
Abstract
This paper highlights the process of transition to a female majority for dentistry, examines various influences on this trajectory, and considers the implications for the profession, health systems and patients, as well as individual dentists.
This celebratory transition has been facilitated by educational systems that provide both males and females with equal opportunities and is supported by legislation, as well as societal change that has spanned decades. In crossing this gender representation threshold, we have outperformed doctors nationally.
In order to embrace our highly educated workforce and support them to better serve their patients and the population, urgent debate and action aimed at reshaping current systems of dental care provision are required. In this regard, flexible working arrangements, together with reshaping professional leadership to better represent the workforce, as well as changes in terminology can all play their part; however, we will need careful discussions about how this might happen effectively.
A collaborative effort between the dental profession and wider health systems is required to ensure that there are opportunities for everyone to flourish and contribute back to the profession and society. Our medical counterparts have been considering how healthcare should be shaped creatively, particularly in relation to working patterns, economic models and quality patient care: we need to catch up.
Learning Objectives
To understand the changing gender balance in dentistry in the UK
To recognise remain gender inequalities in leadership roles and specialties
To reflect on the possibilities to make positive changes in the way dentistry is provided for patients and members of the dental team
Introduction
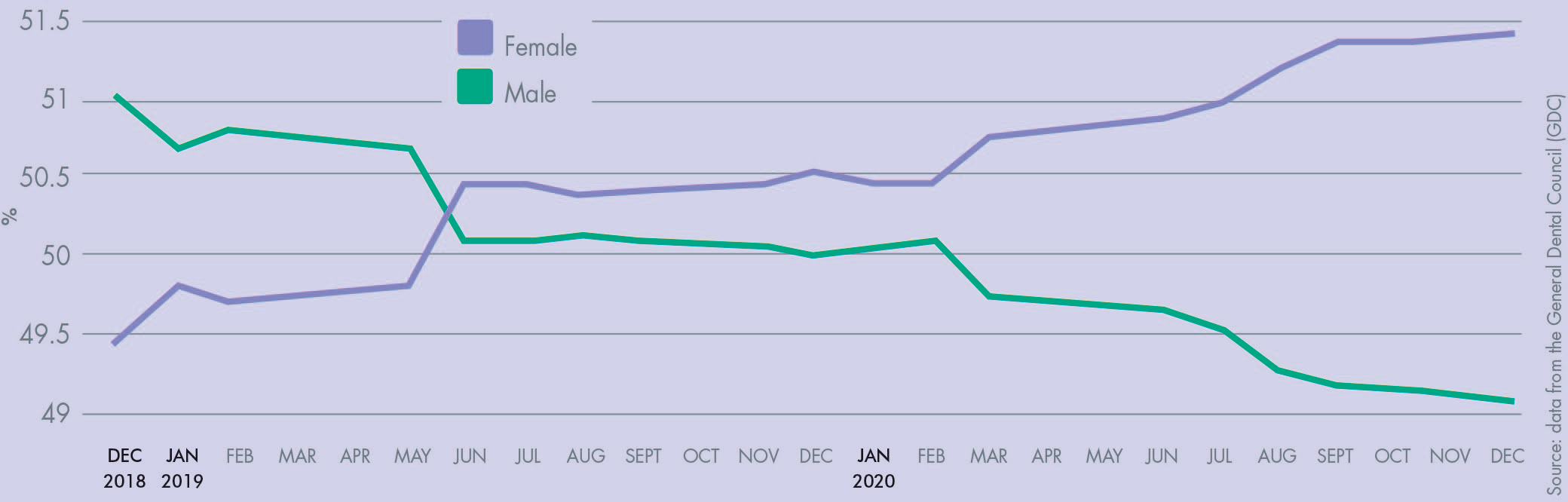
The dental profession was established with, by, and for, men in the United Kingdom, in line with the culture and professional norms of the day. It has been changing slowly over time as women were permitted to study and practise dentistry; thus, the 5,831 dentists registered in 1921 were virtually all men, whereas in December 2020 the majority of the 43,007 registered dentists are female. 1 Whilst some events are heralded, the transition to a female majority in dentistry in the UK has largely happened silently. In 2012 the Health and Social Care Information Centre estimated that by 2020 half of all UK dentists will be female. It happened six months earlier than predicted. 2 According to registration data held by the General Dental Council, the UK reached a 50% female workforce in June 2019, with the gap widening and heading towards a clear 51%/49% split by January 2021, 3 as presented in Figure 1. In this respect, we have made this transition ahead of our medical counterparts, where currently 46.3% are female. 4
UK Dentistry Workforce Transition
It is not just in the UK that we have seen increases in the number of women applying to, studying, qualifying, and practising as dentists over the past 50 years. This is a phenomenon in many western countries globally. Prior to the 1970s, fewer than 3% of American dentists were female, the lowest percentage in the western world. 5 By March 2020 in the USA, women accounted for 33% of practising dentists according to the Kaiser Family Foundation. 6 In Europe as a whole, women accounted for more than 60% of all practising dentists by 2016 (Women Dentists Worldwide 2016), with almost four in five dentists in Finland, Russia, Latvia and Lithuania identifying as female (Carlisle 2015). This reflects fundamental differences between countries in the west, and those in eastern Europe, where dentists traditionally come from a stomatological, rather than an odontological background; and where the majority of professionals in caring professions including dentists and doctors, have traditionally been female. 7
At this point it is important to recognise that our wider, and increasingly professionalised dental workforce is predominantly female (notably dental hygienists, dental therapists and dental nurses), 3 particularly considering their current sentiments for better recognition within dentistry.
Access to the university and the profession: representation at all levels?
It is helpful to consider dentistry in the wider context of university and the profession when looking at patterns. Early dental qualifications came through the Royal Colleges, and it was only later that medical and dental education was provided through universities. The pattern for dental education was part of the wider emancipation of women providing access to university education, degrees, and the professions, 8 and remains so today.9-12 In so many of these developments, we have followed, or at least paralleled, developments amongst our medical colleagues.
The first female dentist in the UK, Lilian Lindsey (née Murray) was reluctantly permitted to join Edinburgh Dental School, having been refused entry or even a proper interview by the National Dental Hospital in London. 13 This meant that she had to incur the challenge of studying away from home, with the resultant cost implications. Such was her determination that she did this, and won prizes along the way. Her story is interesting in that even she had a mentor, who inspired her to pursue a career in dentistry: a female German dentist, and family friend, who had qualified at the University of Pennsylvania in America and then worked in London. 14 Prior to qualifying as a dentist, Lindsey worked as a technician to gain the relevant experience. She practised in London to work off her student debt for a decade prior to marrying and returning to Edinburgh to work alongside her husband Robert Lindsay before they both returned to London. Lilian went on to become the honorary librarian of the newly created British Dental Association [BDA] and sub-editor of the British Dental Journal, contributing much to the profession over her working life. She was elected the first female president of the BDA in 1946, at a time when women were increasingly being accepted into dental schools, and will have been an inspiration to others along the way.
Dental students
Last summer (2020), 62% of dental school admissions in the UK were female. 15 Niven et al have examined dental and medical school applications and admissions over the last 20 years, identifying trends in sociodemographic, academic and geographical influences on dental and medical admissions in the UK.9-16 Females are more likely to apply in the first place and then to be accepted; the odds of admission are significantly higher for females than males. 9 The transition from a male majority entering dentistry to a female majority occurred in the mid 1990s, and has consistently been the case for dentistry with the exception of 1998. 17 Medicine exhibits a similar trend, albeit there are minor annual changes (Figure 2); and, of course, this largely parallels the pattern of university applications and admissions.11,12,16

Proportion of female entrants to UK Medical and Dental Schools (Home EU and International Students), 1990-2020
Research on motivations for entering the profession amongst final year dental students reported a wide range of factors influencing their choice of dentistry as a career. Features of the ‘professional job’, followed by ‘healthcare and people’ were the most important underlying factors influencing choice of career. 18 These influencing factors varied by sex, ethnicity and mode of entry, but the only difference of note was that males were more interested in the business of dentistry. 18
Access to education and the professions does not always translate to representation across all levels, however, and the gender split across education, primary dental care and the specialties, and academia tells a more nuanced story, which will be considered below.
Primary dental care
The majority of dentistry is delivered in primary care and women are now in the majority on the front line. Interestingly the NHS statistics suggest that women dentists work slightly shorter hours than men but have slightly better morale. This could be attributed to the fact that they have a better work life balance through a combination of working shorter hours and taking more annual leave. Whilst this result initially suggests that the motivation of female dentists is less affected by their working patterns than that of their male colleagues, the fact they tend to work fewer weekly hours (33.5 compared to 38.4 hours) may play a role. 19 Low morale and thoughts of leaving NHS dentistry are very prevalent amongst male and female dentists, however, and must be addressed if we are to retain our workforce.19-24
Dental specialties
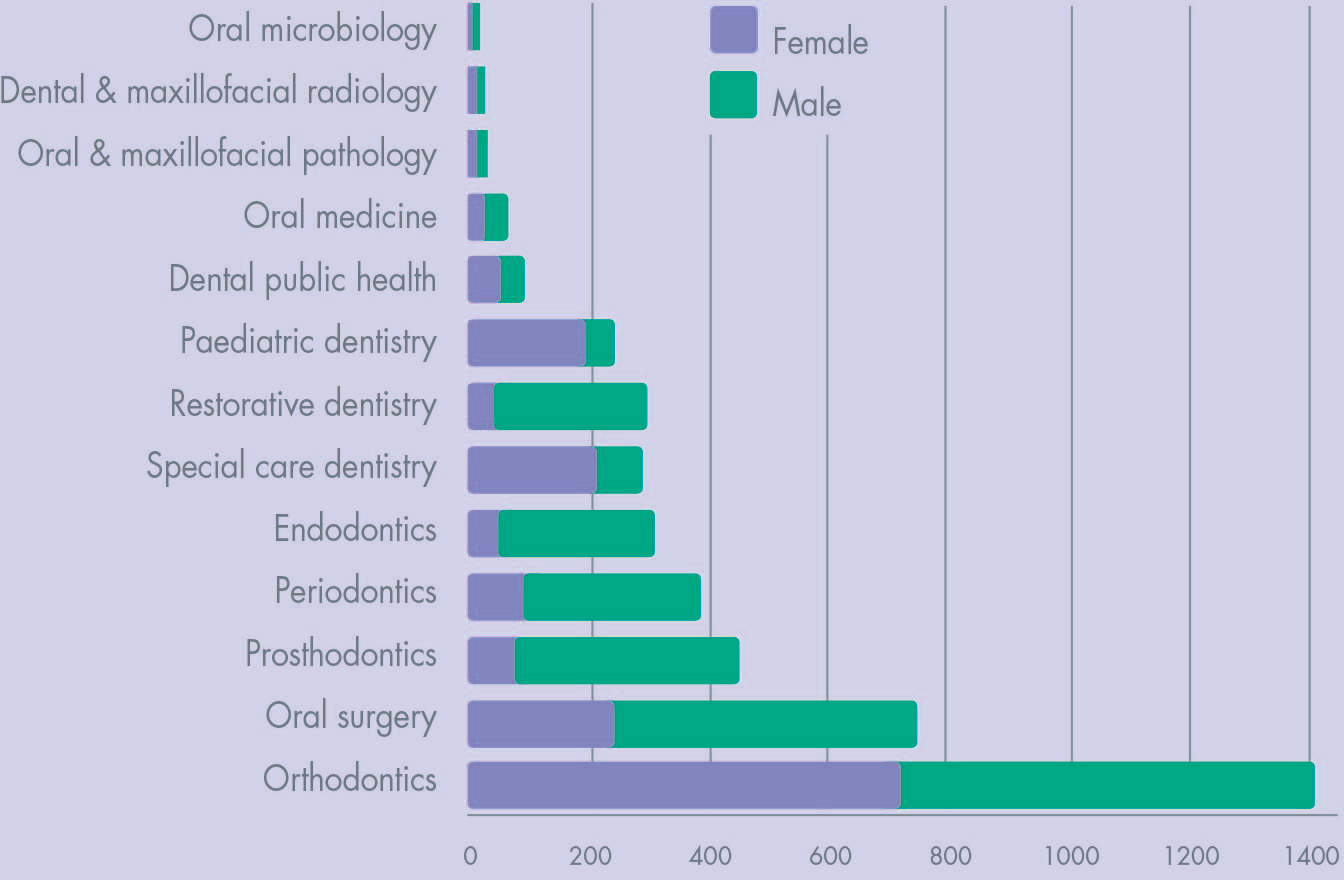
By December 2020 women outnumbered men in six of the 15 dental specialities including oral microbiology, dental and maxillofacial radiology, paediatric dentistry, and special care dentistry, while men still dominate in the specialities which are perceived to have higher status. Over two thirds of dentists in oral surgery are male and approximately three in four dentists specialising in prosthodontics (73%) and restorative dentistry (76%) are male (General Dental Council 2021). This parallels challenges in general surgery, which the Royal Colleges have been tackling in recent years.
UK Dentistry Specialists by Gender, December 2020
Academia
Female representation in dental academia is increasing: professor (22%), senior lecturer (42%) and lecturers (58%), but the gradient remains clear and steep. Representation of women within clinical teaching roles is also progressing, albeit more slowly: senior clinical teacher (44%) and clinical teachers (46%), but with a much shallower gradient. 25 A similar proportion of males and females works less than full-time in academia; but this is complicated by the heavy use of clinical teachers on a part-time basis who also carry out other roles in practice. 25 In clinical academia, women present a younger age profile than male clinical academics. Given the length of time it takes to train as a clinical academic, this is encouraging for future representation. Support will be needed, however, throughout the process of career development, 26 and particularly where there may be a lack of flexibility to relocate for career progression and the need to seek internal promotion.
The practice of dentistry
Most dentists are ‘generalists’ working in primary dental care, some with extended education and skills. Recent research suggests that there is strong interest amongst practitioners in gaining ‘extended skills’ training. 27 Only about 10% of the profession go on to gain specialist status following further education and training, and fewer still become clinical academics. This development is partly constrained by training positions. There is little recent research in the field on gender in dentistry, albeit NHS surveys seek to understand work patterns over time by country, system and position in the practice.19 -21 Historically, research suggests that there are minimal differences in working hours between men and women prior to ‘career breaks’, but female dentists are more likely to take such breaks and are more likely to reduce their hours once they return to work afterwards. 28 Largely due to this, male dentists tend to contribute more working hours across their careers than female dentists. This ties in with the findings of a study by McKay and Quinonez (2012) which drew on Canadian data, suggesting that male and female dentists differ in a number of ways, with women working fewer hours, seeing fewer patients and being less represented in leadership roles or academia. 29
A study focusing on vocational dental practitioners in the U, conversely found that the financially lucrative nature of the career, job security, professional status and flexible working were key features amongst both men and women choosing to practise as dentists. While changes in healthcare provision were posing a potential threat to their visions, their expectations “were closely linked with their personal lives and support a vision of a favourable work-life balance.” 30 Similarly, in a study of the dental profession in Ontario, Adams and Lynn (2005), found very few differences between men and women in attitudes towards, and characteristics of, practice. 31 It was found, however, that women are more likely to work as associates, whilst men are more likely to work as solo dentists and that women dentists earned around 60% of their male counterparts’ earnings, even where hours worked were broadly similar. 31
As outlined above, one potential gendered difference in practice relates to career breaks; however, over 60% of female and just over a quarter of male dentists in the UK reported taking a career break two decades ago. 32 It is worth noting here that the term ‘career break’ is itself gendered, as it is used to be shorthand for women taking maternity leave and carries connotations of women being less dedicated to their careers by virtue of their biology. Changing legislation which facilitates paternity leave, and a change in terminology to favour parental leave may help to tackle this.
The nature of dental practices is also changing and this needs to be factored into any discussion and analysis of the future of dental provision. Looking ahead, most dental practices are likely to be run by a small number of corporate bodies or conglomerates. The proportion of dentists holding a provider role within the NHS sector continues to decline. 33 If the current trend to a reduced number of organisational providers continues, however, future dentists are unlikely to end up running their own dental practice and are more likely to work within systems which could potentially provide the opportunity for flexible working. That said, many will require periods of parental leave during their childbearing years and there is emerging evidence in the current English contractual system that this presents challenges for practice owners in delivering their NHS contracts.22,23 This creates challenges which the system will have to face in the redesign of dental care in light of the disruptions caused by COVID-19. Particularly in parts of the country where workforce capacity is low, it may not be possible to obtain locum cover and practices should not be financially penalised for employing women of a childbearing age. System redesign must include making this workable for our female workforce and practice principals and owners.
The feminisation of dentistry
Professions can be described as occupations which have some combination of social status and social power (authority), that involve formal qualifications/credentials and years of study, and that have a large degree of autonomy, either through self or institutional regulation. 34 Many of these occupations can be found in the field of healthcare, and traditional healthcare professions have developed around a clear gender division, with women historically prevented from training or practising as doctors or dentists. Furthermore, Adams and Lynn suggest that women’s healthcare work was often concentrated in ‘semi-professions’ such as nursing and dental nursing, which supported the male dominated healthcare professions but did not have the autonomy and status on the male dominated professions. 31 Over the past 50 years, however, increasing numbers of women have been studying, qualifying, and practising in traditionally male dominated healthcare professions such as medicine and dentistry. This change in the gender balance led to discussions about the ‘feminisation’ of healthcare. In its simplest form this refers to the movement of women into male dominated professions. 35 For some, however, reference to feminisation reflected a presumed change in the nature of the work itself and the status ascribed to that work. The suggestion is that when professions become female-dominated, this changes the nature of the profession and the services it provides. 36
The rise in the number of women qualifying and practising as dentists has led to a debate about the ‘feminisation’ of dentistry as a profession, both in numerical and characteristic terms, and to some discussion about the implications of this feminisation on the future of the profession and the provision of dental care. Bedi and Gilthorpe recognised that dentistry was going through the gender transition in the 1990s, and suggested that “this development will have implications for workforce capacity in the longer term”. 17 Whilst, as we have shown, more women are now qualifying and practising as dentists in the UK than men, there is a clear gradient when it comes to representation at the higher levels. In relation to the characteristics of dentistry and dentists, McKay and Quinonez suggested that the ‘feminisation’ of dentistry could lead to dentists being less entrepreneurial, more focused on the work-life balance, and could lead to the availability of fewer hours of clinical time available for patients. 29 Drawing parallels with work on professionalism in medicine, 37 Adams and Lynn suggest however that, rather than increasing numbers of women in dentistry changing the nature of the profession, women are moving into dentistry in increasing numbers at a time when dentistry is undergoing change in the same way that medicine is. 31 Calls for flexible working practices which cater better to the needs of patients and the dental team, person centred care, increased public access to expert knowledge and a decrease in the authority ascribed to doctors and dentists, 34 all form part of the backdrop against which increasing numbers of women have moved into dental and medical practice. Adams and Lynn further suggest that the characteristics of the profession that made it popular for men, are the very ones that women are seeking: the job security, status ascribed to the role, expert knowledge and a fulfilling role. 31
The changing nature of the workforce, coinciding with the changing nature of the demands on the profession could provide the catalyst needed for change. Generational differences are important to acknowledge along with gender. 38 In parallel with our medical colleagues, we must recognise the challenges that this presents. First, that the NHS will get a lower return from the number of doctors or dentists that it trains if people work part-time. Second, leadership capacity needs to be built in, as elite leadership positions have traditionally involved more than full-time working, often out of hours. For clinical academics, combining research, teaching and specialist care in part-time working is very difficult; however, we have a bigger pool of talent than ever. Third, the possibilities of a two-tier system emerging between those working full-time and those working part-time is something that needs to be avoided, with its implications for workforce satisfaction and patient care. And in the process of addressing these challenges, along with our medical counterparts, we must celebrate the successes of women so that their stories are recognised too. 39
Moving forward
The data presented here suggests that, whilst more women are studying, qualifying and practising as dentists in the UK now, they remain under-represented at higher levels in practice and in academia, and the representation is very uneven across the dental specialties. As dental services change and reorientate to address the inherent weaknesses in the system exposed by COVID, there is the chance to harness the current and emergent workforce and serve population needs better. 40 Maybe as we work towards longer clinical days, there will be greater opportunities for people working less than part-time to join forces to care for groups of patients, and share the necessary cover of key holiday periods. This is an opportunity to think creatively, on two fronts, for the workforce and for the patients.
Restructuring dentistry to build in flexible working practices, parental leave, to make practices more family friendly and to build-in strategies for covering maternity leave in particular, will all work to boost the morale of the workforce. Reform to facilitate opportunities for career development and promotion will also help, as well as providing supportive environments with clear career paths, while increasing the numbers of women in leadership roles acting as mentors and role models. 26 This will reduce turnover and the number of dentists seeking to leave NHS practice, and so improve the care provided for patients. Embedding person centred care into future practice to address the increased public access to expert knowledge, and a decrease in the authority ascribed to doctors and dentists, will also help create clinical encounters which better meet the needs of both dentists and their patients. However, making this work for patients, where people are working less than full-time, requires careful consideration and planning.
We may be ahead of our medical colleagues with a female majority; however, it is time that we follow their lead, 41 to consider workforce design, the economic challenges of workforce patterns for patient care, the business of dentistry and the importance of leadership. We also need to explore how we can encourage and support under-represented groups to apply for a career in dentistry.
Footnotes
Acknowledgements
Thanks to Dr Victoria Niven and Manveet Aulakh who assisted with the figures for this document.