
Abstract
In response to the nationwide lockdown on 23 March 2020 in the UK, urgent dental hubs (UDHs) were established in the community to provide emergency dental care.
Consecutive referrals to a primary care UDH were prospectively analysed over a one-month period, from 18 May 2020 to 18 June 2020.
Of 400 referrals received, the most common were in relation to pain (87%). In 63% neither a radiograph nor photograph was provided with the referral. Seventy percent of patients were telephone triaged within 24 hours of receipt of referral. Fifty-three percent of referrals were accepted for face-to-face treatment, of which 69% were treated by extraction. Of rejected referrals (n=179; 45%), 79% were due to symptoms having settled or being manageable by the time of triage. A small number of referrals were redirected for specialist care. Referrals that were accepted were more likely to have been prescribed antibiotics and less likely to have been referred by the general dental practitioner (GDP) they regularly saw (p <0.01).
Patients that were older and those that identified themselves as not having a regular GDP were less likely to have been referred to an UDH. The quality of referrals was poor and there may be a role for virtual consultations moving forwards. We found pre-referral antimicrobial prescriptions were high and a confused public health message may have been sent.
Learning Objectives
To understand the types of cases referred to the urgent dental hubs during the COVID-19 pandemic
To identify areas for future service improvement for dental emergencies in primary care dental practice
Introduction
On 11 March 2020 the World Health Organization (WHO) declared the outbreak of COVID-19 a pandemic, following substantial infection rates and deaths globally. 1 As cases increased in the UK, a national lockdown was imposed on 23 March 2020. Dental professionals were among those most at risk of contraction and transmission of the COVID-19 causing virus, SARS-CoV-2, in the community and clinicians were asked to down tools.
The national lockdown necessitated only essential dental care to be carried out. Urgent dental hubs (UDHs) were therefore established in the community to provide emergency care while reducing inappropriate potential exposure to SARS-CoV-2. This was critical to prevent patients from attending and overloading emergency departments (EDs) as well as to reduce the risk of hospital admissions. A range of conditions recommended for referral were outlined by NHS England (See Table 1).
NHS England Recommendations for Referral
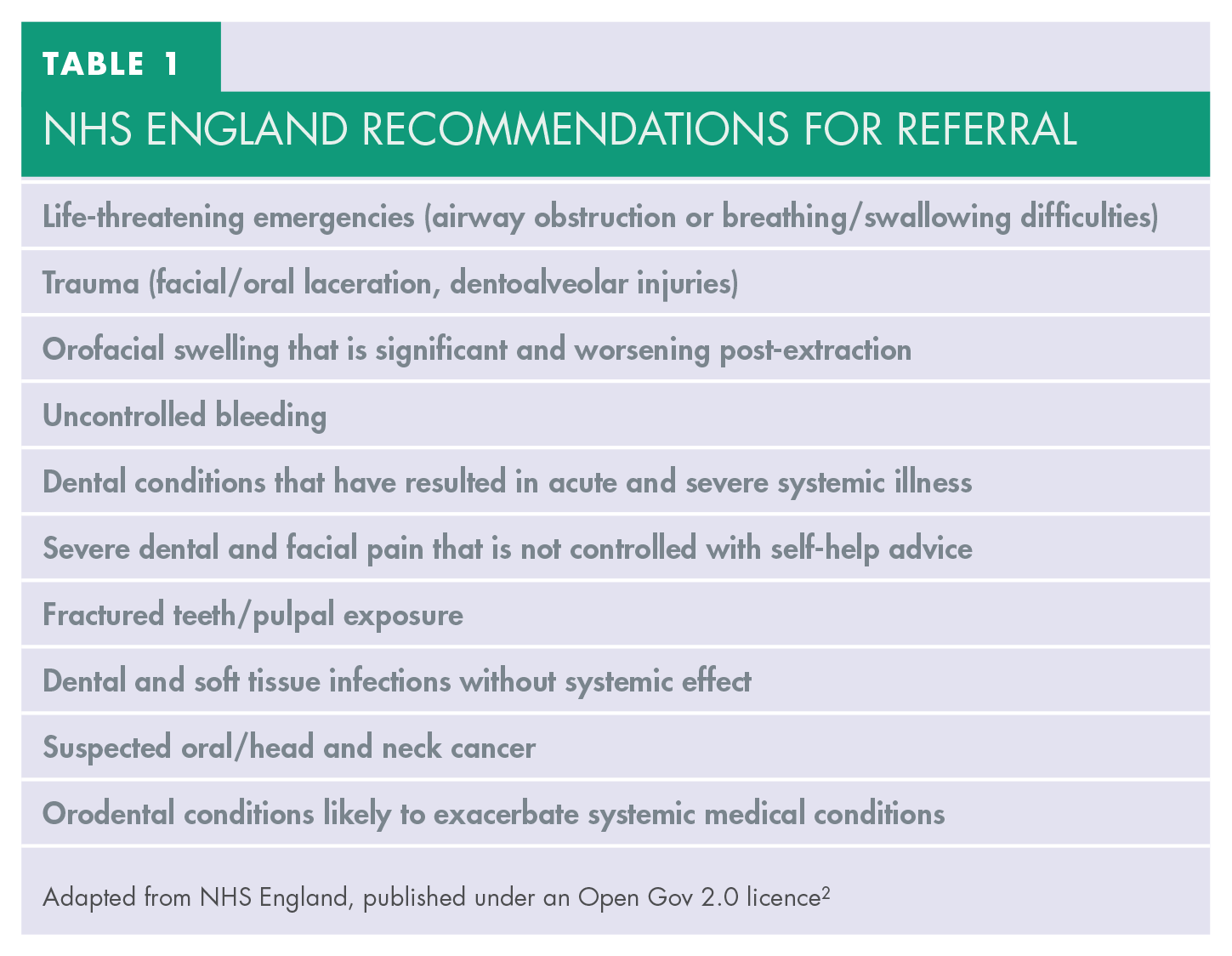
Adapted from NHS England, published under an Open Gov 2.0 licence 2
Subsequently the UK has experienced one of the highest death rates from COVID-19 worldwide. 3 Although the immediate need for UDHs has reduced, the risk of future outbreaks remain. It is likely that some form of this service will be required going forward. Furthermore, primary care dental practices will have to learn from the experience of the UDH to safely manage their own at-risk groups as a model for handling dental emergencies. Telemedicine triaging services have not been commonly used in primary care but were integral during these exceptional circumstances and may play a role in future provision. The aim of this study was to evaluate the referral practices and outcomes of referrals received at an UDH in the South East of England.
Methods
Maidstone Dental and Implant centre was one of 40 UDHs established in the South East of England to provide emergency treatment. Referrals were sent via the Dental Electronic Referral Service online (Vantage Ltd). This is a centralised online electronic referral management system utilised in the region.
Consecutive referrals were prospectively assessed from 18 May 2020 to 18 June 2020. All patients were contacted via telephone by a triaging dentist within 24 hours of referral. Two triaging clinicians were employed throughout the study period. If a patient did not respond, a message was left and they were followed up each day after this until a response was received. Data collection included: patient demographics (age, gender); source and reason of referral; whether antibiotics had been prescribed; supporting information sent (radiographs, images, indication of site of symptoms); time taken to first contact and triage the patient; outcome (rejection or accepted for face-to-face assessment); treatment undertaken if seen face-to-face and reason for rejection if not accepted. The criteria for referral acceptance were based on NHS England guidance (See Table 1).
Data analysis
Statistical analysis was undertaken using IBM SPSS® Statistics software (version 25). A chi-squared (X 2 ) test was used to investigate whether categorical variables differed significantly from one another and an unpaired t-test for parametric continuous data. The significance level was set at α=0.05.
Results
400 referrals were received over the study period. Of these, 48% (n=192) related to male and 52% (n=208) to female patients (male:female 0.9:1.0). The age distribution of referrals is shown in Figure 1. The median age of the entire cohort was 37 years (range 2 months – 78 years).
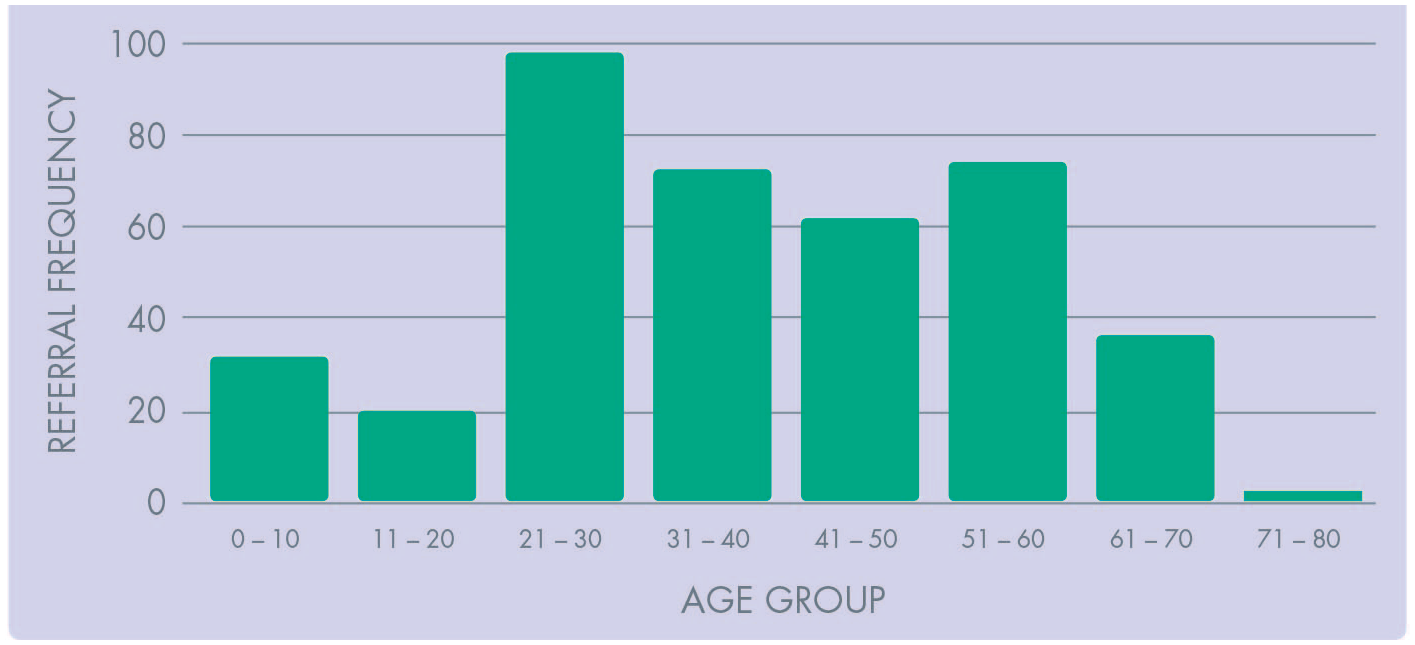
Patient Referral Frequency by Age Group.
278 patients (70%) were triaged within 24 hours of referral, 313 (78%) within 48 hours, 354 (86%) 72 hours, and 377 (94%) 5 days, with a maximum time to telephone triage of 8 days. For 17 (4%) referrals, contact was not possible.
336 (84%) referrals were from a dental practice that the patient regularly attended, with the remaining 64 (16%) from an emergency dental service or practice that the patient had not regularly attended. The most common reason for referral was pain (347; 87%), followed by swelling (42; 10%) and trauma (11; 3%). In 252 (63%) neither a radiograph nor photograph was sent with the referral; in 119 (30%) a radiograph alone, 20 (5%) a photograph and 9 (2%) both a radiograph and photograph were sent. In 343 (86%) referrals the location of symptoms was specified. 305 (76%) of patients referred had been prescribed antibiotics.
211 (53%) referrals were accepted for treatment, 179 (45%) were rejected and 10 (2%) redirected to a Community Dental Services hub site for specialist care. Of those accepted, 146 (69%) had a tooth extraction, 16 (8%) advice was given, 13 (6%) extirpation, 12 (6%) a filling and in 24 (11%) the patient no longer wanted an appointment or failed to attend. Of rejected referrals, 141 (79%) were due to symptoms having settled or being manageable by the time of triage, in 23 (13%) it was not possible to contact and the remainder (15; 8%) were rejected either due to treatment already having been completed elsewhere, the referral was unclear or a non-dental service was required.
Patients prescribed prior antibiotics and those referred by a source other than their regular GDP were more likely to be accepted (p<0.01 for both). No other variables were associated with referral acceptance (age, gender, referral reason, supporting information inclusion, time to triage).
Discussion
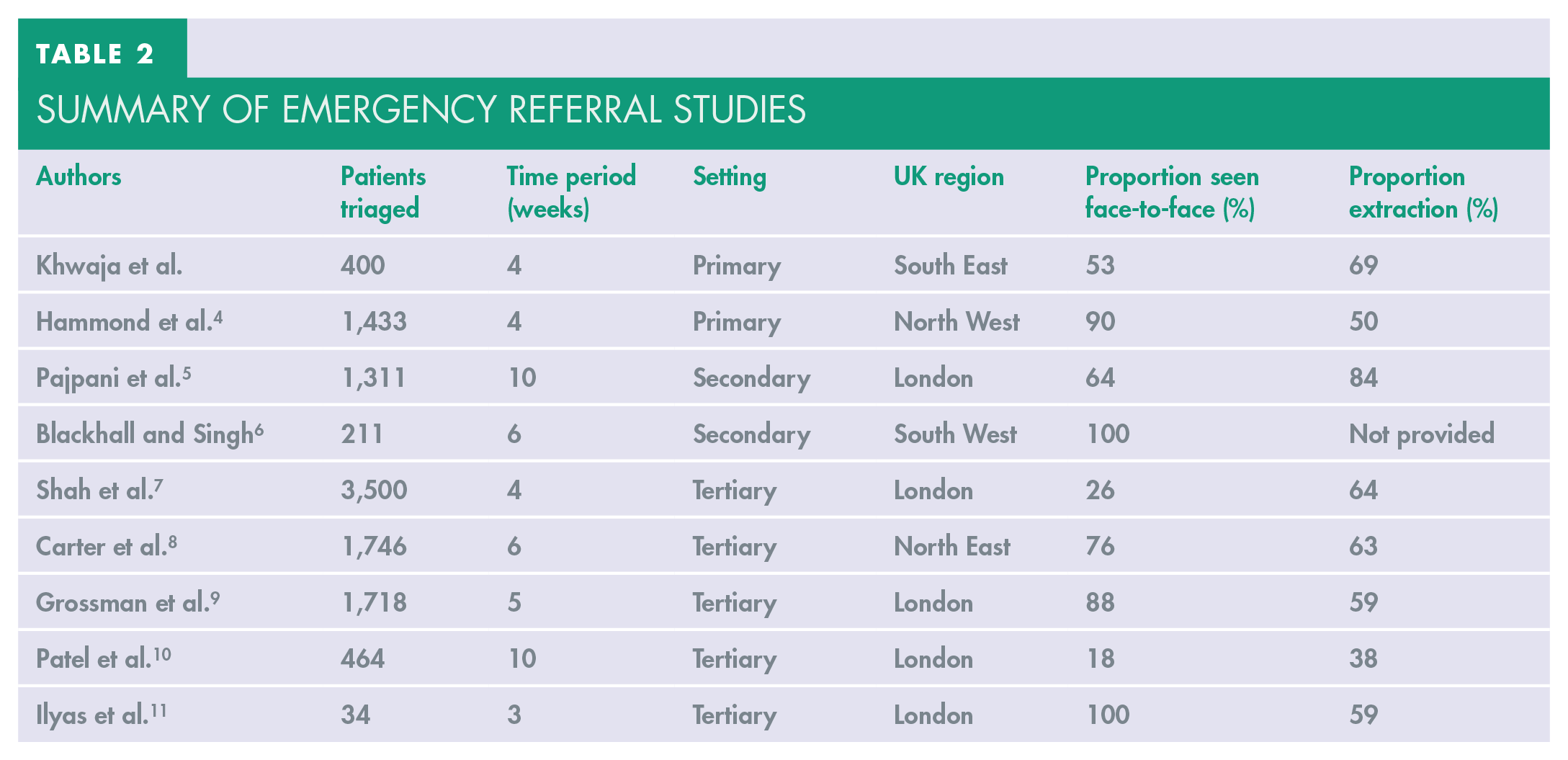
These exceptional circumstances were the first instance in which teledentistry has been considered mandatory to the safe running of an emergency service in the UK. Our evaluation reviews the effectiveness of this system with a view to inform future services during and beyond the pandemic. To the authors’ knowledge, this is the second reported study of referrals to a primary care UDH during the COVID-19 pandemic in the UK, with 400 patients triaged over one month. Unlike the presented service, Hammond et al. 4 report data from a large primary care centre providing specialist Tier 2 oral surgery services with practitioners allied to secondary care services. All other studies have reported on findings from hospitals and may not reflect the experience of primary care. A summary of emergency referral studies is shown in Table 2.
Summary of Emergency Referral Studies
The benefits of teledentistry have been discussed in the literature in terms of clinical effectiveness, cost-efficiency and patient access. 12 The significant benefit during the pandemic was the ability to triage patients remotely, reducing inappropriate patient contact and thus minimising the risk of COVID-19 transmission to staff and patients. Furthermore, from our experience, staff from at-risk groups or those self-isolating contributed to the workforce by remote triage from home. Our results highlight the effectiveness of the service to rapidly contact emergency patients. Time to triage has not been reported in the literature elsewhere, however we found that the majority of those referred were contacted by the UDH within 24-hours (70%). This may have potentially reduced inappropriate ED attendance and hospital admissions, thus avoiding unnecessary burden on stretched secondary care services. A short communication (n=19) compared the attendance for dental abscesses to ED 2-weeks before and after guidance for GDPs to cease routine treatment. 13 Those seen for dental infections were more likely to require admission as in-patients. The authors suggested that patients avoided hospitals because of a fear of contracting COVID-19 and thus presented with swellings later. This emphasises the potential role of UDHs in the early management of these patients.
The median age of patients referred was in keeping with other reported literature.8,6,9 Increasing age is a risk factor for adverse outcomes related to COVID-19 and was well publicised by the UK government. This may have influenced the decision of patients contacting their dentists, with those perceived at greater risk due to age less likely to seek referral. Only 0.75% of referrals were for those aged 70 years or above. This appears at odds with literature from ED attendance prior to the pandemic, in which attendance among this vulnerable cohort was higher, ranging from 1.6–3%.14,15 This cohort may have potentially been affected by dental symptoms but did not access primary care services. Of note, during the study period no confirmed cases of COVID-19 among staff or patients visiting the hub were reported. With appropriate personal protective equipment, staff training and social distancing measures, a safe and efficient service was provided. This service could potentially have been utilised more for this vulnerable cohort (>70 years).
Most of those referred to the UDH self-declared as having a GDP that they regularly visited and were referred by (84%). The remaining patients were referred from an emergency dental service or dental practice that the patient had contacted for the first time. Similar results were highlighted by Carter et al. 8 who found that 81% of those who accessed their service reported having a GDP they regularly contacted. Given that the NHS report under half of the adult population (47%) had seen an NHS dentist in the prior 24 months, our data highlights that our UDH was disproportionately utilised by those with access to a regular GDP. 16 Further supporting data would be welcomed to confirm this, as this may identify an underserved vulnerable population that has not been reported elsewhere. Without a regular GDP these patients may have been unaware of our service. Of note, patients referred without a regular GDP were significantly more likely to be accepted for treatment (p<0.01). The triaging clinician may have had a lower threshold for accepting patients without a regular GDP to ensure appropriate safety-netting and follow-up.
Acceptance rate varied among other secondary and primary care sites and may reflect regional and age specific services (Table 2). Of 400 referrals, 53% were accepted for face-to-face consultation and treatment, 45% were given advice and deemed not to require a face-to-face consultation and 2% redirected to a community dental site for specialist care. Of accepted referrals, 70% had tooth extraction. Our results are broadly in keeping with published data from other hub sites in which the majority of patients were treated with extractions.4,8,5,7,9,11 This is unsurprising given the recommended national guidance was to avoid aerosol generating procedures as far as possible. Ultimately this decision was made between the treating dentist and patient.
The quality of referrals to a UDH has not been reported elsewhere. A significant benefit of digital systems is that they allow for the easy attachment of supporting information such as radiographs and photographs as well as the requirement of mandatory information to be included before a referral can be sent. We found the quality of referrals to be poor with limited information or supporting details provided. In 30% of referrals a radiograph was sent, 5% a photograph and 14% no information pertaining to the site of symptoms were given. It is possible that the presenting complaint was entirely new so a previous radiograph may not have been available to send. When radiographs were sent these allowed the triaging clinician to assess the likely treatment required as well as the complexity of the case. Patients could then be booked with a specialist oral surgeon, if necessary, and thus prevent unnecessary travel to the UDH. Photographs were rarely sent but provided critical diagnostic information, particularly regarding the presence or extent of facial swelling. Possible reasons for not including photographs may be that referring GDPs do not have the facility to take photographs or have time pressure in a busy clinical environment. A role for video consultations has been proposed to overcome this. 10 High patient satisfaction rates have been reported when utilised in a dental hospital setting.17,18 NHS England have procured the licence to use a video consultation system (Attend Anywhere®) for use by NHS trusts in secondary care settings. Although commonly available in general medical practices, utilisation of these systems in a primary dental setting appears minimal. Our experience supports the use of these systems. Further research is required to identify feasibility and potential barriers, including patient concerns.
The reasons for rejection of face-to-face assessment have not been documented in previous reports. Of those rejected in this article, the vast majority were due to symptoms having settled or being considered manageable by the time of triage (79%). This high proportion may be the result of a stricter interpretation of what necessitated an urgent appointment by the triaging clinician than the referring GDP. Some authors have recommended a scoring framework for identifying dental emergencies during the current pandemic. 19 This is based on the severity of the oral condition, systemic health and anxiety. Although this has not been validated in any patient group, the mandatory completion of such a scoring system on digital referrals may aid decision making. It is possible that patient symptoms had settled by this point and therefore were deemed not to fit the criteria for an urgent appointment. This data supports the recommendation of GDPs following up all patients 24 hours after initial contact before considering referral to the UDH. This would have potentially decreased the number of rejected referrals.
The inappropriate use of antibiotics for patients suffering from dental pain has long been a concern. To our knowledge, the use of antibiotics prior to referral has not been reported elsewhere in the literature. The majority of patients (76%) referred in this study had been prescribed at least one course of antibiotics. This is of note given that swelling only accounted for a minority of referrals (10%), whereas most were referred for dental pain (87%). This should be considered in the light of the requirement for all face-to-face activity to immediately cease and a “3As” (Advice-Analgesia-Antimicrobial) where appropriate strategy at the time of study, employed. Indeed, antibiotic prescribing was 25% higher in England from April to July 2020 compared to the previous year. 20 Consequently, there is a risk that a confusing message has been sent to both patients and clinicians given the longstanding public health campaign that antibiotics do not cure toothache. Others have observed that the 3As approach would have been better colloquialised as the “4As” approach (Advice, Analgesia and, if Appropriate, Antimicrobials) to more explicitly highlight the continued need for judicious use of antibiotics when treating acute dental conditions. 8 This would encourage dentists to consider the suitability of prescribing, rather than as a routine step in the management of dental pain.
There is limited data published from primary care UDHs during the first COVID-19 UK national lockdown. In order to evaluate the applicability of our findings it would be prudent to compare our results with other regions in the UK. Two researchers triaged all the patients during the study. No formal calibration was used for this process and thus a risk of inter-researcher bias was present.
Conclusion
Given the unprecedented circumstances, the use of teledentistry was central to provide an emergency service in a primary care setting. During the study period there was a high demand for services with the majority of patients contacted within 24 hours of referral. We found patients >70 years of age and those that identified themselves as not having a regular GDP as less likely to have been referred to our service. The quality of referrals was poor and there may be a role for virtual consultations, moving forwards. We found pre-referral antimicrobial prescriptions were high and a confused public health message may have been sent. Overall, we were able to establish a safe and efficient primary care emergency service. This model may be useful to provide care in future emergency situations as well as having a potential role in targeting other underserved populations.