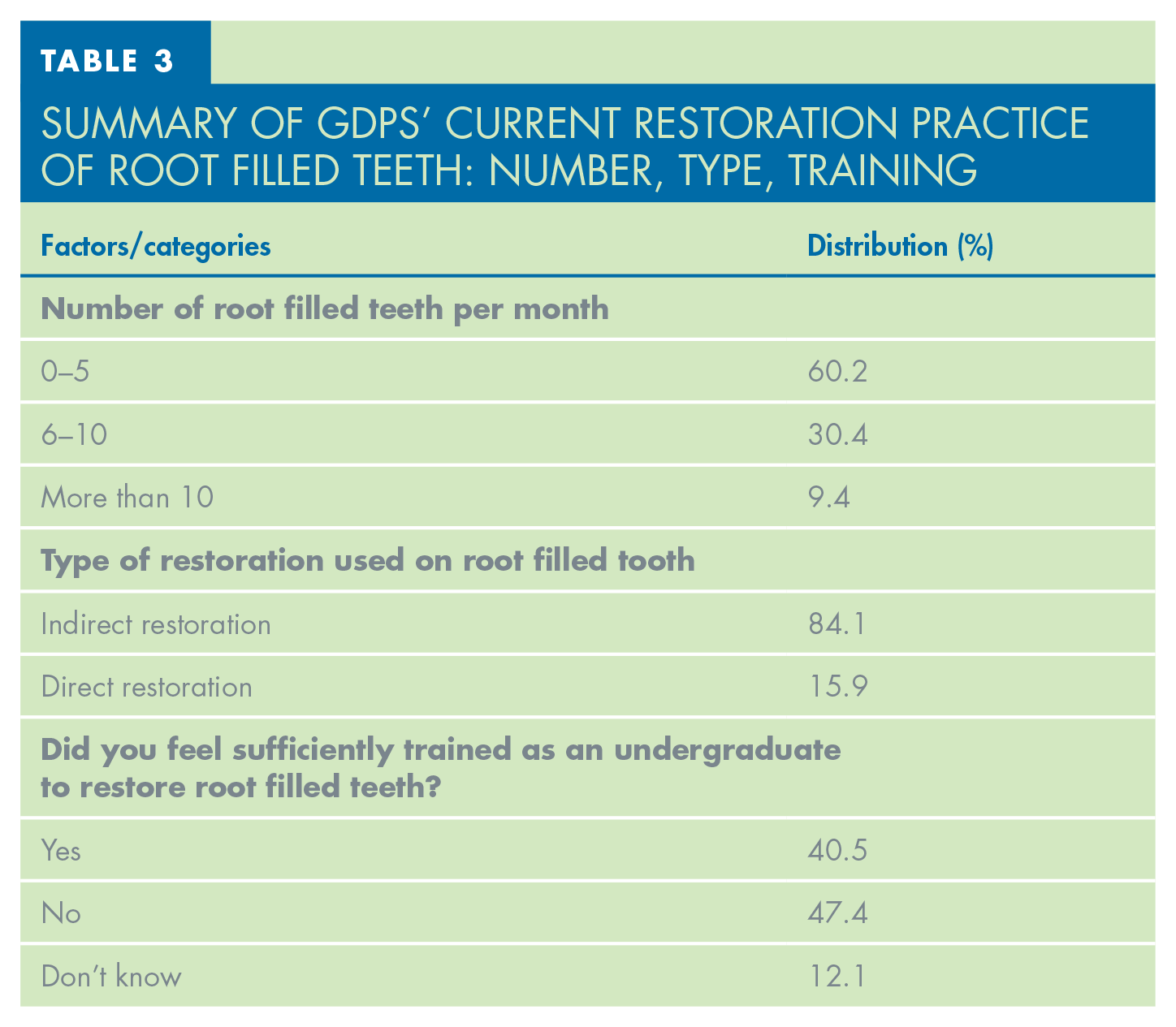
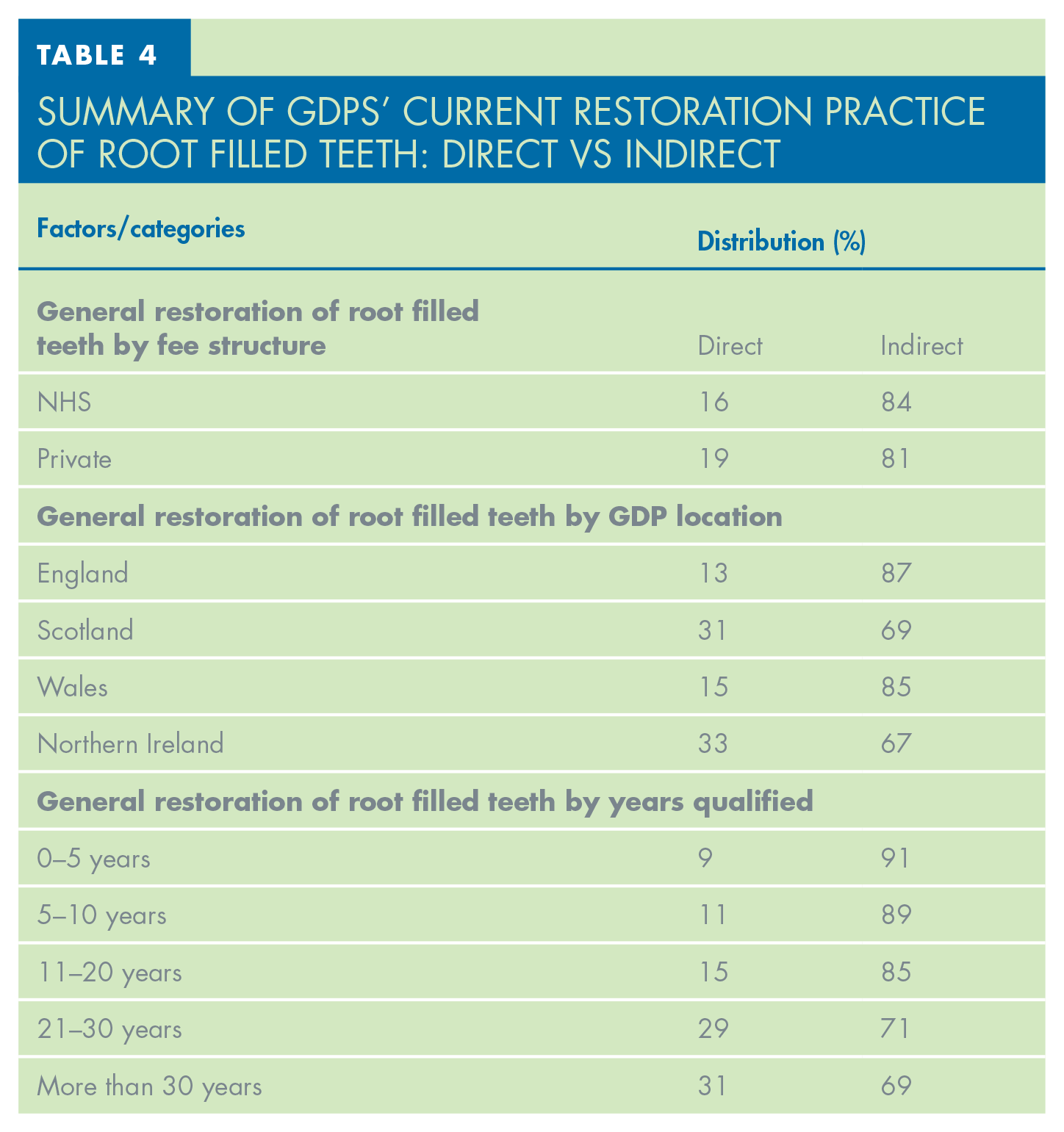
Table 3 outlines the summary of GDP’s current restoration practice of root filled teeth, showing that 60.2% of GDPs restored between 0–5 root filled teeth per month. Indirect restorations were most utilised by GDPs to restore root filled teeth, with 84.1% of respondents choosing this option. Table 4 showcases the trends of GDP restoration practices by years qualified, fee structure, and location. Both NHS and private GDPs choose to use indirect restorations in over 80% of cases when restoring root filled teeth. The reported restorative practice of more experienced GDPs shows that they are less likely to opt for an indirect restoration; only 69% of GDPs with over 30 years of experience choose an indirect approach compared to the 84% overall average.
Summary of GDPS’ Current Restoration Practice of Root Filled Teeth: Number, Type, Training
Summary of GDPS’ Current Restoration Practice of Root Filled Teeth: Direct vs Indirect
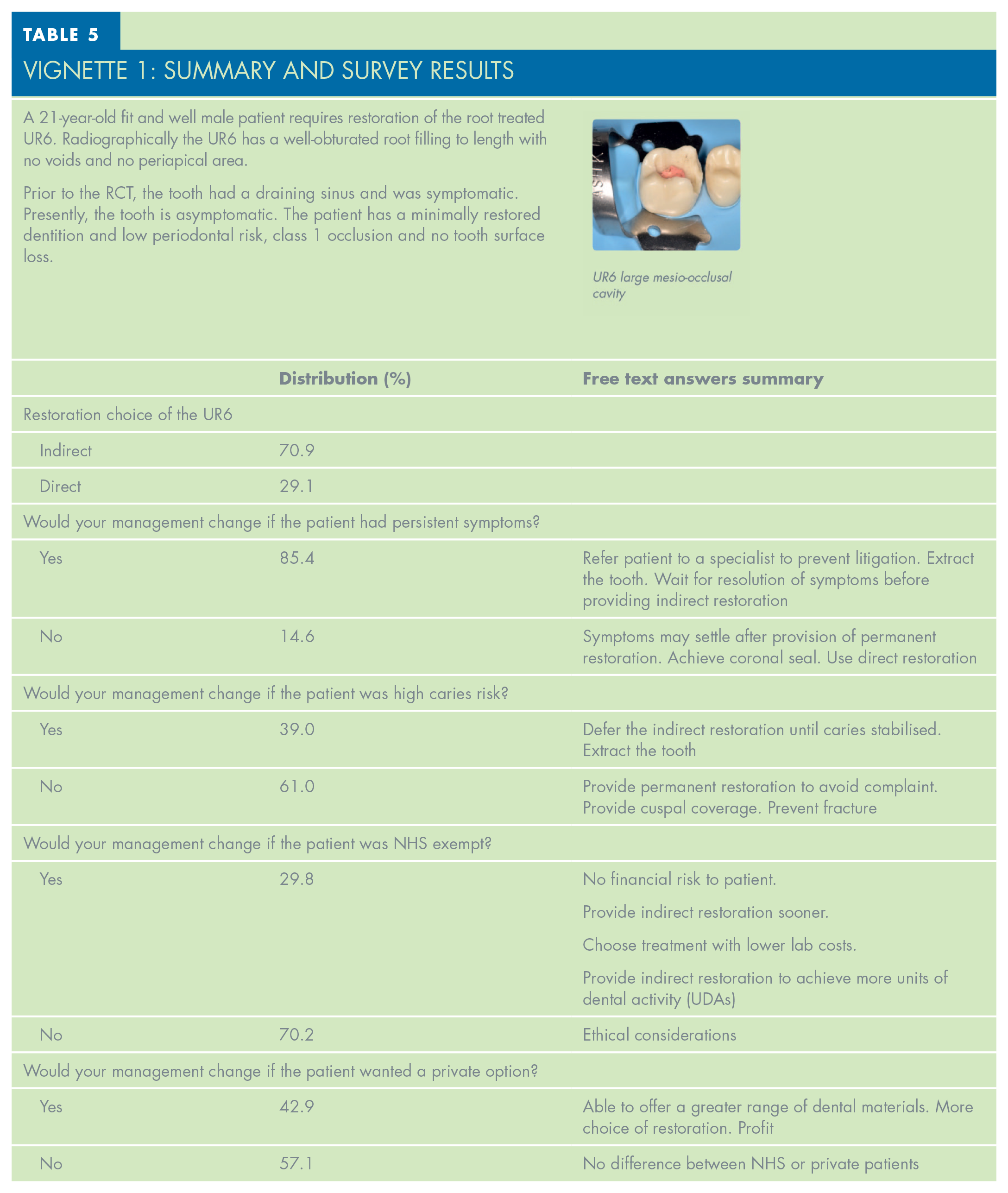
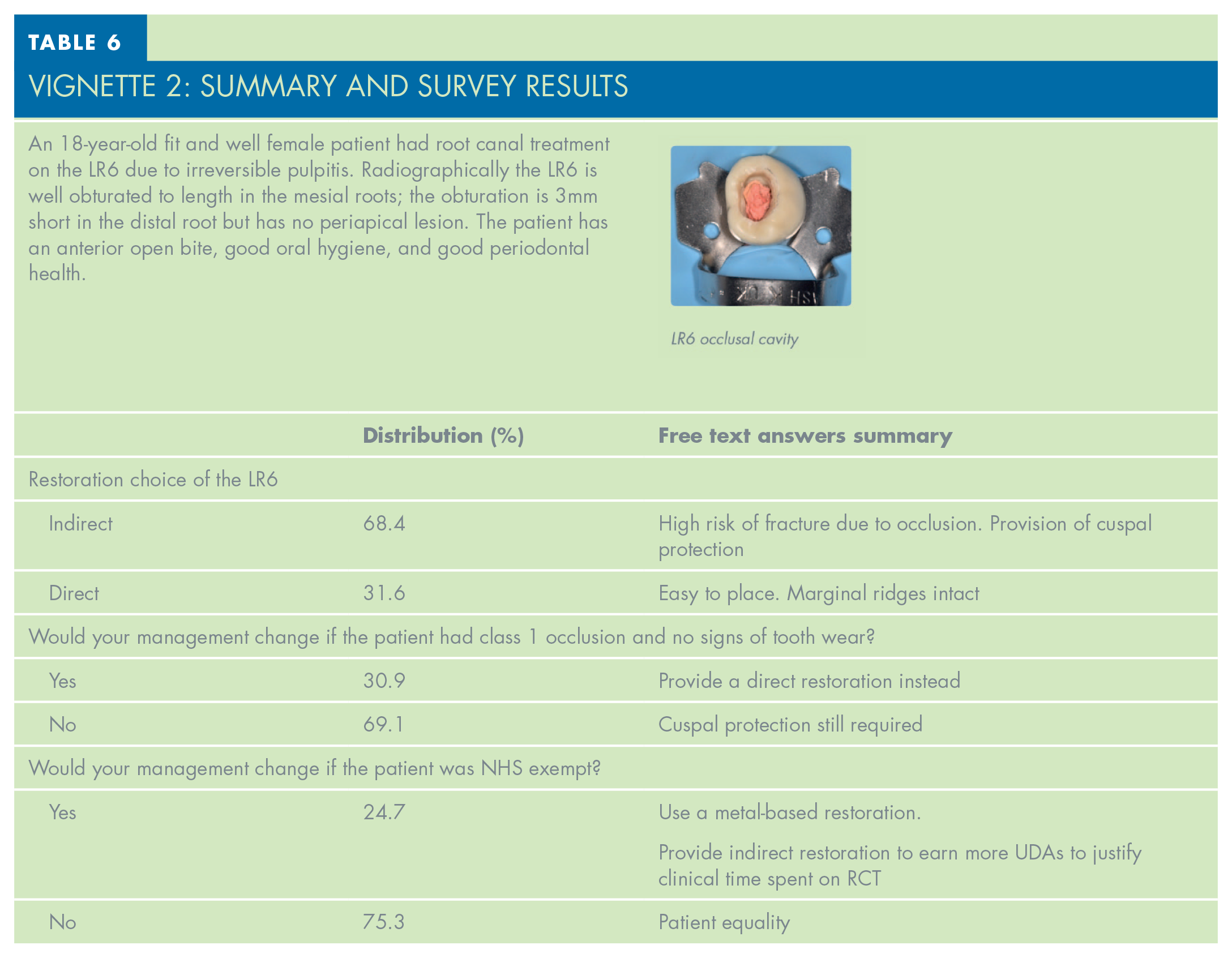
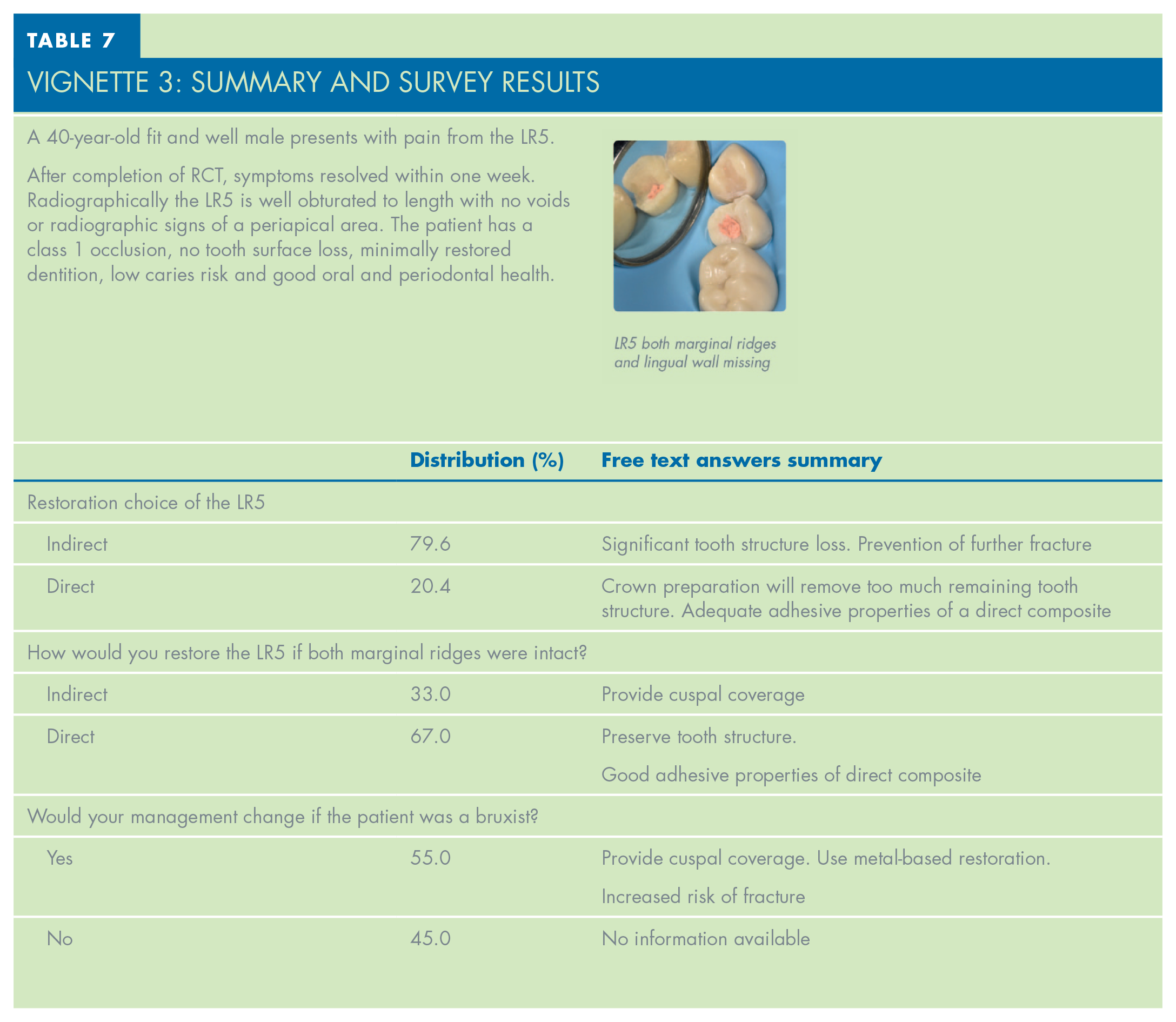
The three vignette cases and associated summaries of the responses are presented in Tables 5, 6 and 7.
VIGNETTE 1: Summary and Survey Results
VIGNETTE 2: Summary and Survey Results
VIGNETTE 3: Summary and Survey Results
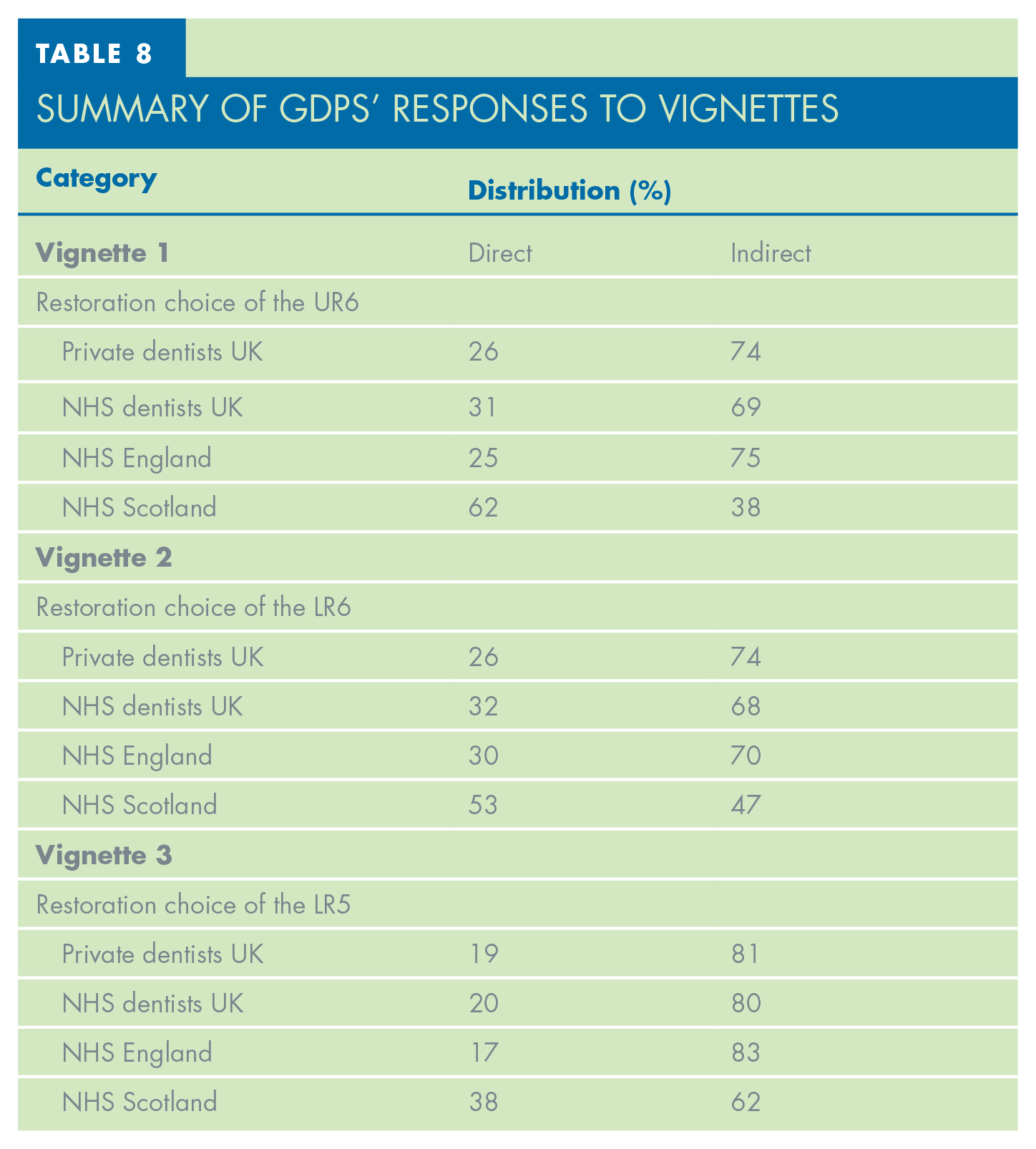
Additional analysis of responses to the vignettes by fee structure and region is shown in Table 8. It indicates that GDPs from both NHS and private practices restore root filled teeth similarly, however private dentists prefer using indirect restorations which can be seen across all three vignettes. The collected data also shows that Scottish NHS dentists are far more likely to use direct restorative approaches in all vignette cases.
Summary of GDPS’ Responses to Vignettes
Discussion
General restoration trends
The general trends of restoration of root filled teeth by GDPs, which were shown in Table 4, are discussed below.
The GDP fee structure did not show significant differences in both general restorative approaches and vignette responses. Both NHS and private GDPs opted for an indirect restorative approach by at least 68% of surveyed practitioners in all three vignette cases. Private dentists chose the indirect restorative approaches more frequently compared to their NHS colleagues, which these authors suspect reflects greater clinical freedom and different patient demographics.
Location of the GDPs was also shown to affect the choice of restoration type. Strong trends in general use of direct restorative materials to restore endodontically treated teeth were identified in GDPs from Scotland and Northern Ireland. Responses to the vignette cases from Scottish NHS GDPs further confirmed the preference of direct restorative approach in this region. Compared to the rest of the surveyed population, this shift could be a result of the Scottish NHS remuneration structure or demographics of the treated patients, which have been shown to have an impact on treatment decision making. 11 However, very low sample size was available on the NHS Scotland GDPs so the data need to be interpreted with caution.
Postgraduate experience of the GDPs showed a clear trend in older and experienced GDPs opting for direct restorative approaches more often, when restoring root filled teeth. This may be a result of differences in approaches taught during their BDS degree, with recent graduates being encouraged to use indirect restorations when restoring root filled teeth. Despite the GDC’s compulsory continuing professional development (CPD) requirements, restorative dentistry CPD is not mandatory. 12 Consequently, it’s possible that this is one of the main reasons for the disparities in restoration trends that are evident in the data.
Experienced dentists may also be more confident in their abilities and likely to employ direct restorative materials more predictably, in comparison to their younger colleagues.
The vignettes were designed to explore how different factors influence GDPs’ restorative management of the root filled teeth. These include tooth, patient, and financial factors and are discussed below.
Tooth related factors
Vignettes 1 and 3 both feature teeth which have lost their marginal ridges. Mondelli et al. 11 have suggested that the loss of marginal ridges weakens the tooth, with a mesio-occlusal restoration reducing stiffness by as much as 63%. 13 The majority of GDPs in this survey chose to use an indirect cuspal coverage restoration to restore posterior root filled teeth, which reflects the findings seen in other studies.14,15 Current evidence regarding restoration of posterior root filled teeth is conflicting, which can explain the variety of responses collected in this survey. Systematic reviews by Bhuva et al. and Stavropoulou and Koidis report an increased survival rate of indirectly restored root treated teeth, compared to use of a direct restorative approach.9,16 However, a review by Sequeira-Byron et al. 17 states that there is not currently enough evidence to recommend the use of an indirect restoration to restore a root filled tooth.
Bruxist patients often present with tooth wear and are at higher risk of tooth and restoration fracture. This is especially relevant in root treated teeth due to the increased amount of force applied on chewing motions and reduction in periodontal ligament (PDL) proprioception. 18 This topic was explored in Vignette 3, with 79.6% of GDPs choosing to restore the LR5 with an indirect restoration. Evidence of bruxism would alter the management of 55% of the surveyed practitioners. This was mainly due to a provision of a metal cuspal coverage restoration instead of porcelain, due to higher fracture and wear resistance.
Patient factors
The provision of an indirect coronal restoration can be influenced by the caries risk status of the patient, which was explored in Vignette 1. Patients with a high rate of caries are likely to develop secondary caries, subsequently leading to restoration failure. Therefore, it is advised that more complex treatment such as indirect restorations should be deferred until the caries rate has reduced and no new carious lesions are present. 19 In Vignette 1, only 39% of the surveyed GDPs would choose to change their management in a high caries risk patient, by deferring the provision of the definitive restoration or extracting the tooth. The remaining practitioners stated that the need to achieve a good coronal seal and risk of complaint due to incomplete treatment would influence them to restore the tooth as planned.
Litigation has now become more common in general dental practice, ranging from contractual disputes to patient complaints. 20 In comparison with other health professions, GDPs regularly undertake multiple high-risk operative procedures, which may place them at an increased risk of litigation. The majority of the surveyed participants (85.4%) would alter their management of the UR6 in Vignette 1 if the patient had persistent symptoms after the RCT. The survey responses indicated that, to minimise the risk to the GDP, referral to a specialist for a second opinion or ruling out non-odontogenic pain as an alternative underlying cause were suggested as effective measures. According to Nixdorf et al., it is not unusual for non-odontogenic pain to occur as a result of root canal therapy, and it could account for up to 50% of all cases of persistent tooth pain. 21 However, the prevalence of post-operative pain after RCT completion is well documented 22 and therefore a small proportion of GDPs chose to prioritise achieving a good coronal seal with a permanent restoration. This decision could be driven by research which shows that delaying the definitive restoration can allow more leakage of bacteria back into the root canal system, which can influence the apical periodontal health post RCT completion. 2
The survey also explored how GDPs would approach restoring an asymptomatic LR6 which presented with an obturation which is 3mm short in the distal root. Ng et al. have shown that root fillings which extend less than 2mm from the radiographic apex, have a higher chance of failure. 3 Despite this, around 34% of dentists, would prefer to restore the LR6 immediately after obturation, with equal numbers of private and NHS practitioners choosing this option.
Financial factors
Lumley et al. have shown that patients’ NHS paying status can influence RCT survival rates, with exempt patients having poorer survival rates than patients who pay full NHS charges for their treatment. 23 Exempt patients are also more likely to have lower socio-economic status and present with higher treatment needs. 24 Taking these factors into consideration, Vignettes 1 and 2 explored if the patients’ paying status would influence the GDPs restorative management. More than 70% of surveyed dentists reported that this factor would not influence their treatment plan. However, as seen in the results of both vignettes, a minority of GDPs reported that the factor of NHS exemption status may alter their decision, which was further highlighted in the free text responses. Reasons, such as lack of financial risk to the patient if treatment fails or provision of indirect restoration to offset the clinical time of RCT by qualifying for a higher UDA rate, were reported by the surveyed GDPs. Comparing the NHS Band 2 charge to the US Delta Dental insurance system, the cost of RCT in England and Wales is between one-seventh and one-twentieth the cost of RCT in the USA.25-27 In addition to a patient’s NHS paying status, multiple other confounding factors also need to be considered, which could affect a GDP’s decision-making process. The authors speculate that these could include a patient’s higher caries risk and higher prevalence of caries, therefore other treatment modalities could be more suitable for those exempt NHS patients.
Limitations
One of the clear limitations of this study is the lack of clinical and radiographic information supplied in the vignettes, therefore the results should be viewed with caution.
The intention of this study was not a direct simulation of clinical practice cases; the vignettes were designed to help identify and understand the trends within general dental practice and GDPs’ attitudes to the restoration of posterior root filled teeth.
The majority of responses collected for the survey were obtained through a social media link. This was highly effective in collecting data, however it isolates dentists who have limited access to computers and are less familiar with social media based professional groups. Subsequently the most experienced dentists, with over 20 years post qualification, made up less than a quarter of participants. A postal survey option could have been used to reach those practitioners, to ensure accurate representation of the survey sample.
Finally, the limitations of self-assessment and use of questionnaires need to be considered when interpreting the results of this study. Particularly, social desirability bias which favours overreporting of “good” behaviour and omitting “bad” behaviour may be prevalent in a vignette survey setting.
Conclusion
The responses to the vignettes presented in this survey show that decision-making for the restoration of the root filled posterior tooth is a complex process. It can be influenced by many factors, summarised below.
Tooth factors
Remaining tooth structure was the main factor for the GDP with respect to restoring root filled posterior teeth. Missing marginal ridges and parafunctional habits increased the likelihood of provision of an indirect restoration.
Patient factors
High caries risk and persistent symptoms were important factors to most of the GDPs surveyed and were shown to defer the provision of the definitive restoration.
Financial factors
From this study, there is evidence to suggest that finances can drive treatment decisions. Although for the majority of GDPs, finances wouldn’t change their management, a patient’s fee-paying status may change a dentist’s approach to care due to complexity of patient needs.