
Abstract
The COVID-19 pandemic has created novel barriers in providing and accessing all forms of healthcare, including dentistry. The national dental response during the first peak of the pandemic resulted in rapid changes in the provision of service, to safeguard providers and users of dental care.
Such rapidly leveraged changes resulted in several issues in service delivery, requiring careful input from managers and commissioners within NHS England and Improvement, trainees and consultants in dental public health within Public Health England, and frontline dental teams working across the health and social care system. The local response from Lancashire and South Cumbria is outlined within this article.
Teamwork, communication and reflexive, iterative learning from these groups ensured the delivery of an Urgent Dental Care service during the first lockdown of the pandemic.
The impact of COVID-19 has enabled considerable learning which will inform future pandemic planning, alongside providing the opportunity to deliver meaningful change within NHS dentistry as the service continues to recover.
Learning Objectives
To understand the role of NHS England and Improvement Dental Commissioning teams, Public Health England Dental Public Health teams and front-line dental providers in the Lancashire and South Cumbria pandemic response
To review the barriers and enablers experienced during the first peak of the COVID-19 pandemic and national lockdown
Introduction
The emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and the associated COVID-19 pandemic, have created novel barriers to the delivery of NHS dental care. This has impacted on those seeking to access services, alongside providers in both primary (general dental practices) and secondary (hospitals) care settings. 1
In response to increasing infection and mortality rates due to COVID-19 infection, on 23 March 2020, the UK prime minister instigated nationwide ‘lockdown’ within England. This incorporated measures to curb transmission, such as making ‘non-essential’ travel illegal for all, and the closure of many retail outlets. 2 The most vulnerable in society were advised to ‘shield’ in an even more stringent manner to protect their own health. Two days later, the chief dental officer (CDO) for England, who is the most senior advisor to government for dentistry and leader of the country’s dental profession, wrote to all providers of dental services (both NHS and independent) in England requesting the cessation of all ‘routine’ dental services across primary and secondary care settings. The delivery of ‘urgent care services’ was advocated for, which included appropriate advice, analgesia and antimicrobials following telephone triage (which could include a telemedicine approach). 3 Additionally, it was advised that local ‘Urgent Dental Care’ (UDC) systems should be created to safely treat those whose dental issues could not be managed remotely. A UDC was a single site where such management was offered.
Many procedures in dentistry generate an aerosol and take place in close proximity to the upper respiratory tract; an area likely to harbour SARS-CoV-2, making gold-standard infection prevention and control (IPC) an absolute priority. 4 It was understood that patient capacity within UDCs would be reduced compared to the level that would usually be expected due to the need for enhanced IPC guidance. A standard operating procedure (SOP) for UDCs, which outlined how dental teams should deliver patient care, was released on 15 April 2020 by the CDO, stipulating required changes to IPC. 5
The CDO released a Transition to recovery SOP on 28 May 2020, which stated that all ‘routine dental services’ should resume on 8 June 2020. The document advised that service provision was recommenced based on urgency of need, particularly of those in marginalised groups, and the available clinical capacity of each dental practice. 6 A timeline of national and local activity to this point is demonstrated in Figure 1, which shows key dates alongside significant actions taken nationally and locally.
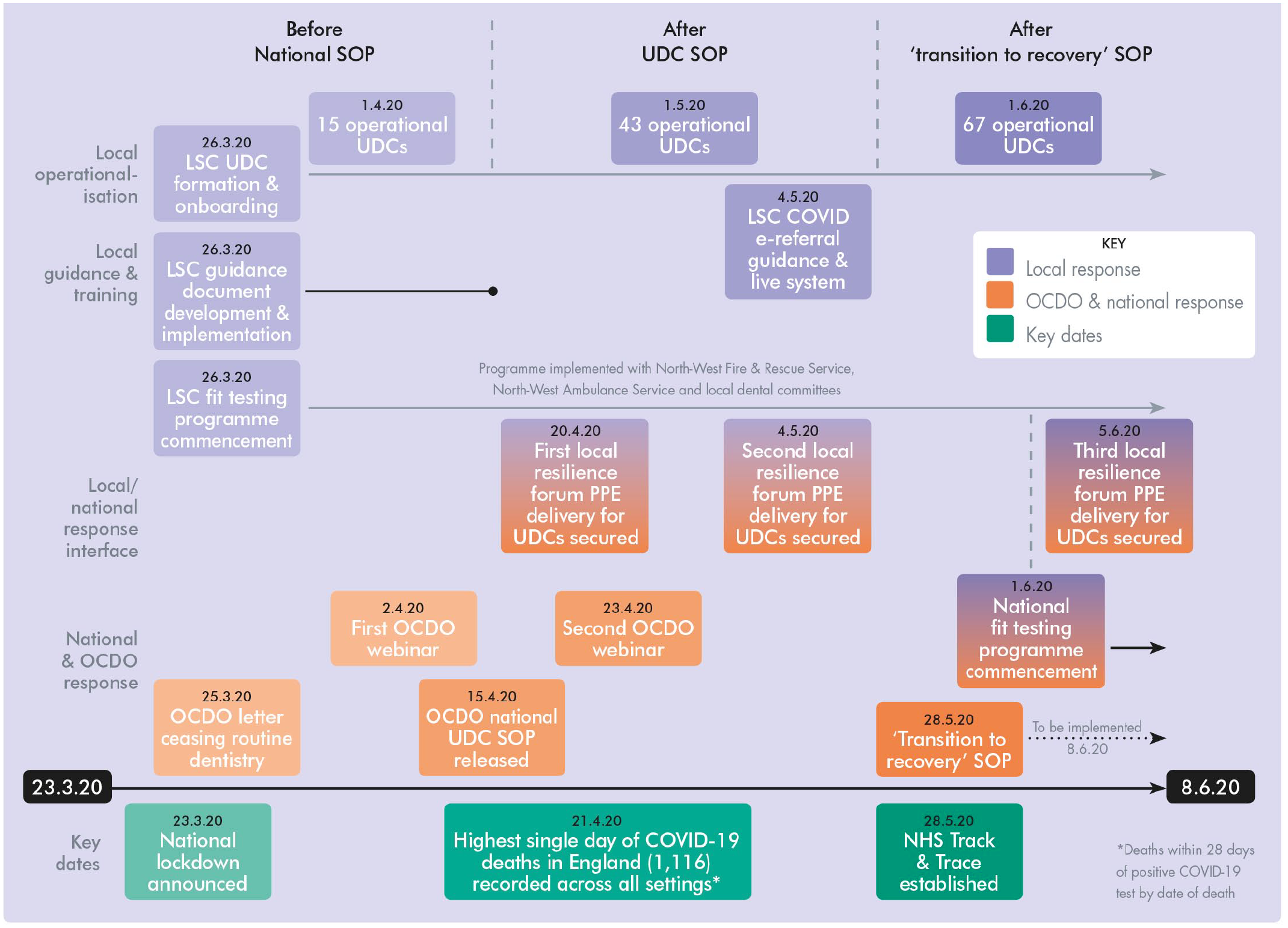
Timeline of National and Local Activity Between 23 March and 8 June 2020.
This paper aims to outline how UDCs were operationalised in Lancashire and South Cumbria (LSC) during the period when routine dental care was ceased, and the subsequent approach to ‘recovery’ taken within the locality, alongside a description of pertinent lessons learned from the experience. The undertaking outlined is demonstrated from a dental public health perspective, and based entirely on activity within LSC, which may be appreciably different to the efforts of equivalent colleagues from different regions.
Dental public health and collaboration during the COVID-19 pandemic
Dental public health is principally concerned with preventing oral disease, promoting oral health and improving quality of life via organised, societal efforts. This is underpinned by the three ‘pillars’ of public health: 7
From the perspective of pandemic preparedness, dental public health teams are well informed, with annual training on Public Health England’s (PHE’s) Pandemic Influenza Response Plan. 8 This requires a thorough understanding of how roles across all three pillars interact and offers some insight into how healthcare services may need to be adapted in the instance of a pandemic. However, the rhetoric of preparedness and reality of a true pandemic have been notably different.
Considering this prior learning, it was quickly identified that delivery of successful UDCs required careful consideration of all three public health pillars. Consideration of good healthcare public health practice was paramount in ensuring that all patients with an urgent dental care need were able to access the service. Changes to IPC reduced the possibility of transmission in dental practices, with such modifications incorporating a health protection focus. Health improvement functions were protected by encouraging the delivery of appropriate messaging during phone consultations between patients and providers, and through input into relevant communication posted on social media.
Creating a UDC system which was accessible safely and equitably, while delivering value for commissioners, required a collaborative approach to pandemic management, engaging a variety of stakeholders. Dental public health colleagues were therefore a part of a convened ‘Planning Group’, which included the following:
NHS England and Improvement (NHSEI):
a. dental commissioners and managers; accountable for decisions relating to patient access to service
b. clinicians from the Local Dental Network (LDN); advocate for dental practitioners working across primary and secondary care
Public Health England (PHE):
a. consultants and specialty trainees in dental public health; provide leadership and expertise relating to public health
This Planning Group ensured the synthesis of a holistic and coherent system-wide vision during the pandemic, and three key lines of enquiry central to the formation of a successful UDC system were rapidly identified. Firstly, could our UDCs meet the oral health needs of the population, as might be expected during a pandemic? Secondly, what changes to routine practice might be needed to safeguard the health of providers and service users? Finally, could we provide appropriate stewardship of the public purse?
These three questions were considered by the group at all stages of UDC formation. Dental public health colleagues led and supported the planning and execution of service delivery, collaborated with wider stakeholders, including clinicians, and delivered iterative evaluation of dental care provision (both patient- and clinician-facing) within UDCs.
The formation of UDCs
Pre-empting possible changes to healthcare access, our Planning Group was formed following the announcement of the first national lockdown. Support from the LDN and Local Dental Committee (LDC) was sought on 24 March 2020. Wider NHSEI and PHE teams rapidly assimilated any available guidance from other medical and surgical specialties, pooling knowledge. When dental services were ceased on 25 March 2020, it was imperative that operational UDCs were able to meet the local demand for urgent oral healthcare, minimising unnecessary referrals into secondary care centres which were straining under the burden of COVID-19. 9 In an attempt to do this, the Planning Group facilitated the delivery of a guidance document, alongside wider stakeholders, to inform best practice when managing urgent dental care during the COVID-19 pandemic. This guidance resulted in wholesale changes to routine practice.
It is important to note that two dental practices were able to immediately comply with the guidance and remained open, providing emergency dental care to the population of Lancashire and South Cumbria for the duration of the lockdown.
While UDCs were being enrolled, pragmatic modelling was simultaneously undertaken to ascertain urgent ‘need’ of the population. This took account for geographical spread, clinical complexities and vulnerabilities of the population (based on historical data from the unscheduled care dental service), while ensuring sufficient access for all, regardless of COVID-status. Considering these complexities, alongside previous urgent dental care attendances in the region, it was estimated that roughly 180 patients per day would require face-to-face management. The local Dental Helpline became the central contact point for urgent and emergency dental care, with clinicians and NHS 111 signposting to this service. Call volume throughout the pandemic is demonstrated in Figure 2. This gave an aspirational target of 30 UDCs offering six emergency appointments per day. There was a need for these services to be distributed equitably across the locality, accounting for COVID-status alongside other patient and procedural factors.
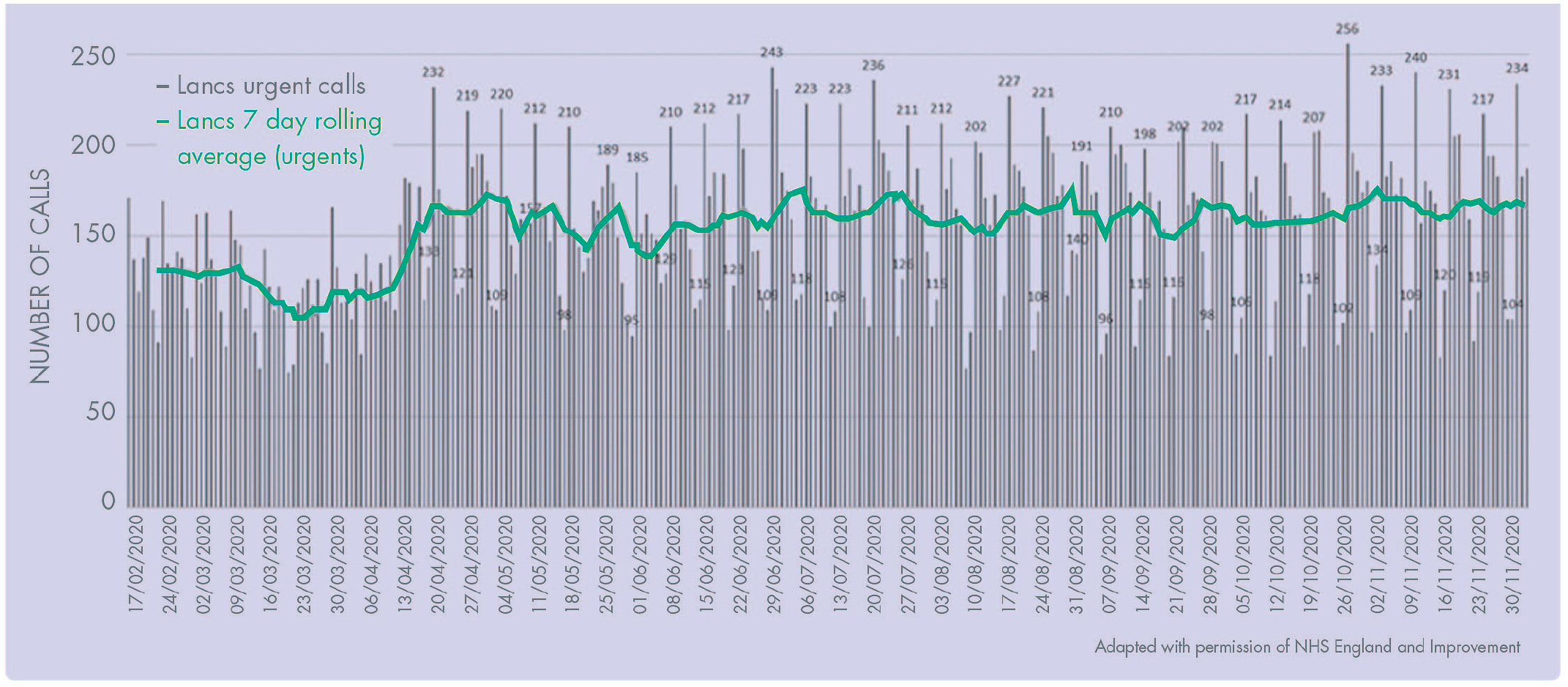
Volume of Urgent Dental Calls To LSC Dental Helpline.
Following cessation of routine care, it was paramount that any dental activity protected the health of clinicians and patients as a minimum. Consequently, from 25 March 2020, local guidance advised that operational UDCs should stop utilising equipment which generated aerosols entirely and advocated for wearing gowns and fitted respirators (FFP2 or 3, with all staff being appropriately fit tested by local acute hospital trusts). A fallow period of one hour was recommended following patient contact, facilitating thorough decontamination of surgeries after a period to allow any aerosolised droplets to settle, i.e. as a result of a potentially infectious patient coughing. Complying with this local guidance document, there were 15 operational UDCs across LSC by 1 April 2020.
A national SOP relating to UDC provision was delivered to all dental care providers by the CDO on 15 April 2020. 5 Of note within this national document was guidance around the ubiquitous nature of aerosol generating procedures (AGPs) within dentistry. Modern management modalities for both caries and periodontal disease typically result in the generation of substantial quantities of aerosol. 10 When it is further considered that the oral cavity is contiguous with the respiratory tract, and that blood and saliva are both potential transmissible mediums for SARS-CoV-2, this national SOP gave the first iteration of agreed IPC standards for dental teams to adhere to throughout the COVID-19 pandemic.11,12 The local guidance was stood down, with operational UDCs following the most contemporaneous national SOP.
By this point, LSC had developed an embryonic system of UDCs, delineated into ‘hot’ and ‘cold’ sites. Hot sites were expected to manage confirmed COVID-19 positive patients and those exhibiting COVID-19 symptoms. These sites also treated shielded groups to ensure access for the most vulnerable and minimise inequities in provision. Managing these cohorts was done safely by locally controlling patient flow through dental practices, treating shielded groups at the very start of the day, alternating surgeries for every patient (to facilitate thorough decontamination), and using enhanced levels of personal protective equipment (PPE). 13 Cold sites were expected to treat all other urgent dental need (which could not be managed remotely) in a safe manner, conforming to the enhanced levels of IPC outlined in the national SOP. As more UDCs were enrolled, it became apparent that there were differences in treatment modalities offered across the system. For example, some practices had staff with underlying health conditions. As a result, staff in these practices would undertake non-aerosol generating treatment, when clinically acceptable, but would refer patients requiring AGPs to an appropriate local UDC.
Regardless of complexities, as a minimum, the system sought to provide ‘urgent mandatory dental services’, as outlined by the General Dental Services (GDS) Contract and Schedule 4 of the NHS Charges Regulations.14,15
By 1 June 2020, 67 sites were offering at least one emergency appointment per day, resulting in capacity for over 300 daily urgent dental appointments. Half of these were equipped to treat patients requiring AGPs. This safely met the increased care demand and offered sufficient resilience across the dental healthcare system.
Learning from developing a UDC system
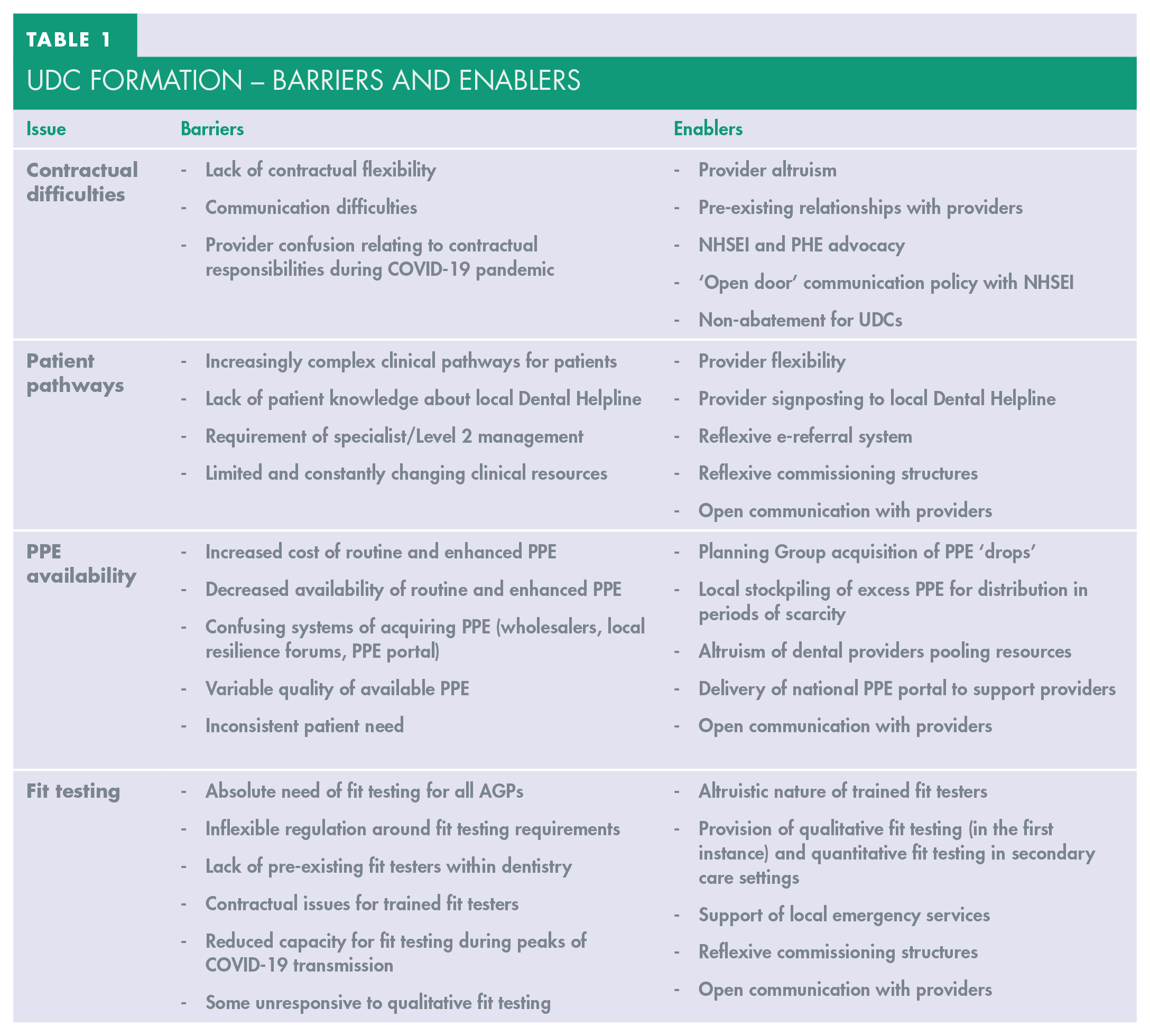
Despite the success of rapidly deploying UDCs, there were a range of issues which impacted on the availability of care. Specifically, these related to the lack of contractual levers available for commissioners to register new UDCs; changes to patient pathways; availability and cost of PPE; and the need for clinician fit testing – all compounded by a backdrop of rapidly changing evidence and guidance and a developing pandemic. Table 1 demonstrates barriers and enablers experienced during UDC formation.
Udc Formation – Barriers And Enablers
Contractual difficulties
The main difficulty experienced by commissioners in enrolling practices to become UDCs was the lack of available contractual flexibility to incentivise the process. Strong relationships with providers were paramount. Of the 221 NHS dental providers in LSC, 67 practices were operating as UDCs by the end of May 2020, indicating that over 30% of practices had opted to participate without any promise of financial remuneration. The lack of clarity around how dental contracts may be managed during the COVID-19 pandemic was distressing to many providers and meant that these practices remained open despite the fact they could be operating at a financial loss. As one provider said, this decision was driven by wanting to ‘do the right thing’ for the patients they served.
Maintaining trust between commissioners and practitioners was extremely important as lockdown measures were instigated. Also, commissioning teams were keen to protect funding traditionally earmarked for dental care provision. Continued face-to-face dental activity was a strong argument for UDCs to be paid their full contractual value, especially as overheads increased through the need to source comparatively costly PPE. 16 Consequently, the Planning Group advocated, at a national level, for UDCs to have an easement of their required contractual obligations, regularly communicating with providers via the LDC. As a result of this support, practices which had operated as UDCs eventually received guarantees that their NHS contract would be paid with no abatement for the lockdown period. 6 Commissioners were therefore able to ensure that sufficient funding was available to treat those with normative, urgent dental need, alongside maintaining the trust of the dental workforce. Upon the resumption of routine dental care on 8 June 2020, non-UDCs had an abatement of 16.75% of their contract value. 6 All practices had to maintain 20% of their usual NHS capacity from this point on to receive their full contractual payments. Open communication has been shown to elicit positive outcomes for patients across a variety of healthcare settings, and this example is no different. 17
Patient pathways
From a patient management perspective, clinical pathways also became more complex and difficult to navigate. Typically, when a patient requires treatment, they contact the practice with which they have an existing relationship. Many practices were closed during this period, and not all practices were undertaking all emergency treatments. Additionally, there was an implicit understanding of the large numbers of individuals who may have no such relationship with a dentist. Flexibilities to access and patient flow across the system were therefore required.
Signposting patients to the local Dental Helpline was the first stage of ensuring those in need could access care. This was typically undertaken following telephone/telemedicine consultation with an individual’s dental practice, or by staff working for NHS 111 for those without a relationship with an NHS dental provider. Upon calling the Dental Helpline, the individual would be triaged by a dental nurse and allocated to a UDC, if appropriate. COVID-19 and shielding status, alongside clinical need, would help inform this process.
However, it became apparent that this approach was insufficiently flexible to manage the clinical need of patients, and the fluctuating capacity within dental practices. Clinician factors, patient factors and availability of clinical resources (including staff absence due to COVID-19) could all impair the availability of certain treatments within UDCs on a daily basis. As a result, a practice may have had capacity to undertake certain treatments one day, but not the next, necessitating onward referral for appropriate management, e.g. AGP treatments. Learning through this iterative process, it also became apparent that some patients had needs outside the scope of practice commensurate with that of a general dental practitioner, as defined by the Foundation Dental Curriculum. 18 These patients required referral to clinicians with enhanced skillsets, and reducing unnecessary referrals to secondary care settings remained a priority. The ‘Level 2’ Oral Surgery Service, delivered in the primary care setting and locally commissioned by NHSEI, was therefore reopened as a matter of urgency. 19 This operated in both a ‘hot’ and ‘cold’ site capacity to meet the needs of the population. The service, incorporating several sites across the LSC geography, became part of the wider UDC system. It was fully operational by 1 May 2020.
To facilitate the flow of patients across dental practices and Level 2 providers, the locally commissioned e-referral provider (Dental Referrals [FDS Consultants]) was engaged. An e-referral form was delivered to enable onward referral to an appropriate location, e.g. a site where AGPs could be undertaken or a Level 2 Oral Surgery provider, based on clinical factors. Providers were given the option of switching off the acceptance of new referrals if they were operating at full capacity or in event of resource scarcity. The algorithm of the e-referral system ensured that patients were always allocated a clinician with an adequate skillset for the treatment proposed, in the most geographically convenient location.
This e-referral platform remained live after non-UDC dental practices reopened on 8 June 2020, to facilitate onward referral of patients to an appropriate location. Data from this can be viewed in Figure 3, noting the spike in referrals as dental practices prepared to resume routine care (following the Transition to recovery SOP on 28 May 2020). Due to the robust nature of the UDC system by this point, the service was not overwhelmed.

Number of E-Referrals Sent Per Day Across Lancashire & South Cumbria.
PPE availability
Regarding PPE, ‘appropriate’ levels have been required by all clinicians working in dental practice, which has often been influenced by the treatment being undertaken. Although there have been some changes in what has constituted ‘appropriate’ over the course of the COVID-19 pandemic, it has consistently been ‘enhanced’ compared to what is typically worn by dental teams.
Nationwide, it was found that clinicians initially struggled to acquire appropriate PPE due to scarcity and cost, creating a significant financial burden. 20 Additionally, the type of PPE offered by suppliers, and availability of requested products, was found to be extremely variable. As more NHS dental providers began offering their services as UDCs, demand for PPE increased in line with a greater provision of treatment. Although the responsibility for acquiring PPE typically rests with the provider, clinical activity and associated PPE usage were monitored across the region during the COVID-19 pandemic. This was to ensure sufficient responsiveness and emergency PPE acquisition in the event of absolute scarcity, due to the crucial need for PPE in the delivery of dental services.
Providers could request PPE from the following sources:
Dental Wholesalers: to be used in the first instance
Local Resilience Forums (local multi-agency group, which holds statutory responsibilities during emergency response): to be approached if wholesale routes were unsuccessful
‘The PPE Portal’: limited and rationed supply; for ‘emergency top-up’ only
Alongside these sources, some dental practices pooled resources, and others had previous ‘stockpiles’ of PPE they could access. Nationally and locally, dental public health teams (and our Planning Group) engaged with the National Disruption Service and Local Resilience Forums to acquire three large ‘drops’ of PPE. Distribution was arranged at a local level. In LSC, this was done equitably based on practice size and the number of emergency appointments offered. To safeguard the service in the event of widespread scarcity, a small amount of surplus was held by the local NHSEI team from these ‘drops’. This surplus was distributed when all other routes proved unsuccessful for providers, and ensured that urgent care provision was safeguarded.
Fit testing
The need for dental professionals to wear ‘fitted respirators’ as part of their enhanced PPE while undertaking AGPs was a further barrier in the supply of appropriate urgent care.
To confer protection to the wearer, an adequate respirator fit must be confirmed by ‘fit testing’. Respirator use, and the necessity for fit testing in dentistry, are outlined in the Health and Safety Executive’s (HSE) Control of Substances Hazardous to Health and Respiratory Protective Equipment at Work.21,22 Details surrounding this were clarified in the SOP for Transition to recovery. 23 The requirement for ‘fit testing’ was, and remains, inextricably linked to PPE provision; dental professionals must be fit tested on all novel brands and models of respirators they wear, meaning scarcity of supply can cause issues with service delivery. Fit testing must be conducted by a competent person, in line with HSE INDG 479. 24
Initially, dentists received fit testing via local secondary care centres, the North-West Ambulance Service and the North-West Fire and Rescue Service. However, this was not sufficiently reliable and a PHE funded national scheme was devised to train dental professionals as qualitative fit testers via a ‘Fit2Fit’ educational course. This course meets the level of competence outlined in HSE INDG 479. 24 Thirty dental professionals were trained in LSC, alongside the offer of an ‘honorary contract’ with the NHS, which conferred sufficient indemnity for fit testing provision outside of the individual’s own dental practice.
These practitioners acted altruistically, with no remuneration promised for their time and expertise. LDC members, in particular, bore the burden of this task to ensure dentistry could continue across the region. PHE strongly advocated for these dental professionals to be appropriately paid for their time, which ultimately resulted in a contract being devised nationally to pay dental fit testers, backdated for previous activity.
For a small number of providers, the fit testing offered by the PHE scheme was not appropriate. Those suffering from ‘long COVID’ symptoms, or heavy smokers, can have a reduced sense of smell, making this qualitative method ineffective25,26 (sense of smell being essential in effective fit testing). For these groups, local hospitals provided support with a ‘quantitative’ method of fit testing on respirators, which does not rely on the individual’s ability to smell. This approach has continued to prove adequate as services recover.
The roadmap to recovery
Despite the ongoing challenges from this unprecedented pandemic, there have been opportunities to improve the quality and ease of healthcare access for stakeholders by providing innovative solutions to issues which have arisen. 27 Although this article has, until this point, focussed on how dental services were managed during the first national lockdown in England, there is still a need for dental care to continue to re-emerge safely. Utilising an appropriate quality framework during recovery, such as Donabedian’s model, will ensure that dental services are providing an appropriate standard of care to patients. 28
It is still unknown what the long-term effects of COVID-19 are on normative dental need, but it is unlikely that oral health will have improved in the absence of routine dental care provision. Anecdotally, waiting lists for specialist dental services are at an all-time high, with all dental care providers still unable to operate at a capacity comparative to ‘pre-COVID’. Until activity returns to these levels, there will be increased strain on a partially paralysed healthcare system.
NHSEI and PHE therefore continue to support providers in their recovery, strategically planning for resumption of services, ensuring that population need is met, while keeping patients and practitioners safe. In LSC, the Planning Group advocated that providers deliver dental services considering a theoretical roadmap with 4 ‘stages’ of clinical care. This is conceptually underpinned by ideology outlined in the ‘Steele Review’ of NHS Services in England: 29
Regular patients (who have a previous relationship with the practice)
A small number of irregular attenders, referred via the Dental Helpline
This locally developed roadmap is further outlined visually in Figures 4 and 5. Central to recovery is the delivery of urgent and emergency care by all providers (i.e. a provider should not be undertaking ‘routine’ treatments if overburdened with ‘urgent’ demand).
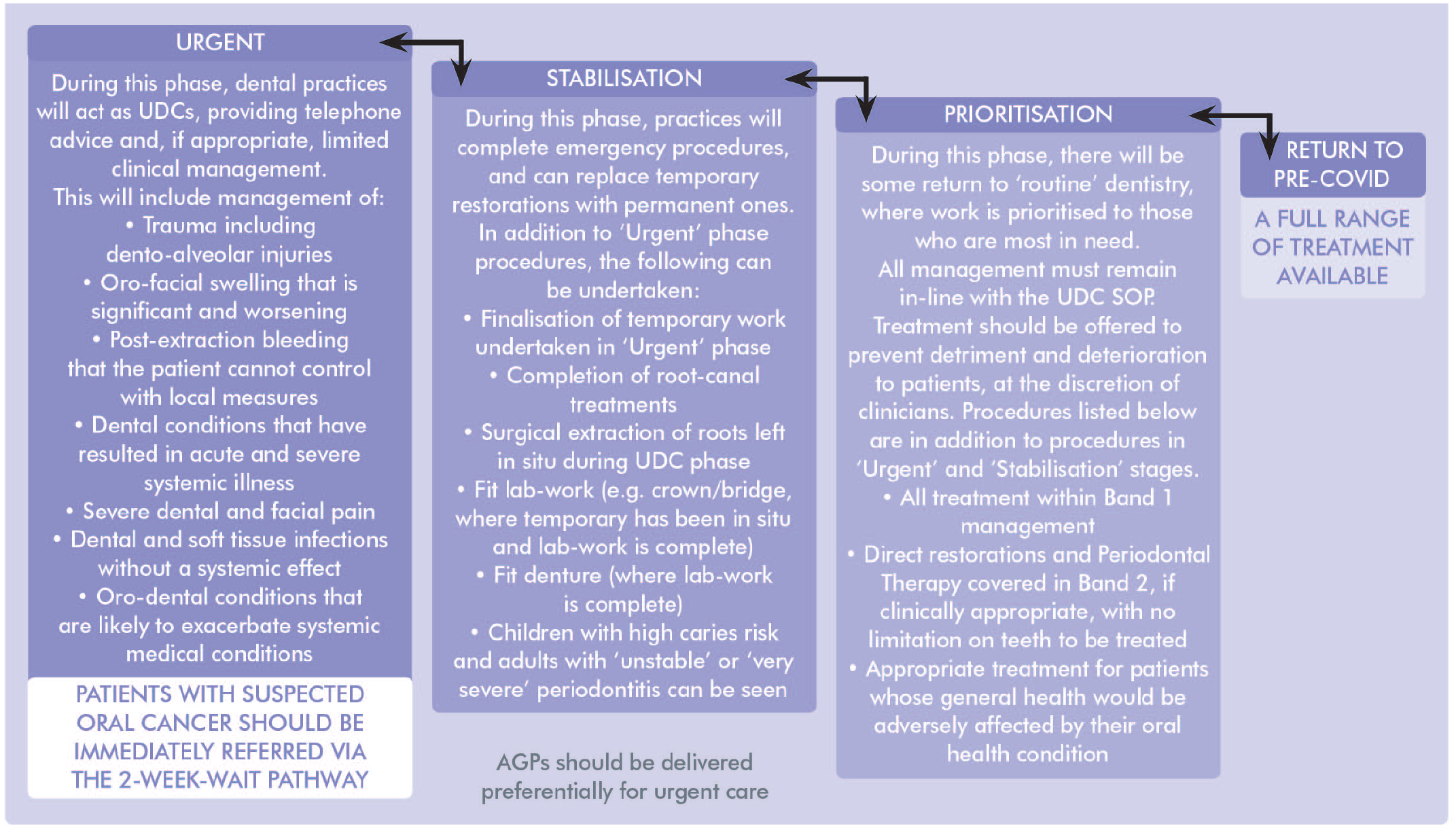
Examples of Treatment on the Roadmap to Recovery.
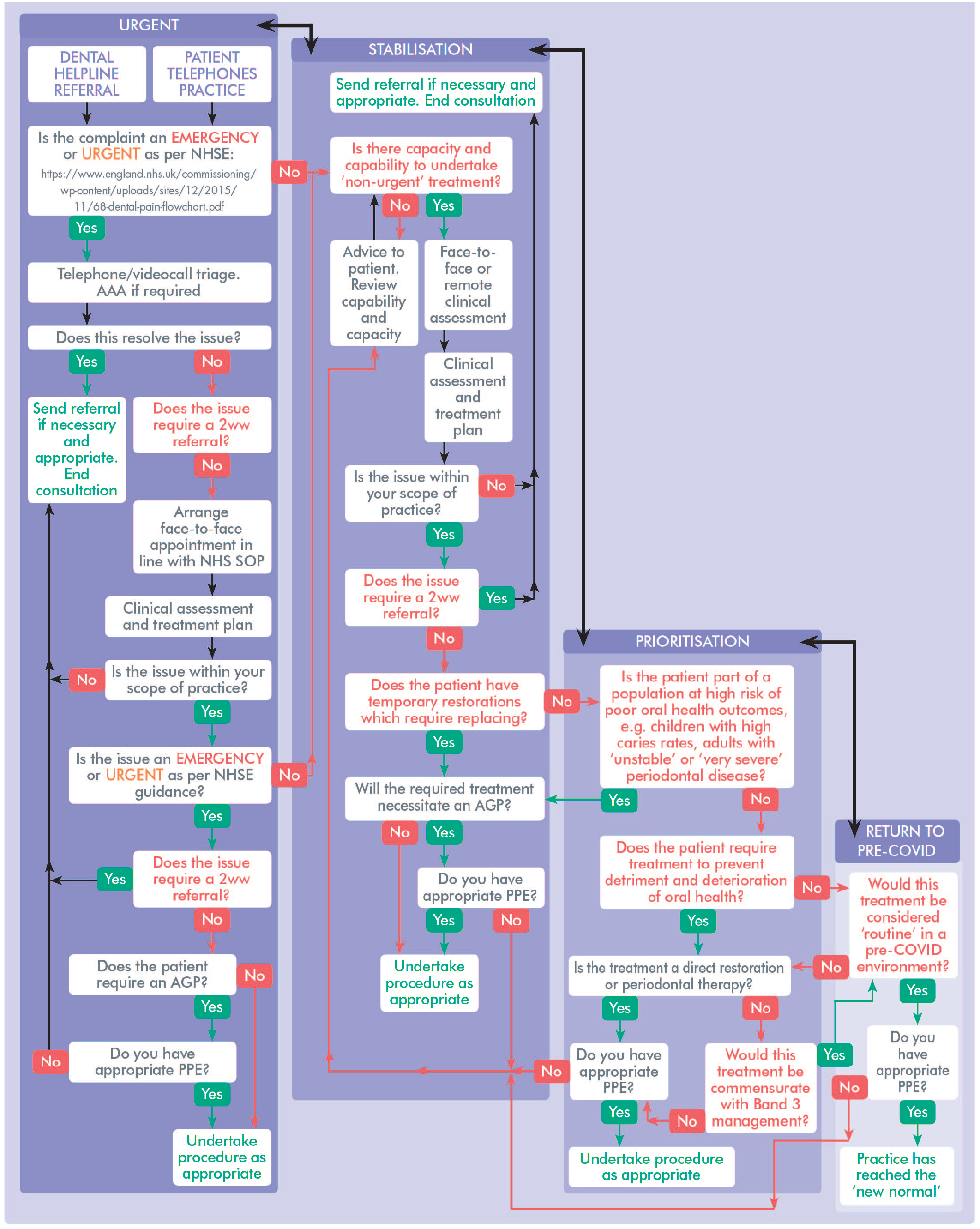
Theoretical Flow Chart of the Roadmap to Recovery.
It is hoped that providers will feel empowered to do this as, at the time of writing, it is stipulated that they must only maintain 45% of their contracted activity to receive full NHS payment.
It is important to stress that every provider will take their own journey through the roadmap outlined. There is a need to be responsive to peaks and troughs of transmission during the pandemic, which may be linked to national or regional lockdowns and could impact on service provision. Moreover, the delivery of any care is contingent on the availability of appropriate PPE; providers may therefore need to limit the type of treatment offered in the event of equipment scarcity or limited staffing and move bidirectionally through the stages.
Knowledge and understanding of SARS-CoV-2 continues to progress at a rapid pace. This has resulted in changes to dental specific SOPs, alongside modifications to practice across a variety of healthcare stakeholders. For example, evidence based alterations, such as the reduction in fallow time and increased use of ‘reusable’ fitted respirators or ‘hoods’, have helped dentists safely increase clinical capacity. 30 As guidance continues to be updated, it is hoped that dental services can continue to recover securely.
Conclusion
This paper has outlined the approach to delivering urgent dental care during the COVID-19 pandemic. It has highlighted the challenges and learning, alongside a conceptual model to facilitate recovery of NHS dentistry, until it is possible to return to ‘normal’. In this instance, learning has been iterative, and required at a rapid pace. Indeed, experiences from within LSC will help inform future pandemic planning, both in dentistry and the wider healthcare arena.
At the time of writing, there is hope for a full return to pre-COVID capacity within NHS dentistry, as a mass COVID-19 vaccination strategy has commenced UK-wide, from 8 December 2020. Continued cross-organisational working in the future by PHE, NHSEI and their partner organisations will ensure that services are suitably reflexive to required changes. This will be necessary to successfully address any issues which arise within NHS dentistry during COVID-19 recovery and beyond.
A flexible strategy moving forward is essential, ensuring that dental services can continue to operate, while gradually increasing capacity through the final stages of the pandemic. The experiences summarised in this document show the need for consideration of wider reform across NHS dentistry in the near future, underpinned by public health principles. This will ensure that any potential increased oral health needs among the population are managed successfully by the service.