
Abstract
Patient safety should be at the heart of any healthcare service. Systems, teams, individuals and environments must work in tandem to strive for safety and quality. Research into patient safety in dentistry is still in the early stages. The vast majority of the research in this area has originated from the secondary care and academic fields. Approximately 95% of dental care is provided in the primary care sector. In this paper, we provide an overview of the evidence base for patient safety in dentistry and discuss the following aspects of patient safety: human factors; best practice; the second victim concept; potential for over-regulation and creating a patient safety culture. Through discussion of these concepts, we hope to provide the reader with the necessary tools to develop a patient safety culture in their practice.
Learning Objectives
To understand contemporary concepts relating to patient safety
To learn examples of best practice which can be incorporated into everyday patient care
To get an overview of resources available to aid practitioners when developing their own patient safety culture
Background
Patient safety in dentistry is an area of active research. The concept of patient safety is best described as ‘the reduction of risk of unnecessary harm associated with health care to an acceptable minimum.’ 1 Much of the research to date has taken place in the secondary care hospital and academic settings. 2 However, the vast majority of dental care in the UK (and indeed globally) is provided in primary care settings. A recent report found that 95% of dental care is provided in primary care, 3 yet almost all of the research on patient safety in dentistry originates from the presumed 5% of care that is delivered in secondary care and academic settings. Indeed, even the research from secondary care settings usually originates from an oral surgery department.
The authors believe that this observation is due to the addition of wrong tooth extraction to the NHS Never Events framework in England in 2015, 4 and the subsequent observation that this has become the most frequently reported surgical Never Event nationally, accounting for between 20-25% of wrong site surgery Never Events.5,6
Concurrently, oral surgery services are being moved from secondary care to primary care following the publication and implementation of the Commissioning Guides since 2015. 7 This move raises questions as to where the research should be conducted in the future. There is no reason that research cannot be carried out in primary care; the authors are aware of studies funded by the National Institute for Health Research (NIHR) which are underway in primary care settings. Given the findings in this paper, we encourage further funding in order to pursue primary care research in dentistry.
This paper aims to provide an update on patient safety for the General Dental Practitioner (GDP), and we a hope to share examples of best practice and tools that may be adapted by GDPs in order to ensure that they are practising in a safe environment with appropriate risk management protocols.
Patient safety in dentistry
Although we have defined patient safety in general, there is still a lack of consensus as to what constitutes a patient safety event or incident in primary care dentistry. 1 Previous attempts have been made to define or categorise patient safety incidents specific to primary care dentistry.8,9 A recent study by Black & Bowie 10 found that the following events may be considered as adverse or never events related to dentistry (listed in order of risk to patient):
Failure to check past medical history
Inhalation or swallowing of a crown or instrument
Restoring the wrong tooth
Oxygen and/or emergency drugs not being available
Allergic reaction due to not checking medical history
Extracting the wrong tooth
Iatrogenic damage to adjacent tooth
Delay in routine referral
Delay in urgent referral
Using dirty instruments
Treating the wrong patient
A further study suggested a similar list of ‘never events’ as applied to dentistry, they also included various forms of iatrogenic harm which can occur during a dental visit. They were in agreement with Black and Bowie that failure to check medical history is the leading cause of harm in dental care settings. 11 These findings are also echoed by studies from the USA.12,13
Human factors
No discussion of patient safety is complete without a full consideration of the impact of human factors on patient safety. The term itself is in widespread use and alludes to the limitations in human performance and how these can adversely affect patient safety. A closer look at the definition places the person or clinician at the centre and examines their interaction between tasks/technology, their team members, and the environment around them. 14
It is essential for one to consider these interactions as they operate independently to clinical knowledge and expertise. That said, we are all susceptible to errors in clinical practice, regardless of our seniority. Instead, our decision-making process has been commonly categorised into ‘Type 1 processing’ (fast, intuitive thinking) and ‘Type 2 Processing’ (slow, analytical thinking); famously presented in Daniel Kahneman’s piece ‘Thinking, Fast and Slow’.15,16
All of those involved in clinical decision-making processes are subject to cognitive bias. Cognitive biases describe our subconscious tendency to behave in a particular manner. There are several examples of cognitive bias that are well documented in medicine. In a 2016 systematic review of cognitive biases affecting medical decision-making, every included study identified at least one cognitive bias which affected clinical decision-making. 17
Common cognitive biases are listed in Table 1 with examples of how these may manifest in everyday dental practice.
Examples of cognitive biases and how they can present in practice
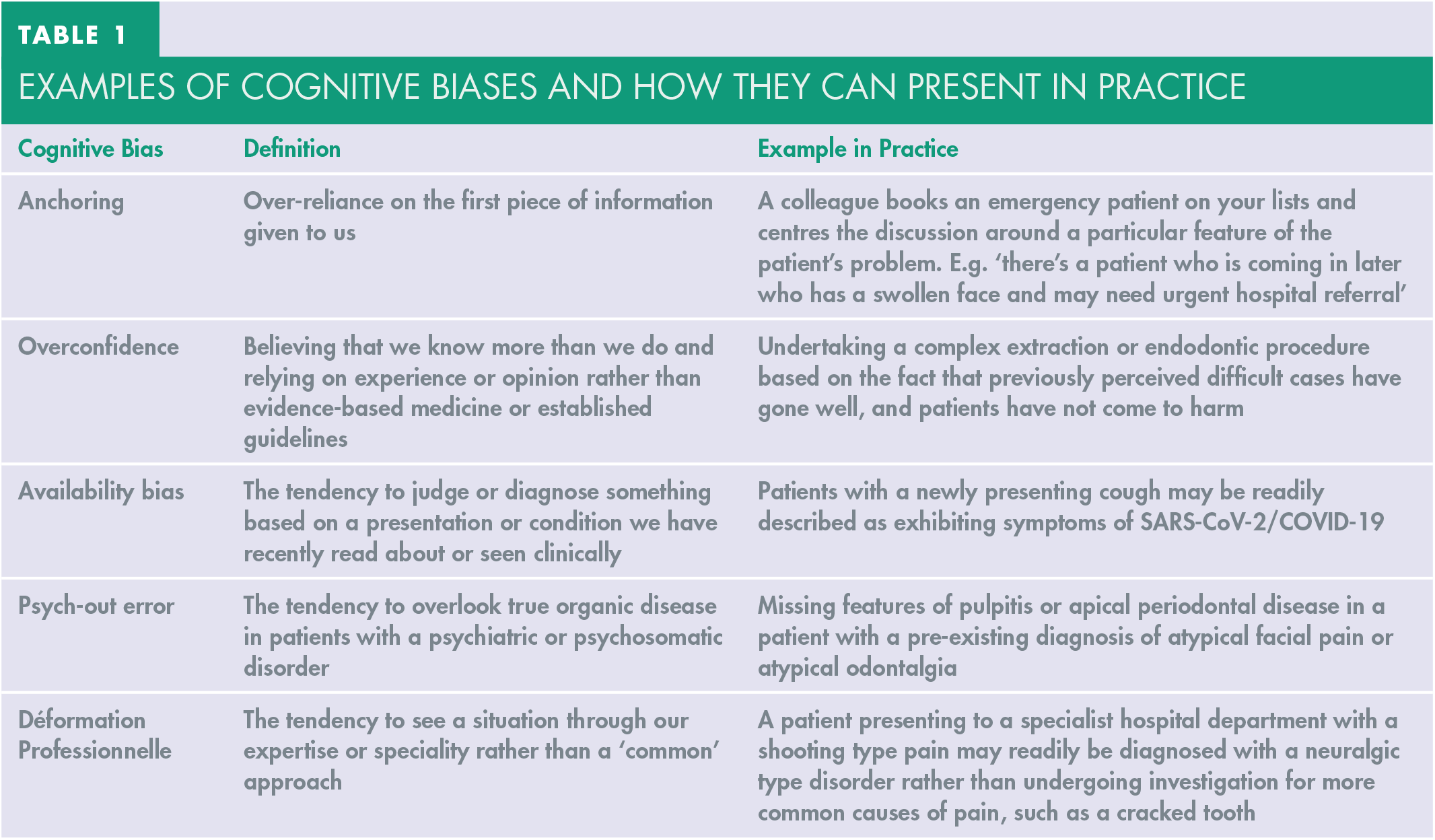
As such, the authors recommend several strategies that can be used to help reduce such biases.
Examples include taking a thorough history and clinical examination to gather information about the patient for one’s self, rather than depending on the information in a referral, from a colleague or telephone consultation. Try to apply evidence-based medicine and adhere to national guidelines before embarking on treatment.
Furthermore, start each case as a ‘clean slate’, obtain a differential diagnosis and then factor in co-morbidities and other aspects that can influence the final diagnosis.
Use checklists before embarking on treatment; this should include patient details, medical history checklists, availability of functioning and in-date equipment/materials.
Consider the use of a team-brief prior to starting the clinic list. This will give every team member an opportunity to voice concerns and an opportunity to discuss parts of the list which may not be ‘routine’ in nature. It will also demonstrate that what might seem obvious to you, may not necessarily be as apparent to other team members. As such, this is an excellent opportunity to ensure all team members are comfortable with what is to be expected. 18
The ‘second victim concept’
The concept of the second victim in patient safety was discussed in a BMJ editorial back in 2000.
19
The second victim is the healthcare provider who is involved in an adverse event or patient safety incident. In Wu’s original paper, he describes the emotions that a second victim might experience following an adverse event:
‘Virtually every practitioner knows the sickening realization of making a bad mistake. You feel singled out and exposed—seized by the instinct to see if anyone has noticed. You agonize about what to do, whether to tell anyone, what to say. Later, the event replays itself over and over in your mind. You question your competence but fear being discovered. You know you should confess, but dread the prospect of potential punishment and of the patient’s anger. You may become overly attentive to the patient or family, lamenting the failure to do so earlier and, if you haven’t told them, wondering if they know’
19
This paper was published 20 years ago, yet the description provided above may still feel pertinent to any dental care professional who has recently experienced an adverse event.
The individual involved experiences emotional distress which is similar to that of the patient involved (the first victim). 20 Scott and colleagues 21 described a six-stage cycle that occurs during the second victim phenomenon, comprising:
Chaos and accident response
Intrusive reflections
Restoring personal integrity
Enduring the inquisition
Obtaining emotional first aid
Moving on
The authors of this qualitative study found that involvement of the second victim in patient safety improvement or advocacy projects helped them to move towards stage 6 more swiftly. Subsequent research in this area has identified a lack of organisational support for second victims and difficulties relating to the investigations of such incidents and the sharing of their findings with the team involved. 20
Neglecting the second victim will not lead to an open culture where clinicians feel free to discuss errors and shortcomings. Second victims require support and a forum to enable them to discuss their emotions. The psychological distress associated with being a second victim can have detrimental effects on cognitive performance and this will impact on patient care. 22 There is, however, a counter argument that states that the term ‘second victim’ should be abandoned as it has led to more focus being placed on the clinician rather than on the first victim or their families. The use of the word ‘victim’ is also contentious – victims bear no responsibility or accountability; they elicit feelings of sympathy. This term may, therefore, be used to mask underlying issues within a healthcare service causing actual harm to patients. 23 Wu himself has revisited the concept and found that the term should be used to encourage the funding of support services for clinicians involved in adverse incidents. However, the needs of the first victim are also extremely important. 24
In summary, the emotional and psychological needs of the clinician involved do need to be addressed. Being aware of these will improve incident reporting and honesty and may be part of creating a ‘patient safety culture’. However, the needs of the first victim must also be a priority and the temptation for the clinician to hide behind the victim label must be countered as this can lead to negative outcomes for patients.
In England, the NHS launched Practitioner Health as part of the NHS Long Term Plan. It was launched in 2017 and extended to dentists in 2019. This is a free, confidential NHS service for doctors and dentists across England with mental illness, stress or depression. 25
Examples of good and suboptimal practice
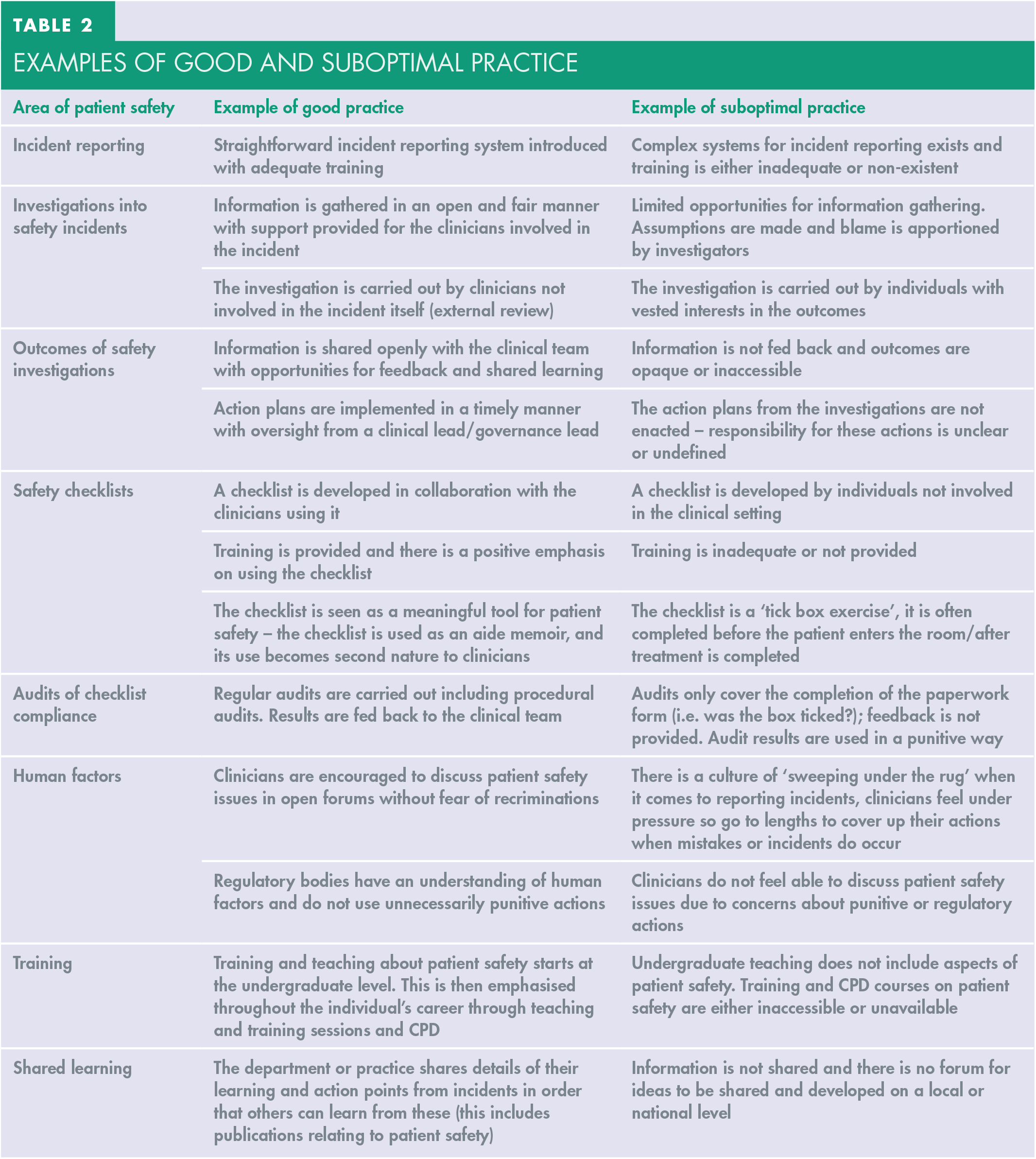
The authors have several years of experience in various oral surgery departments and primary care services. In Table 2, we have gathered some ideas in the hope of outlining what good practice and what suboptimal (or poor) practice looks like in relation to patient safety in dentistry.
Examples of good and suboptimal practice
Potential for over-regulation
In the UK, there is a general feeling that the dental profession is over-regulated at the present time, with evidence showing that litigation cases involving dentists have increased over recent years.26-28 Against this background, it can be difficult to imagine working in a culture of openness where discussion of errors or mistakes is encouraged. The case of Dr Bawa-Garba, the trainee paediatrician who faced punitive actions when a child in her care died in 2011, has acted as an unfortunate counter to the desired culture of openness. One of the features of the case was that her reflections from her training portfolio were used in a court of law. 29
In dentistry, there are examples of practitioners trying to cover up their mistakes when it comes to patient safety incidents. In these two examples,30,31 one practitioner was suspended and the other struck off for lying to investigators when an error had occurred (wrong tooth extraction in both cases). These cases demonstrate, perhaps, the fear that clinicians feel when errors do occur, but they also make it clear that the issue of dishonesty is taken very seriously by regulators. To clarify – the actions taken against these clinicians were due to their dishonesty, and not due to the clinical errors in isolation.
One might think of asking the patients or general public what their opinions are on patient safety and what action should be taken when errors occur. According to a recent GDC survey, 32 49% of the sample surveyed (1,232 respondents) felt that a dentist removing a wrong tooth should either be struck off the register or suspended.
There are recent examples of the profession taking ownership of patient safety. In 2019, after much confusion, it was clarified by NHS England and NHS Improvement that wrong site inferior dental nerve blocks do not constitute Never Events. 33 This is not to say that their occurrence should not be investigated and dealt with as a patient safety incident, as there is always learning to be had from such events.
Creating a patient safety culture
Pemberton 34 suggests four strategic areas for improving patient safety:
Identifying threats to patient safety by incident reporting
Evaluating incidents and identifying best practice
Communication and education about patient safety
Building a safety culture
Incident reporting is a very important tool in developing patient safety strategies. Without incident reporting and learning from mistakes, the profession will never know the extent of the problem.26,35 Research has shown that an increasing number of wrong tooth extractions have been reported from primary care. 5 This practice needs to be encouraged as it is the only way to know the size of the problem and therefore to develop the means for dealing with these issues which affect patient care. Reporting of Never Events occurring in primary care is now mandated and should be escalated via the local commissioners. 35
Surgical safety checklists have been shown to reduce the harm to patients undergoing dental extractions in hospital settings.2,36-38 To date, there are no trials that demonstrate the efficacy of checklists in primary care dental settings. There has been recent debate on the role of checklists for surgery. A recent systematic review found the view that introduction of a correct site surgery checklist will lead to improvements in patient care, is somewhat naïve, and the sociocultural nuances of checklist culture need to be explored in detail to better understand how we can improve in this field. 39 Another study into improving quality and safety in healthcare found that the traditional model focusing on compliance and isolating discreet problems and finding solutions to these in a linear fashion is incongruent with what we know about healthcare. Healthcare is complex and often non-linear. 40
Surgical safety checklists consist of the following stages:
An example of a correct site surgery checklist for dental extractions currently used at a large London teaching hospital is shown in Figure 1.
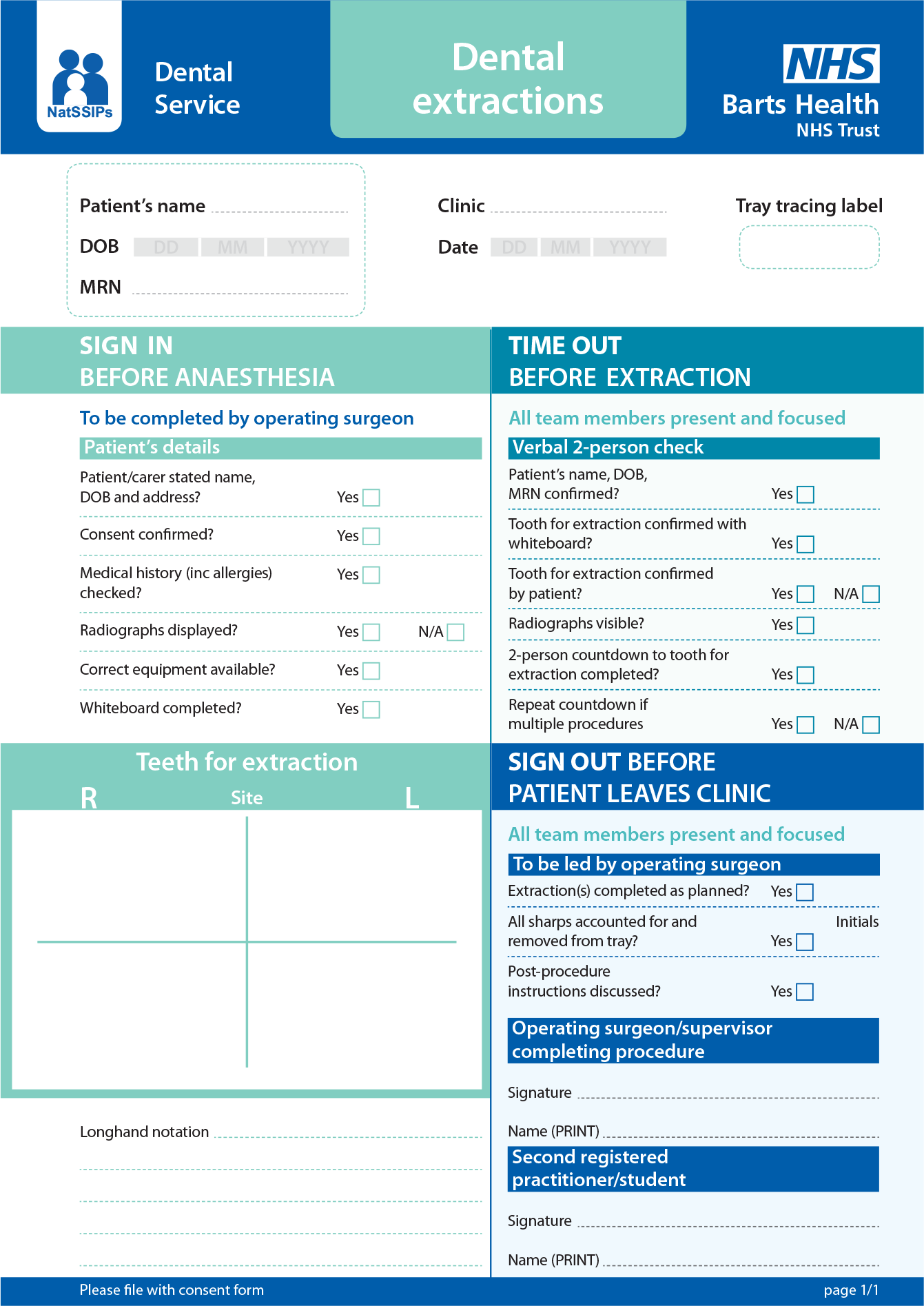
Dental extraction checklist.
In 2015, NHS England launched the National Safety Standards for Invasive Procedures (NatSSIPs), 41 which aim to reduce the number of patient safety incidents in surgery (this includes wrong site tooth extraction). NHS trusts are encouraged to develop local safety standards for invasive procedures (LocSSIPs) based on the national guidance. In dentistry, toolkits are available for adaptation by practitioners,38,42 and the use of these is encouraged. 43
Improvements in patient safety culture have been noted in institutions in the USA. The authors of this survey-based study also found that our medical colleagues appeared to be ahead in terms of patient safety culture. 12
The authors’ experience of creating a climate or culture of patient safety in dental settings is outlined in Figure 2.

Creating a Patient Safety Culture
Teaching and training are significant pillars for developing a patient safety culture. This should start at the undergraduate level44,45 and the intention is that instilling an awareness of patient safety culture will endure throughout a dental professional’s career. 18
Conclusion
Wrong tooth extraction may be one of the most tangible errors that can occur in the dental chair. All would agree that this outcome is to be avoided and that measures must be implemented to reduce the risks of it occurring. However, focusing patient safety research in dentistry on the subject of wrong tooth extraction alone leads to a limited scope of evidence. The profession needs to undertake more research in primary care dental settings, where 95% of dental care actually occurs.
In addition, the profession needs to decide what constitutes a patient safety incident in dentistry. Wrong tooth extraction is a starting point, but there are far more nuanced examples of patient harm that need further investigation.
Much of the discussion relating to patient safety in dentistry has revolved around the use of checklists to prevent wrong site surgery. These are, of course, an important aspect of patient safety and serve as an aide memoir, or a tool for practitioners to use in order to minimise the risks of wrong site surgery. However, as the reader will appreciate, patient safety is far more complex than this and the ultimate aim for all healthcare services should be delivering care in a safe and effective manner whilst understanding human factors.
The authors believe that the responsibility for maintaining, and indeed improving patient safety in dentistry (and ultimately quality), lies with the profession. Dental care professionals should feel empowered to take this issue on, and they should have adequate resources to implement tools for improving patient safety. They should also feel confident enough to speak up when things are not as they should be and to contribute to debates on patient safety.
Sources of information for dentists
British Association of Oral Surgeons – Patient Safety:
World Health Organisation – Patient Safety:
NHS Improvement – examples of LocSSIPs:
Royal College of Surgeons of England – LocSSIPs Toolkit for Dental Extractions: