
Abstract
Regular dental attendance is a key oral health behaviour. Behaviour change interventions are increasingly being used to promote positive oral health behaviours. A systematic approach to understanding behaviour has led to the development of frameworks which aim to guide the process of designing behaviour change interventions. One such framework is the Behaviour Change Wheel (BCW). This article aims to explore and identify barriers to regular dental attendance which may be targeted using behaviour change interventions based on the Capability, Opportunity and Motivation Behaviour model (COM-B) and the BCW, and suggests potential behaviour change techniques which could be utilised into a behaviour change intervention with the aim to promote regular dental attendance.
Learning Objectives
To understand biopsychosocial factors behind urgent only dental attendance
To appreciate the theoretical basis of the Behaviour Change Wheel and COM-B Behaviour model
Introduction
Regular dental attendance is a key oral health behaviour.1,2 A regular attender is defined as someone who attends for routine dental check-ups, regardless of their dental needs.3,4 The National Institute for Health and Care Excellence (NICE) recommends all adults should have dental recalls between three months and two years, based on their oral health risk.5,6 Urgent only or non-regular attenders are those who attend for dental care when they have a specific dental problem. 3 In the UK, 39% of adults are not regular dental attenders, which means a significant proportion of the population do not receive preventative advice, regular oral cancer screenings or timely intervention of dental disease.6,7,8 Non-regular dental attendance is associated with poorer oral health compared with those who do regularly attend.3,4,7,9 Dental attendance patterns have been shown to vary by factors such as age, gender and socioeconomic status6,10,11,12 but the most common reasons provided for not attending the dentist regularly are concerns over the cost of treatment, anxiety and a lack of perceived need.9,13
Behaviour change interventions have been used to promote positive oral health behaviour changes14,15 and have been shown to be more effective when the underlying theory is understood and applied.16,17,18 Behaviour models aim to provide an understanding of behaviour, and with the provision of oral health care shifting towards a biopsychosocial model, the relationships between individual and environmental factors behind an urgent only attendance pattern need to be understood to assist dentists and dental care professionals in the development and implementation of targeted behaviour change interventions to promote regular dental attendance. 15
Behaviour change interventions
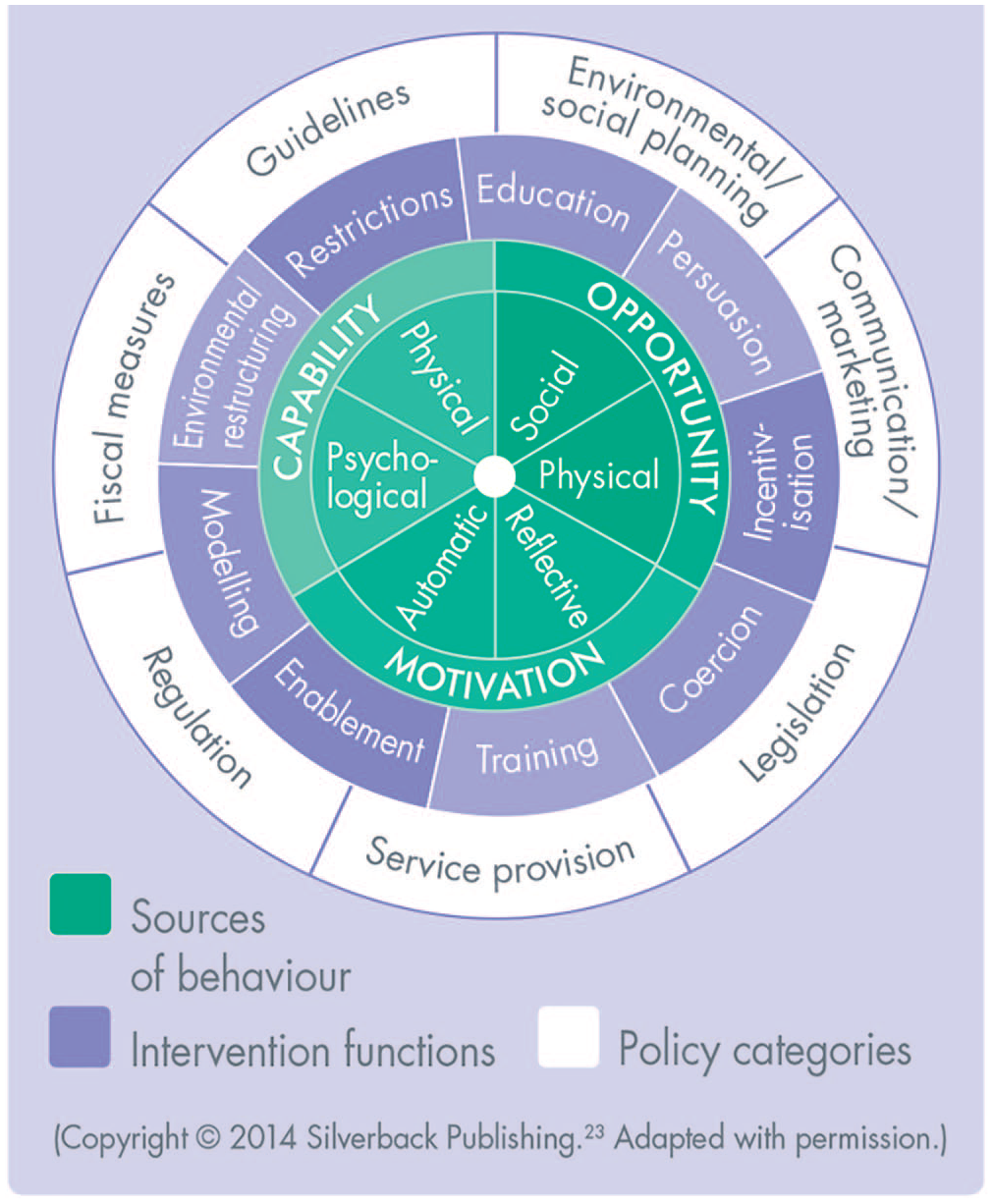
Historically, oral health promotion has relied on education alone in the form of giving information to patients on oral diseases, but this has not been shown to change behaviour. 19 Oral health promotion has shifted towards the application of behaviour change interventions to promote positive health behaviour changes.14,20,21,22 Traditional behaviour models such as the Health Belief Model or the Transtheoretical/Stages of Change model have been shown to be unreliable in guiding behaviour change. 17 There are many different theories of behaviour change but little guidance on how to choose an appropriate theory for a particular behaviour. This has been cited as a reason why theory is underused in intervention design and implementation of behaviour change techniques. 23 A systematic approach to understand the individual components or barriers to change a behaviour has led to the development of frameworks, which combine multiple and often overlapping theories on behaviour change and aim to guide and simplify the process of developing evidence-based behaviour change interventions. One such framework is the Behaviour Change Wheel (BCW) (Figure 1), which is based on the COM-B model of behaviour (Figure 2).17,23,24
Behaviour Change Wheel
COM-B Model of Behaviour
Behaviour Change Wheel (BCW) and the COM-B model
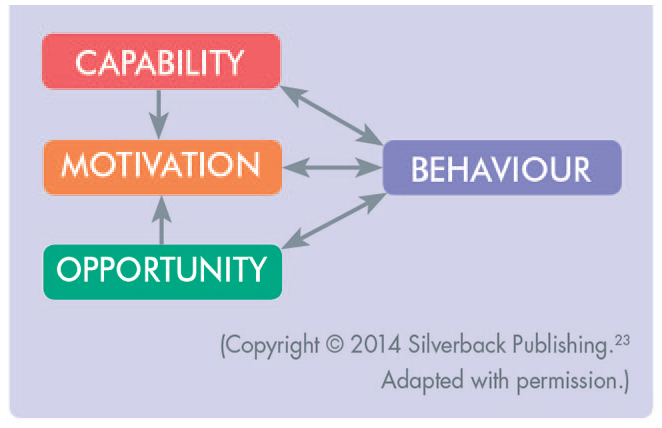
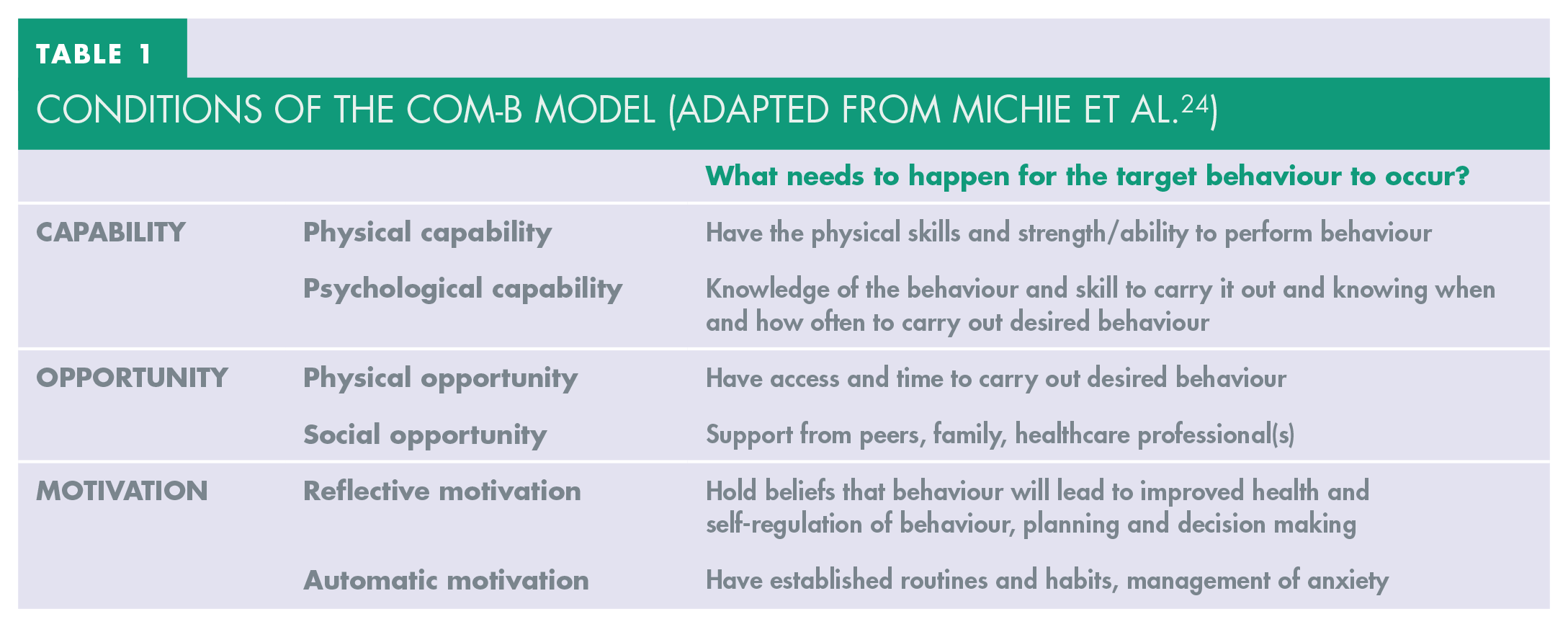
The BCW is a tool used to design behaviour change interventions based around the COM-B model, which explains that behaviour consists of three interrelated factors – capability, opportunity and motivation (Figure 2). Before the desired behaviour can take place the person must feel they are psychologically and physically capable, they must have the social and physical opportunity to carry out the behaviour, and they must have a desire or motivation to carry out the behaviour (Table 1). Any attempt to change behaviour should aim to address one or more of these components. 24 The second layer of the BCW links the three COM-B factors to ‘intervention function’ groups with suggested evidence-based behaviour change techniques to consider. Seven ‘policy categories’ make up the outer layer of the BCW, and are used to identify the method of delivering the behaviour change intervention on a wider population level. 24
Conditions of the COM-B Model (Adapted from Michie et al. 24 )
Behaviour change interventions in dentistry
Within dental research, there has been an uptake in the application of behaviour change models and frameworks (such as the COM-B model and the Theoretical Domains Framework 25 ) to help in understanding the antibiotic prescribing behaviour of dental clinicians, 26 the promotion of oral health advice among professional athletes 27 and in the design of interventions to promote positive oral health behaviour in patients with periodontal disease.19,20,21,28 However, there has been little research, to date, on the use of behaviour change interventions to promote dental attendance. Behaviour change techniques such as ‘action planning’ and ‘coping planning’ have been shown to increase dental attendance in patients with low dental anxiety levels. 29 The provision of written material to reinforce verbal advice has also been shown to improve attendance. 30 There is a need to consider, develop and clinically evaluate behaviour change interventions which target regular dental attendance on an individual patient level, which clinicians can implement in practice and on a population level. The reporting of behaviour interventions has improved with the introduction of evidence-based frameworks and the Template for Intervention Description and Replication (TIDieR) guide checklist 31 but clinicians looking to employ behaviour change interventions into their practice should understand the theoretical concepts in the design of behaviour interventions, in order to critically appraise which behavioural interventions are effective in different contexts.
Developing behaviour change interventions
The following information is to inform dentists and dental care professionals on the process behind developing behaviour change interventions based on the COM-B model and the BCW.
Understanding the behaviour
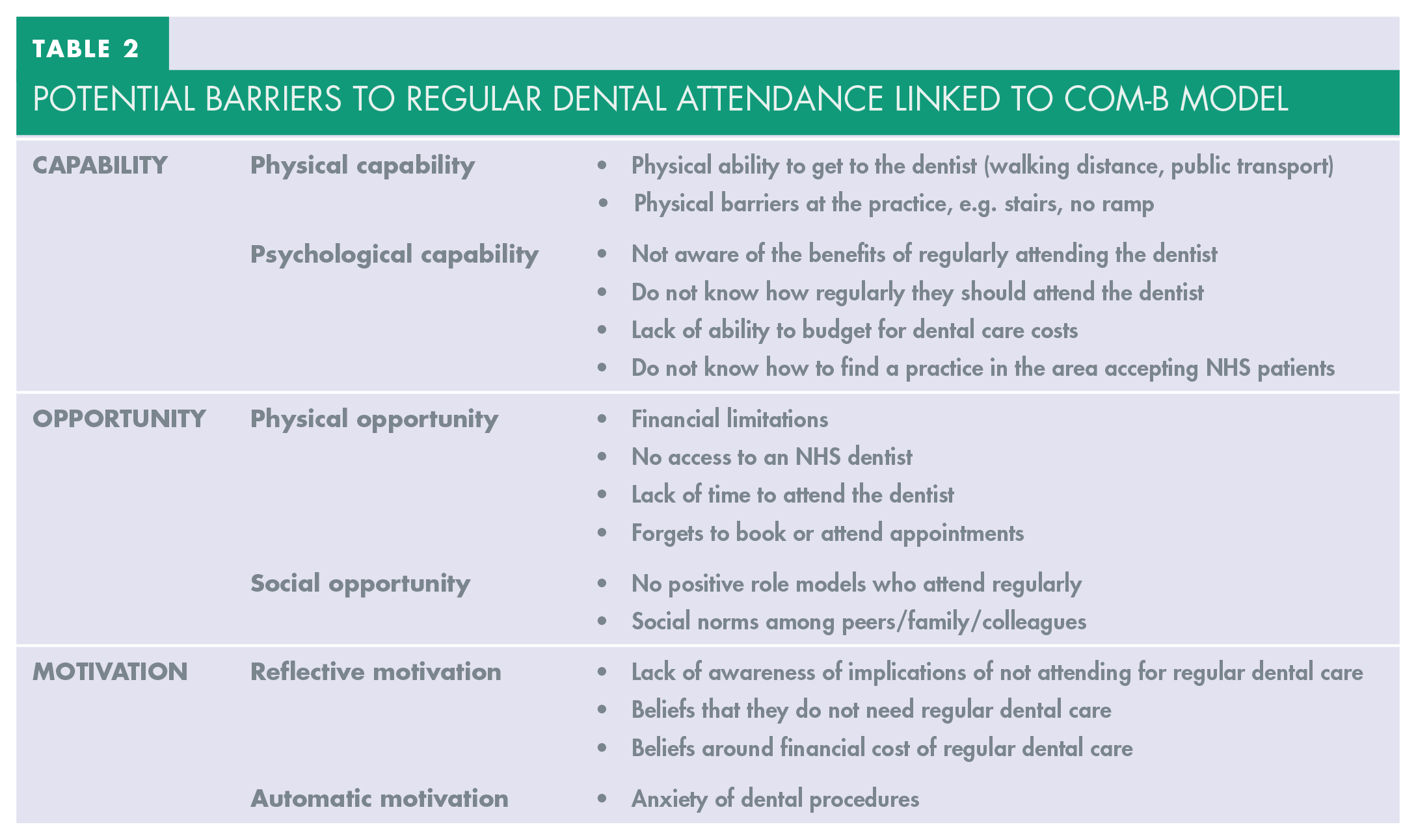
When developing a behaviour change intervention, the first aim is to understand the behaviour and identify any barriers to the target behaviour. A clinician encountering an urgent only attender should assess the patient’s capability, opportunity and motivation to become a regular attender. 24 Attending for regular dental care is a complex behaviour with many underlying factors, such as not knowing how often to attend (a psychological capability factor), or a reported lack of time (a physical capability factor). Some of the factors behind urgent only dental attendance behaviour, linked to the COM-B model, are listed in Table 2. Not all the factors behind urgent only attendance may be modified or addressed through these processes, so clinicians should aim to address one or two barriers and target the barriers which are most likely to lead to a change in behaviour. 24
Potential Barriers to Regular Dental Attendance Linked to COM-B Model
Identifying appropriate behaviour change techniques
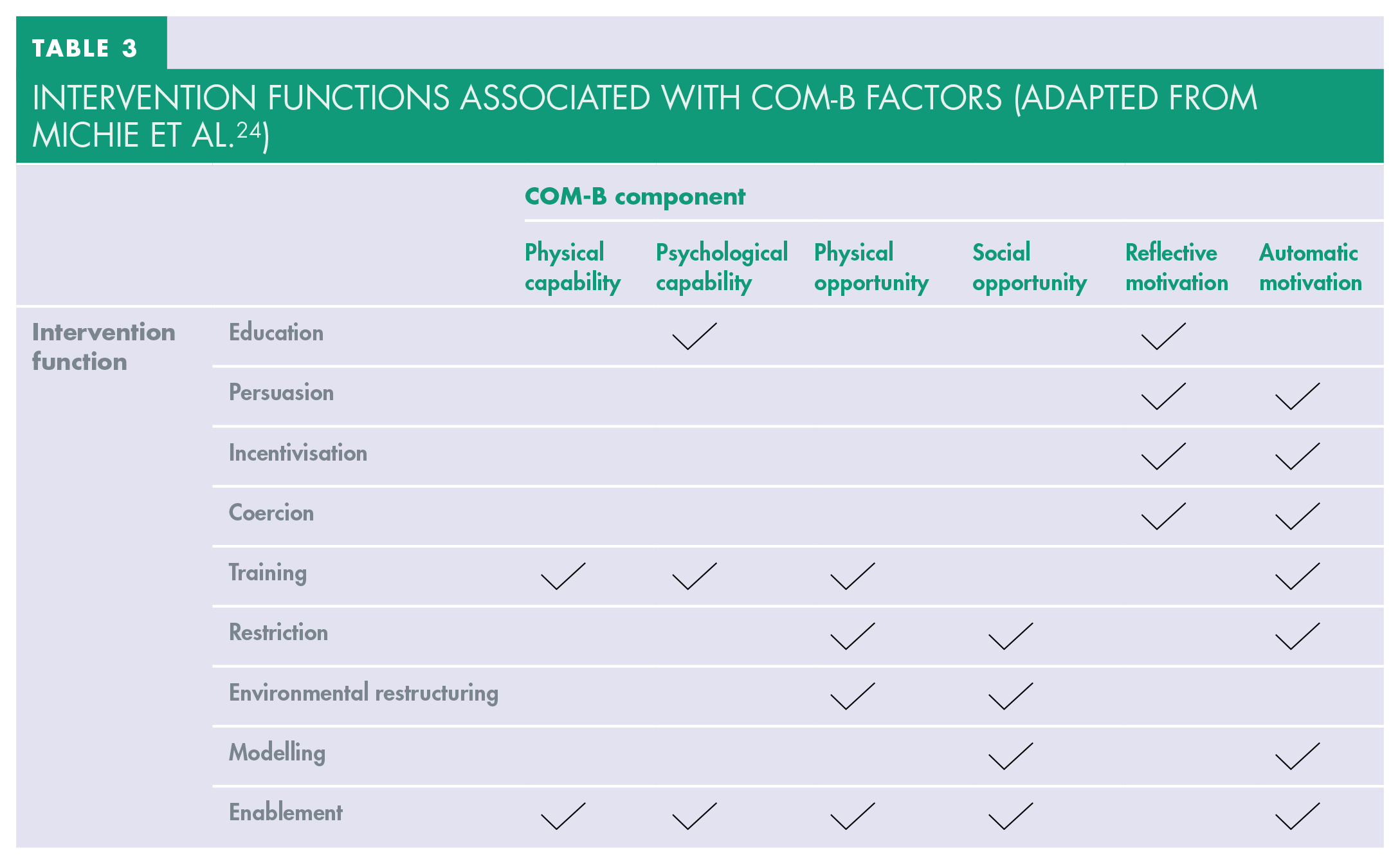
Once there is an understanding of the barriers to the target behaviour, the BCW can be used to identify which intervention function group linked behaviour change techniques are most appropriate to remove the barrier or facilitate the behaviour (see Table 3). Each intervention function is linked to effective evidence-based behaviour change techniques – the “active” component of a behaviour change intervention which aims to modify a process that leads to a certain behaviour.23,24,32
Intervention Junctions Associated with COM-B Factors (Adapted from Michie et al. 24 )
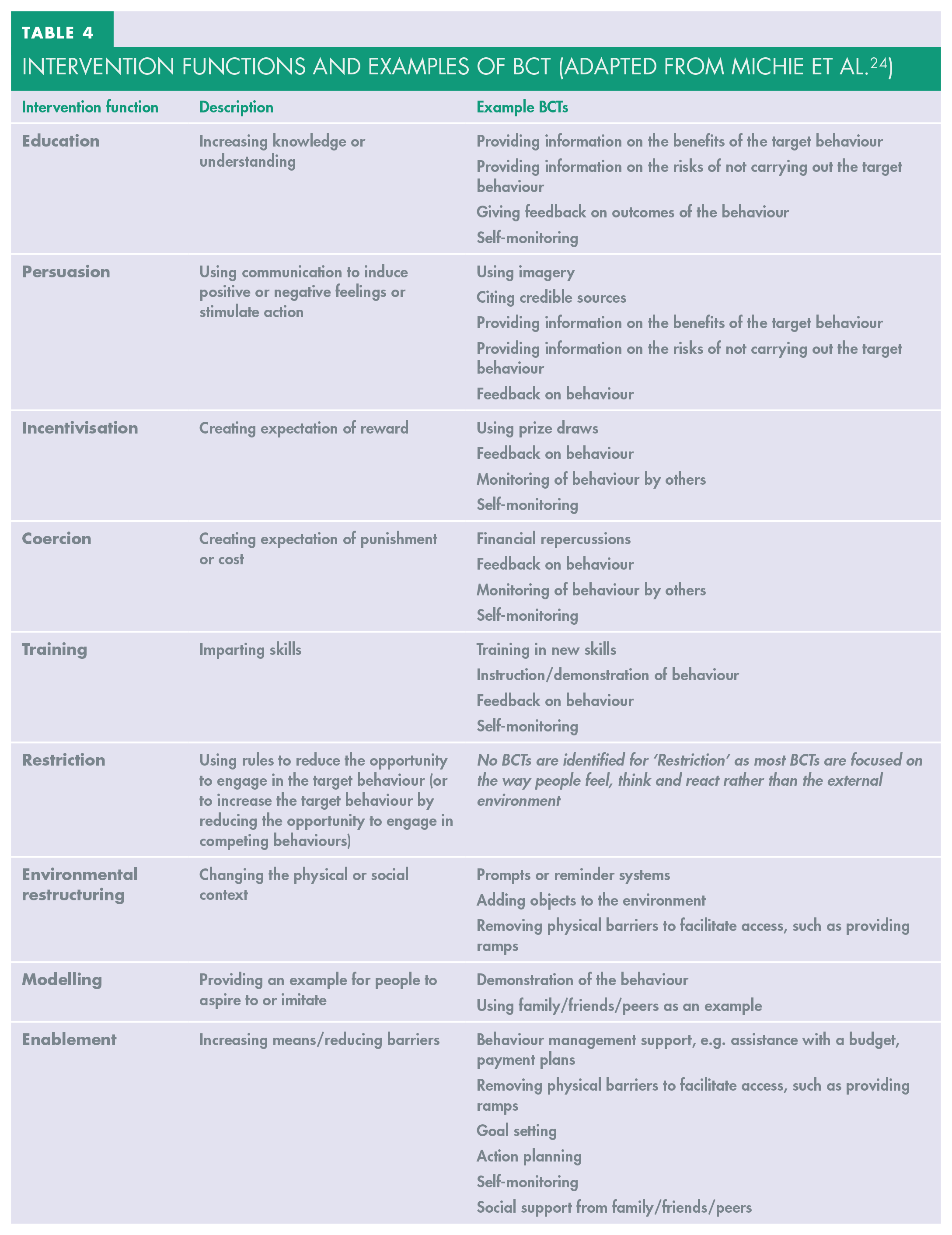
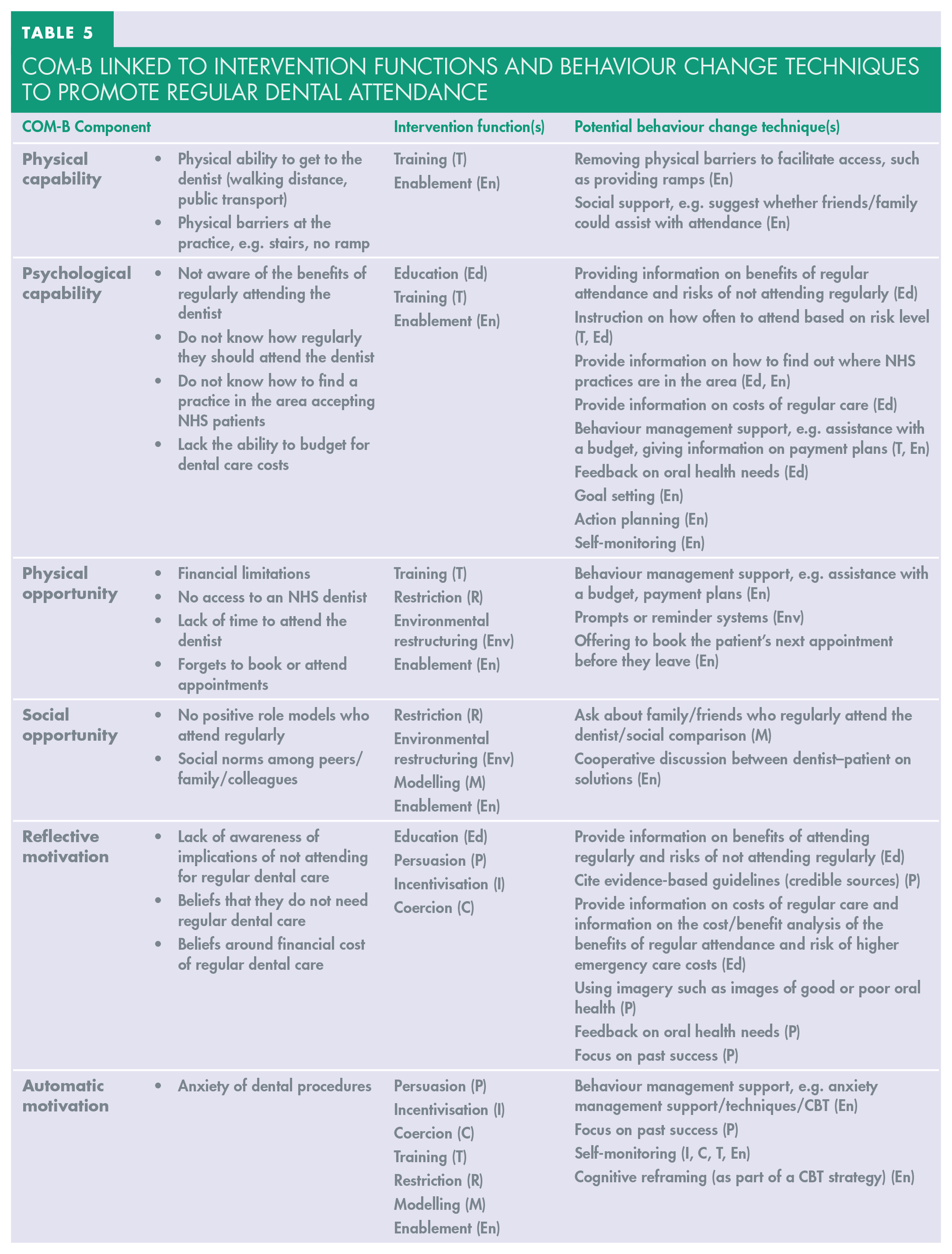
A behaviour change taxonomy (BCT) app is available (BCT Taxonomy, compatible with iOS/Android) which identifies and groups 93 behaviour change techniques into intervention function categories, and was developed by the BCT Taxonomy Project. 33 Commonly utilised behaviour change techniques by intervention function type are shown in Table 4. Some behaviour change techniques can be considered for more than one intervention function type. Theory-based behaviour change techniques that could be used in a behaviour change intervention to promote regular dental attendance are shown in Table 5.
Intervention Functions and Examples of BCT (Adapted from Michie et al. 24 )
COM-B Linked to Intervention Functions and Behaviour Change Techniques to Promote Regular Dental Attendance
Identify mode of delivery
Once the target barriers and appropriate behaviour change techniques have been identified, the mode of delivery can be determined. The most suitable modes of delivery appropriate to an emergency dental appointment are verbal through face-to-face contact or in written form, such as a leaflet, to reinforce the verbal advice and provide information the patient could take away, as there is often limited time available. Interventions could be developed which utilise social media. To maintain regular dental attendance, interventions which can be implemented over time may need to be developed.
Summary of the behaviour intervention design process
Conclusion
The COM-B model is used to identify ‘what’ behaviour needs to be altered, and the BCW helps us understand ‘how’ this might be possible. To achieve the aim of having a population with a healthy functioning natural dentition throughout life, dental clinicians involved in providing care to urgent only attenders should look at employing behaviour change interventions grounded in evidence-based theory to promote regular attendance. Behaviour change interventions are more successful when the underpinning theory is understood and applied, therefore it is important that dental clinicians are knowledgeable on the theory behind behaviour change and keep up to date with developments in behaviour change sciences.17,20,21
Further research is required on the development of behaviour change interventions in oral health promotion and on their clinical effectiveness, at an individual patient level and at population level. Training opportunities and robust research providing an evidence base on the development and implementation of behaviour change interventions in clinical dental practice would allow more uptake of these strategies by dental clinicians.