
Abstract
Aim:
The dental handpiece noise in a dental surgery is concerning to both patients and staff as a major cause of dental phobia in patients and potential hearing loss in clinical staff. High-frequency noise generated by dental handpieces is considered to be the worst of the many noises in a dental clinic. Methods to reduce this noise have been proposed and either passive or active noise reduction headphones are often suggested. However, in a dental surgery environment, the need for good verbal communication with the patient needs to be maintained. As a result, this paper aims to evaluate one proprietary anti-noise device considered suitable for this specific purpose.
Methods:
Lab-based experiments were set up and carried out to evaluate QuietOn, using GRAS 43AG-1 Ear and Cheek Simulator to mimic a section of the human head and ear to represent the acoustic characteristics of an actual ear. Two types of dental drill noise recordings, one for electric motor-driven and another one for air turbine-driven, were played back through high-definition speakers. Sound data captured by the simulator are then visualised and plotted using MATLAB for analysis.
Main findings:
QuietOn is effective at low frequencies (< 1kHz). However, when dealing with high-frequency noise such as dental handpieces it is ineffective yet subdues verbal communication.
Conclusions:
Further development of passive or active noise cancellation earplugs is still needed to target dental handpiece noise while maintaining verbal communication.
Learning Objectives
To learn about progress being made to reduce unwanted dental surgery noise for patients and staff
To understand why commercially-available devices offer little help
Introduction
Dental drills, also known as dental handpieces, produce a characteristic high frequency, narrow-band noise that is uncomfortable for patients and is also known to be harmful to dentists under prolonged exposure.1 -7 The dental handpiece noise is generated by components rotating at high speed. Electric and air turbine-driven are two main types of dental handpieces commonly used in dental surgery. Electric handpieces have speeds of around 200,000 revolutions per minute (rpm), meaning the peak noise generated by mechanical resonance will be around 3.3kHz. Air turbine-driven handpieces normally operate at a speed range of 250,000–450,000rpm, corresponding to 4.2–7.5kHz. Therefore the target frequency range for dental handpiece attenuation should be between 3.3 and 7.5kHz.
There are other unpleasant noises in dental surgery which can also be harmful, including the suction apparatus and the ultrasonic cleaning tool.8,9 However, dental handpiece noise is frequently cited by patients as an unpleasant and anxiety-inducing sound and can result in patients avoiding treatment for oral disease leading to further pathology and increased disease and cost of treatment. Dental handpiece noise has scored highest on the Modified Dental Anxiety Scale (MDAS). 10 A study conducted in Hong Kong 11 has shown that more than 76% of the participants, even those who come from a dental practice background, would prefer a lower volume of dental handpiece noise.
From previous work in this field, three main noise control methods available, namely passive noise control (PNC), adaptive filtering (AF) and active noise control (ANC), 12 were considered here.
PNC is a simple approach to noise attenuation that works by blocking the acoustic pathway from a noise source to the ear canal. This is typically effective above about 1kHz, attenuating by up to 20dB but as it does not selectively reduce noise peaks, they can still be perceived. 13
Adaptive filtering (AF) of dental handpiece noise focuses on removing the unwanted noise from the electrical signal driving earphones and has been proven to be effective in a 30dB reduction of specific signal peak frequencies up to around 10kHz. 13 However, as electrical handpieces have an internal gearbox that generates two noise peaks of a fixed ratio, these can both be tackled by the AF. 14 In addition, AF allows reproduction of human speech from the filtered electronic signal, which can be unnatural to hear.
ANC or “anti-noise”, uses similar technologies as AF, but focuses on reversing the unwanted noise played back in the ear out of phase at the same frequency and amplitude to cancel the original acoustic noise. ANC technologies are generally limited to frequencies below 1kHz such as talking, street sounds, traffic and engine noise, 15 and will be largely ineffective against dental surgery noise. Producing anti-noise in the acoustic domain is also technically challenging for frequencies above 1kHz as the “zone of quiet” is inversely proportional to the peak frequency to be reduced. 16 A recent study by Kim et al. 17 concluded that QuietOn Dental (QuietOn Ltd., Kempele, Finland) had the best characteristics of the four commercially-available devices tested but was still unsuitable overall and further development was needed.
In a dental surgery environment, verbal communication between dental staff and patients is vital to enable successful treatment, especially for phobic patients.16,18-19 It is therefore desirable to protect the patient and dentist from this noise while allowing two-way verbal communication, which is essential to best practice patient care. Commercially-available ANC products will attenuate low-frequency speech while PNC will block all sounds at high frequencies. Neither of these two technologies can suppress dental handpiece noise while maintaining speech sound.
This present study was designed to test the QuietOn Dental device in a previously-established test environment 16 to evaluate its effectiveness in dental handpiece noise suppression while allowing two-way communication.
Methods
QuietOn Dental has a compact design similar to Apple™ Airpods (Apple Inc., Cupertino, CA, USA). However, it has neither an on/off button nor the capability to connect to mobile devices to play other types of sounds, such as music. The device tested comes with three sets of Comply™ (Comply Foam UK, Winsford) foam tips of the same size. A photograph of QuietOn Dental (hereafter referred to as QuietOn) earplugs and the Comply™ foam tips is shown in Figure 1a.
According to the operational manual, QuietOn is ready to use the moment the user takes them out of the charging box. The user can simply place them into their ears and get on with the other activities. Since the shape of the earplug is quite unique, fitting instructions were referred to. Figure 1b shows QuietOn earplugs being worn by an adult male. One subjective perception from the authors is that the earplug is easy to put on by referring to the instructions but difficult to find the desired position, i.e. the position that offers the best noise-cancelling performance. In other words, the earplug only works when it is pushed against the ear canal and seals it, similar to a conventional pair of PNC earplugs. This suggests that different fits can affect its performance on noise suppression. Therefore, two types of fit (tight and normal) were investigated in the experiments.
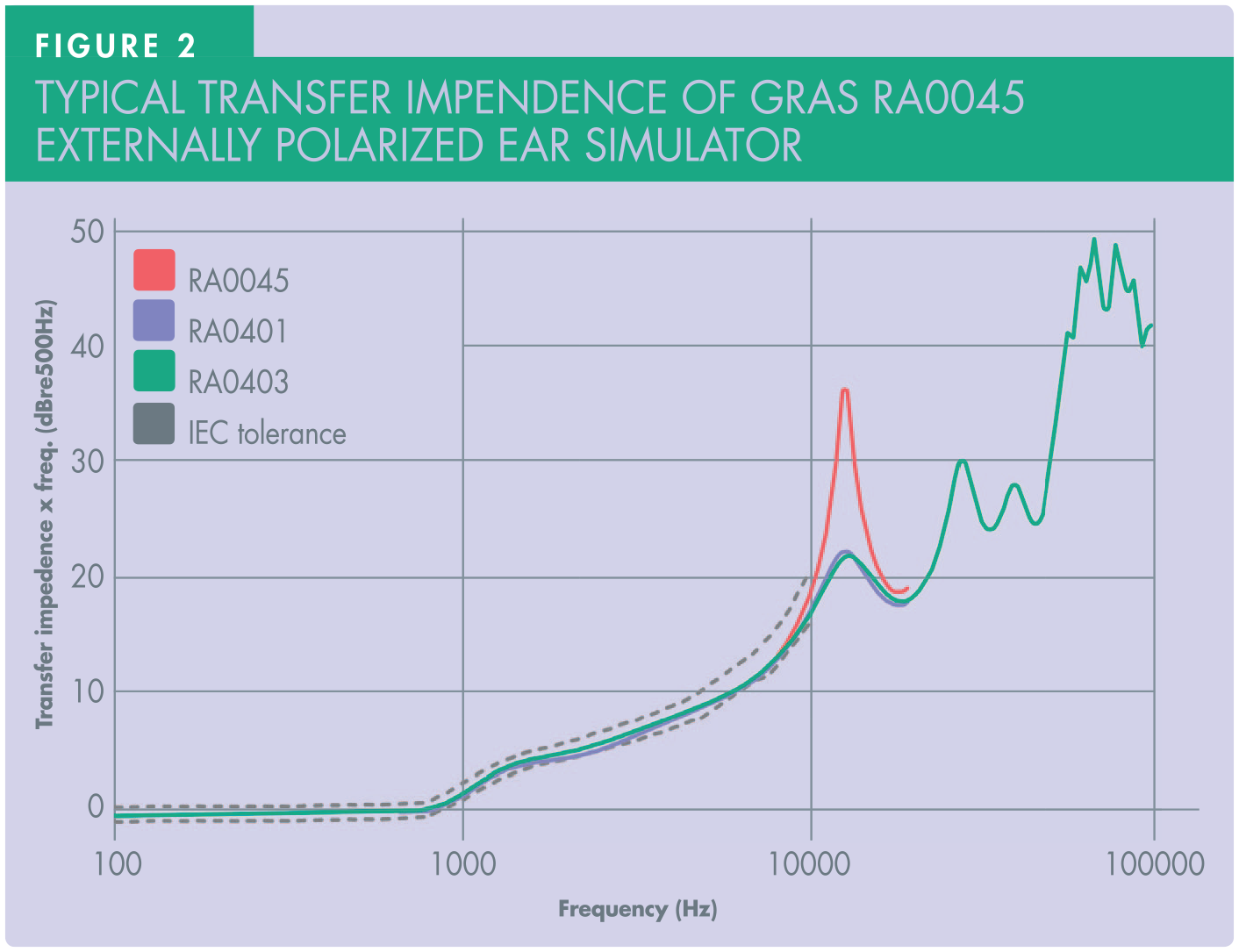
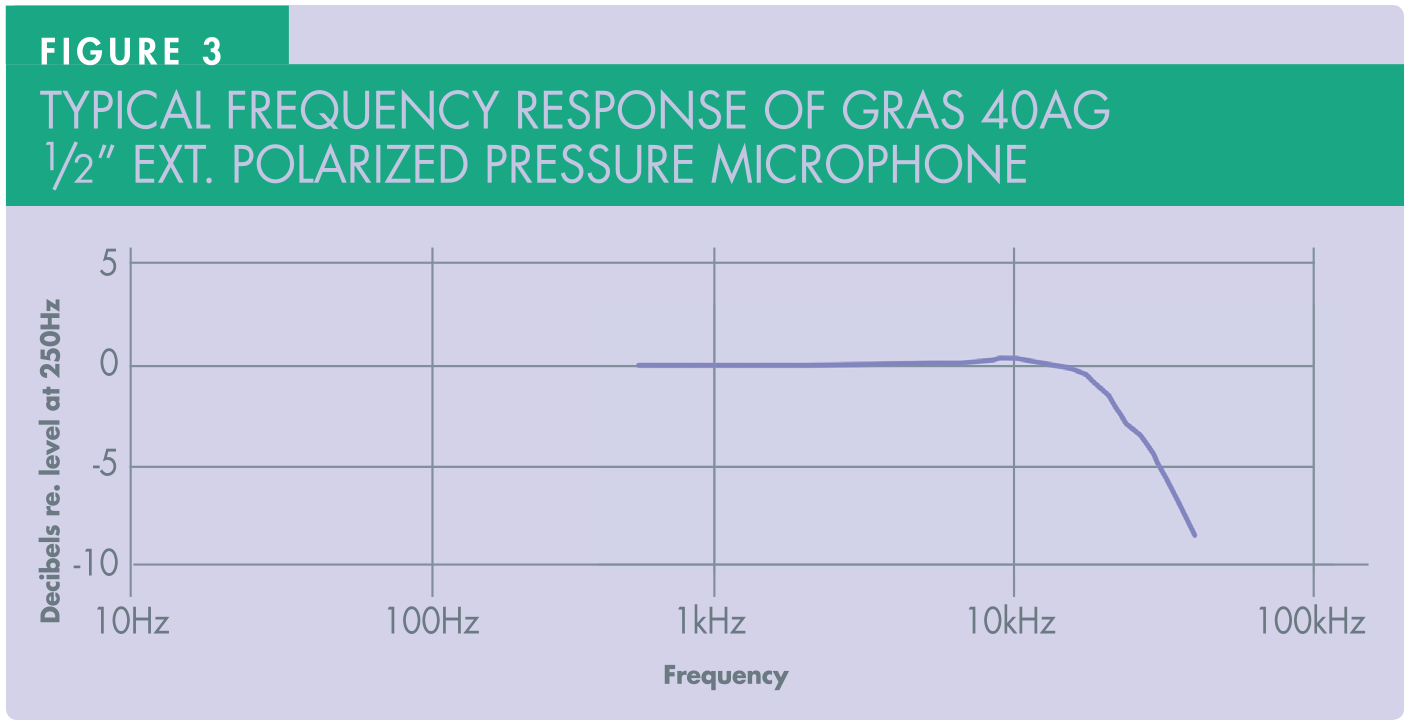
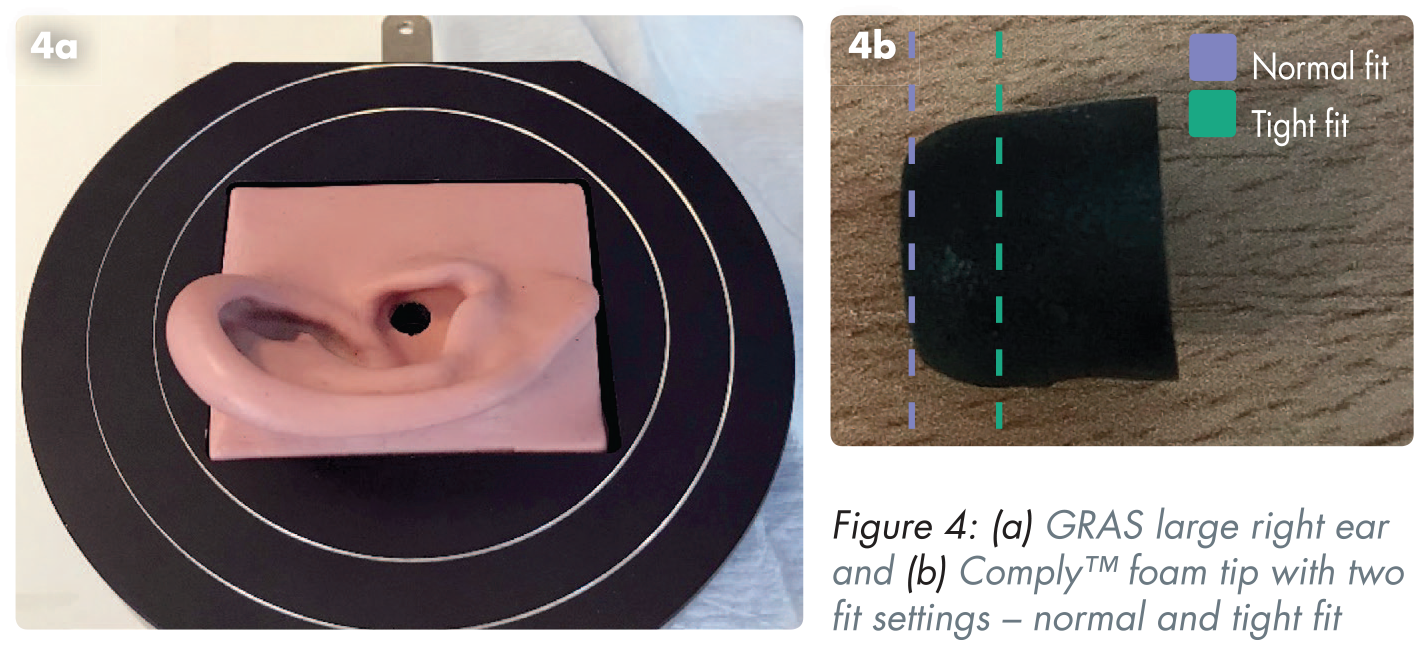
A calibrated GRAS 43AG-1 Ear and Cheek Simulator (ECS) (GRAS Sound and Vibration [Axiometrix Solutions], Skovlytoften, Denmark) 20 was used to mimic a section of a human head and ear canal, representing the acoustic characteristics of an actual ear. It contains GRAS RA0045, 21 an externally polarised ear simulator according to IEC 60318-4, 22 which works effectively below 10kHz. Typical transfer impedance for the RA0045 can be found in Figure 2, which shows that within the frequency range of interest (3–8kHz), the ear simulator is acceptable for this application. The ECS uses a GRAS 40AG ½” externally polarised pressure microphone 23 according to IEC 61094-4. 24 The typical frequency response (Figure 3) shows that the microphone is suitable for up to 20kHz. Figure 4a shows the GRAS 43AG-1 ear and cheek simulator with a GRAS KB0065 Large Right KEMAR Pinna. 25 A normal fit is achieved by gently pushing the foam tip against the artificial ear without deflecting its shape too much. In order words, a normal fit can be understood as a comfortable fit that users are most likely to achieve when actually wearing the earplugs. A tight fit is achieved by forcing the foam tip halfway into the artificial ear, deforming it considerably to create a much better air-tight seal. This aims to create an ideal environment for testing. An indication of the amount of foam pushed into the artificial ear is presented in Figure 4b.
The experiment setup is shown in Figure 5. The ECS is powered by GRAS 12AD which is also the hardware interface between the ECS and a personal computer (PC). A high-performance Behringer (Behringer/Music Tribe, Willich, Germany) MS16 16-Watt monitor speaker was used at a constant volume setting to playback sound recordings representing the sound source. Each type of dental handpiece sound recording was played simultaneously with a speech recording. All digitised audio recordings were 24-bit audio, with a sampling rate of 48kHz and a duration of ten seconds. The speaker has a frequency response over the 80–20kHz range 26 that is suitable for this study. To mimic a dental surgery environment, the nominal distance from the ear to the dental drill and the dentist is estimated as 150mm horizontally and 50mm vertically.
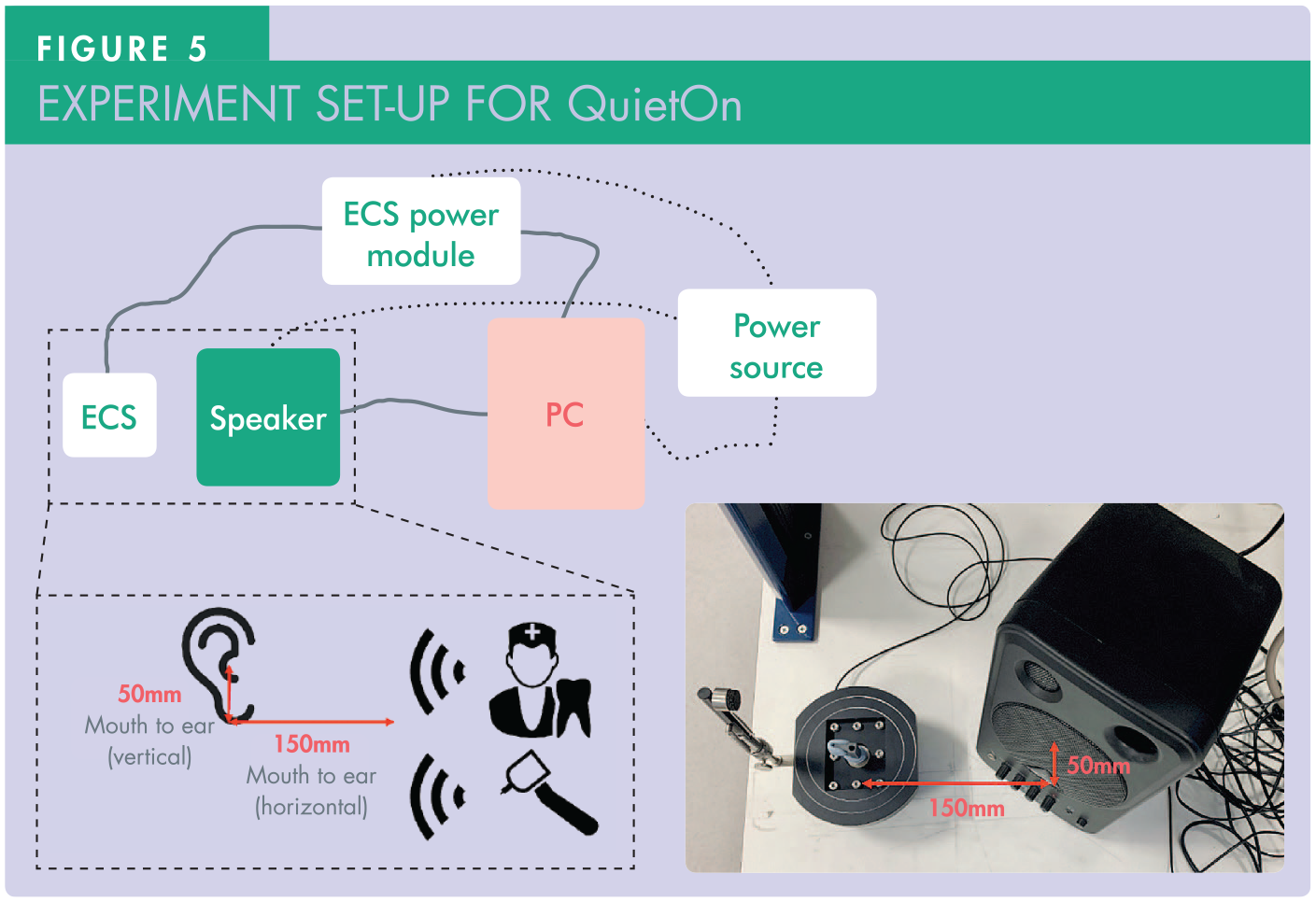
A Windows® PC (Microsoft Corporation, Redmond, WA, USA) was used to capture the sound data transmitted through the ECS. MATLAB® (The Mathworks Inc., Natick, MA, USA) applications were developed to enable data recording and analysis. Frequency domain techniques are widely applied to perform audio signal analysis as they are able to analyse individual frequency components of a signal, 27 amongst which Welch method 28 is used in this study due to its popularity. Welch’s power spectrum density (PSD) analysis is enabled by the MATLAB Signal Processing ToolBox. A window size of 2048 and 1024 overlapped samples were used to produce a PSD plot. The frequency spectrum for the PSD plot was selected to be 16kHz as above this, the threshold of human hearing starts to increase rapidly. 29
Results
PSD analysis for the two types of handpiece noise and two types of fits using QuietOn are presented in Figures 6 and 7. In these plots, three sound profiles are plotted: the original handpiece noise with speech without wearing QuietOn (black); wearing QuietOn with tight fit (blue); and wearing QuietOn with normal fit (green). The power of the signal at specific frequencies (indicated by the vertical axis) is a relative measure, as commonly used in the Welch method, where a higher value indicates a more powerful noise.
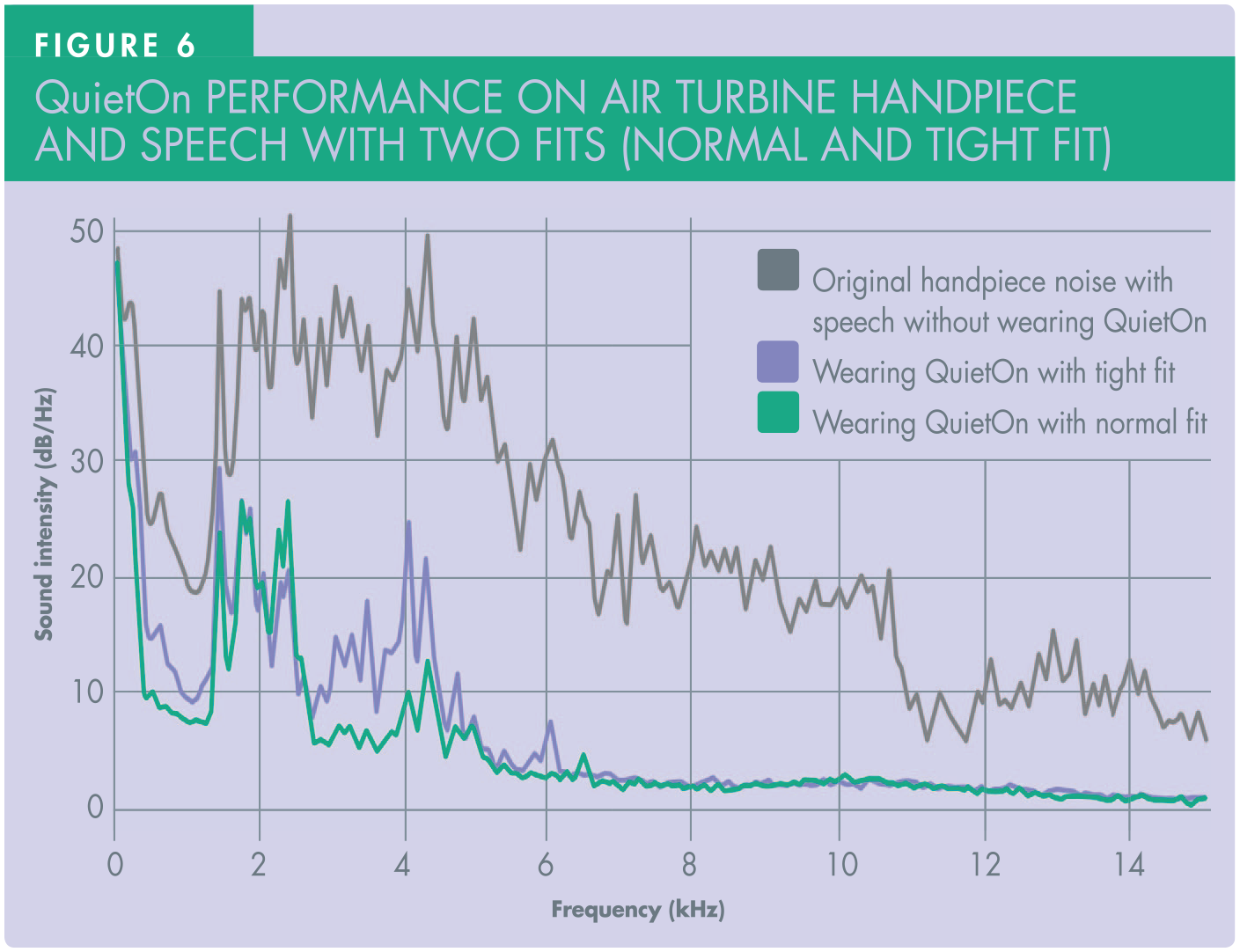
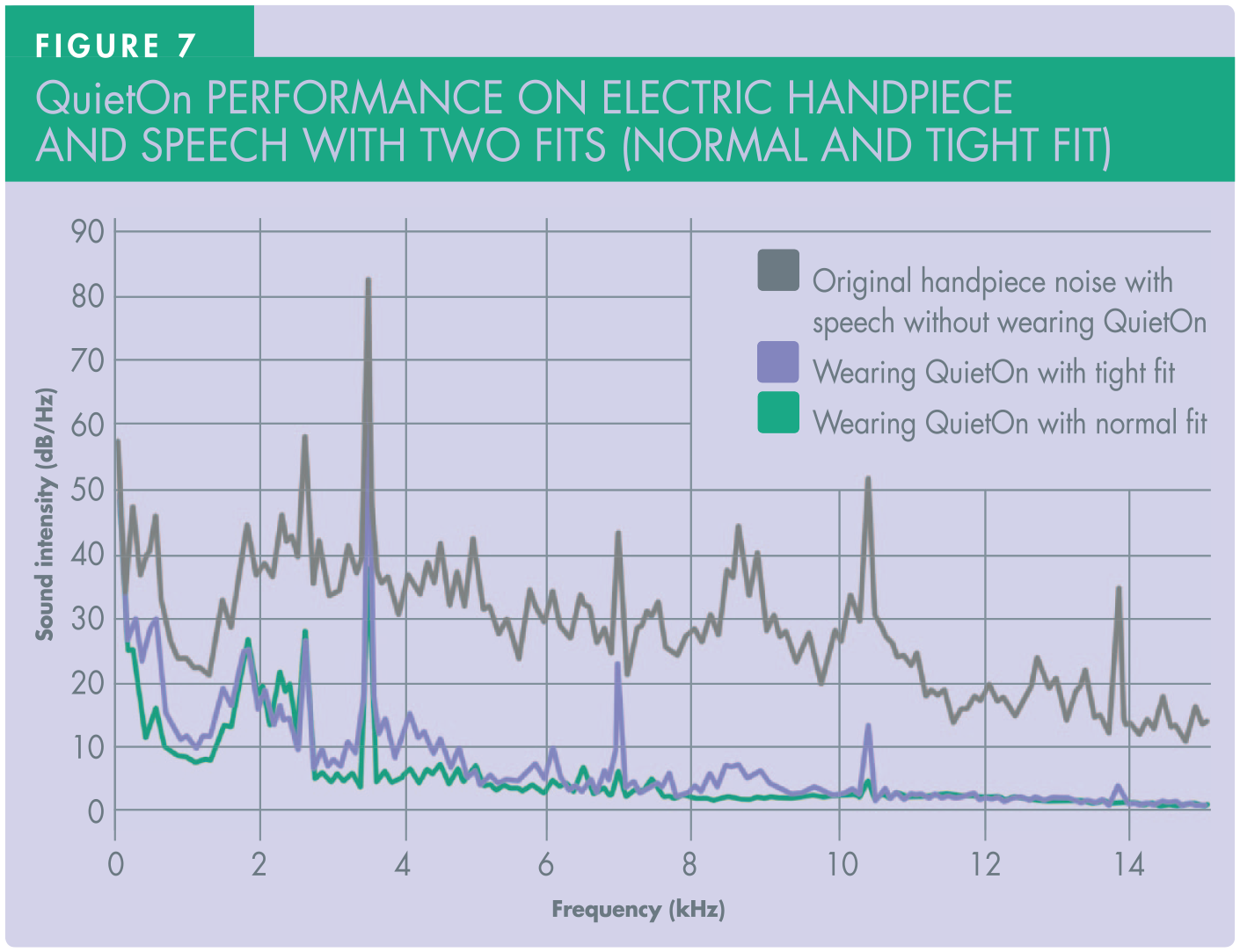
From the figures it is obvious that frequency characteristics of electric and air turbine-driven handpieces are distinct. An air turbine-driven handpiece has several noise peaks due to speed changes when making contact with teeth. Main peaks occur between approximately 2–5kHz. An electric handpiece, on the other hand, is more consistent due its geared mechanical tramission. It has a main noise peak at 3.3kHz, corresponding to its constant speed of 200,000rpm.
When comparing both fits with the original noise (black line in Figures 6 and 7), a significant reduction in noise power can be observed when QuietOn is worn. This is indicated by a large drop of response profiles. This suggests that when QuietOn is used together with Comply™ foam tips, handpiece noise can be suppressed to a significant amount. From both figures it can be observed that different fits indeed have an effect on the noise attenunation performance, with tight fit being more effective. This is reflected on a lower response profile (blue line in Figures 6 and 7) compared to normal fit (green line in Figures 6 and 7), especially when noise frequency is lower than 1kHz and higher than 3kHz. Interestingly the performance of both fits is almost identical at around 2kHz.
With normal fit using QuietOn, noise attenuation performance starts to weaken beyond 3kHz. It is worth noting that the only changing configuration during the experiments is the type of fit. When the foam tip was not fully sealed, peaky noise with higher frequencies managed to pass through, indicated by the remaining noise peaks (green line) shown in both Figures 6 and 7.
The results show that within the frequency range of zero to approximately 1.5kHz, QuietOn is able to suppress the noise by at least 10dB, even with normal fit. In frequency range 3–6kHz, QuietOn was able bring the noise level down, most likely by using the foam tip, but “peakyness” of the handpiece noise remained. Beyond 6kHz the earplug acts as a good passive insulation and essentially prevents all sound passing through to the ear.
Discussion
The present study set out to test the QuietOn device with the experimental set-up used in previous studies. 16 These initial tests have indicated that QuietOn is just like other common noise cancellation earphone/headphones that are only capable of suppressing low frequency noises. This is in agreement with the recent work by Kim et al. (2022). 17 According to the QuietOn website , the device claims to focus on suppressing the noise below 1kHz and will just function as a passive insulation for higher frequencies. 30
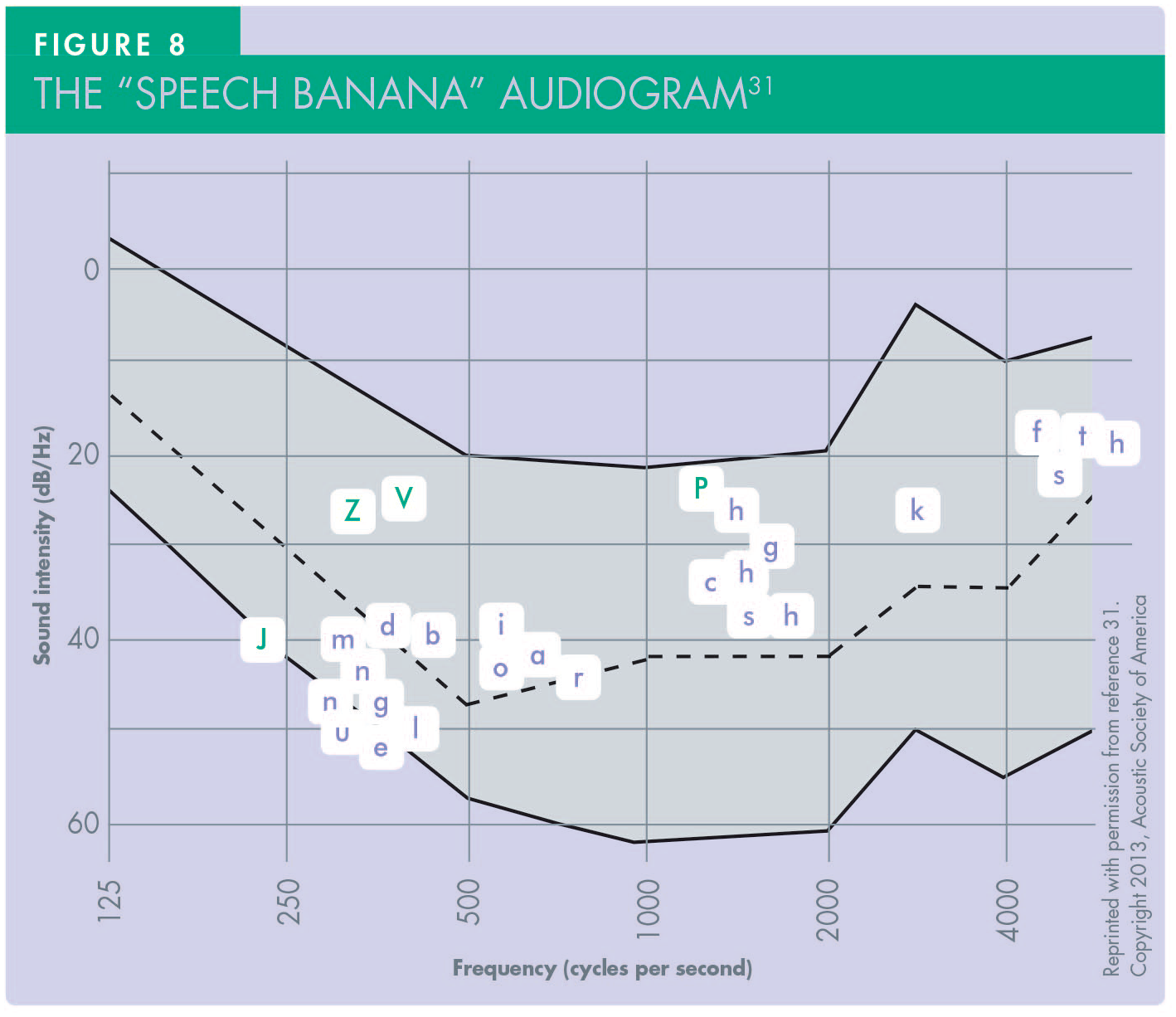
With a demand for maintaining verbal communication in dental surgery, it is necessary to understand speech characteristics. Commonly-used English speech phonemes feature in a banana-shaped cluster on a frequency audiogram, which is often referred to as the “speech banana” (Figure 8). 31 The majority of phonemes are within the frequency range of 250Hz to 2kHz, except for “f”, “s” and “th” which are around 5kHz. In order to maintain the delivery of these phonemes, sounds with 250Hz to 2kHz must not be attenuated too much to allow effective verbal communication. However, from the experiment results and what is claimed on the QuietOn website, speech frequencies with this range were significantly suppressed. Based on this, the authors are in agreement with Kim et al. 17 that while QuietOn can reduce some dental surgery background noise it would not meet the requirements of suppressing drill noise while also enabling verbal communication from dentist and dental nurse to the patient.
The results shown in this study plus four commercially-available ANC devices tested in a recent study by Kim et al., 17 found that the QuietOn device had the better characteristics overall. However, there is still a clear need for a device that is able to target dental handpiece noise and reduce the anxiety-inducing effect of dental drill noise for patients, while maintaining verbal communication. In addition to dental handpiece noise reduction, there may also be a need to reduce this background noise for staff working in a dental surgery environment.
Conclusion
In the dental surgery, dental handpiece noise is a serious issue affecting successful treatment as well as wellbeing. It is therefore reasonable that individuals consider using commercially-available noise-reducing devices in an attempt to suppress unwanted dental handpiece noise. In this study, a series of tests were carried out on a commercially-available anti-noise earplug (QuietOn) that has been proven to be the best among four devices in a recent study. The results show that QuietOn can provide noise suppression in general but has very limited benefit for dental surgery noise, specifically because it cannot maintain the verbal communication frequencies that are essential in dental practice. Further development is needed to provide a reduction in undesirable noise in the dental surgery, to improve patient welfare. It may also have benefits in reducing loss of hearing for the dental team.