
Abstract
Examining the nature of stress distribution within the intact tooth can aid in understanding how natural tooth structures are able to resist mechanical forces during masticatory function. Identification of potential fractures in teeth on clinical examination is essential for correct diagnosis, particularly if there is pulpal involvement. This discussion will consider the different types of fracture, their identification and management. This paper will highlight management of tooth fractures, including identifying prognostic indicators, which are largely dependent on the extent of the fracture within the tooth structure.
Learning Objectives
To understand the classification of types of tooth fracture
Recognise the clinical signs and symptoms of each fracture type
To understand the management of different extents of fracture in teeth and effect on prognosis
Introduction
The primary function of teeth in the oral cavity is to serve as mechanical devices for the mastication of food, and to some extent for speech, aesthetics and well-being.
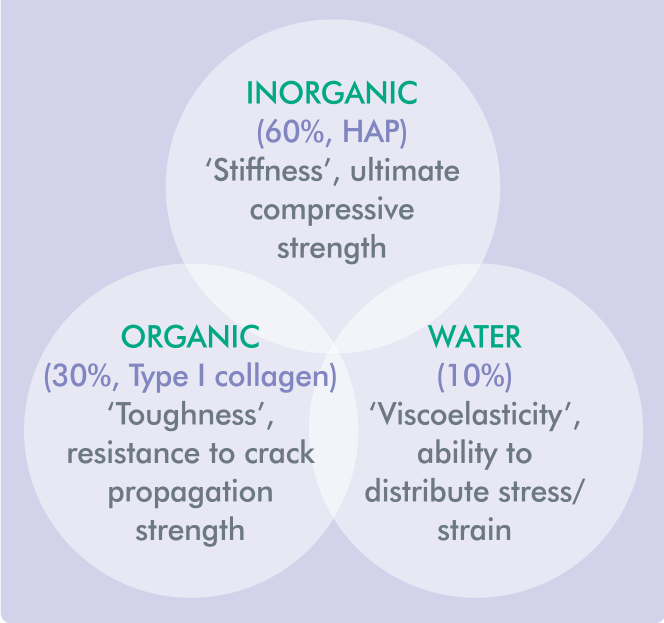
The intact tooth crown comprises the peripheral hard enamel and a sublayer of dentine, the latter consisting of three constituents that affect its physical characteristics during function (Figure 1). 1
– Inorganic (60%, hydroxyapatite) imparting ‘stiffness’ and giving its ultimate compressive strength
– Organic (30%, collagen) imparting ‘toughness’ and its ability to absorb strain and resist crack propagation
– Water (10%) providing ‘viscoelasticity’ and the ability to absorb and distribute stress/strain throughout the entire tooth structure
Constituents of Dentine that have a Role in Affecting Tooth Integrity
The quantity of dentine will determine a tooth’s susceptibility to fracture. The integrity of the interaxial dentine, viz. the ‘core’ of the tooth connecting the axial walls (cusps and marginal ridges) and enclosing the central pulp space, is paramount in this role. 2 The pattern of crack propagation can vary due to the complex anatomy of the occlusal surface and heterogeneous layered structure of a tooth, as both in turn influence the pattern of stress distribution within the tooth.
Patients with a fractured tooth often present with a protracted history of variable symptoms, sometimes poorly localised in a quadrant if the pulp is affected, and with differing pain levels. Signs and symptoms in non-vital and root-filled teeth are markedly different. This discussion will look at tooth fractures in non-endodontically treated teeth.
Prevalence of tooth fracture
The prevalence of cracked teeth is around 80% in patients over 40 years of age. 9 The incidence of incomplete tooth fracture with vital pulps is 9.7%. 23 The average biting loads in humans range from 45.7kg (males) to 36.4kg (females) and the force ratio between molars, premolars, and incisors is 4:2:1 respectively. 10
Abnormal forces on teeth occur in dental trauma, normal occlusal function, or due to parafunctional habits where these loads can be higher. The effects of dental trauma and different levels of tooth fracture are well-documented 4 and is out of the scope of this discussion. We shall instead consider the effect of occlusal forces on the tooth structure that lead to fracture and management.
Mandibular second molar teeth are the most commonly affected teeth followed by mandibular first molars, maxillary premolar; maxillary teeth and mandibular premolar teeth are the least affected. 26
The distolingual cusp of mandibular molars is the most susceptible cusp for fracture. 24 Mandibular molars are more commonly affected than their maxillary counterparts and this may be explained in terms of a combination of their crown anatomy, intercuspal contacts, and their proximity to the fulcrum of jaw rotation (temporomandibular joint), a and so subject to the greater masticatory forces: the ‘nutcracker effect’.8, 26 Although one would expect that maxillary molars should be equally susceptible to fracture due to their distal position, their crown anatomy differs. The oblique and transverse ridges of maxillary molars (which link the distobuccal and mesiobuccal cusps to the mesiolingual cusp) make them more resistant to fracture compared to their mandibular counterparts. They also have a large palatal cusp that often ‘plunges’ inbetween the buccal and lingual cusps of the opposing lower molar to create a wedging effect that separates these cusps. 25
Aetiology
Occlusal forces applied to teeth have an effect on certain parts of a structure, starting from the external surface. This creates a stress plane within the underlying tooth structure in the direction of the force. 3 If the force applied exceeds the strength of dentine (fracture resistance) and its ability to absorb the force, then this will cause the initiation of a crack.1,5 In addition, it has been estimated that restorative procedures can weaken a tooth and predispose the risk of fracture by up to 29 times compared to a healthy intact tooth. 6
Coronal tooth fractures can occur on sudden biting onto a hard object (e.g. olive stone) with the occlusal force focused to a small area of a tooth inducing a ‘masticatory accident. 16 However, over a period of time, the cumulative effect of the number of masticatory cycles in normal and in parafunction 6 can cause chemical and physical bonds along a stress plane in enamel and dentine to break, resulting in tooth fracture. Parafunction plays a significant role in tooth fracture, particularly in an increasingly younger cohort of patients, possibly due to lifestyle and occupational stress-related factors.
There are a host of factors that can contribute to tooth fracture (see Table 1). Broadly, a hierarchy of factors that affect fracture resistance are:
Factors that reduce the fracture resistance of teeth (Adapted from Ellis et al 22 )
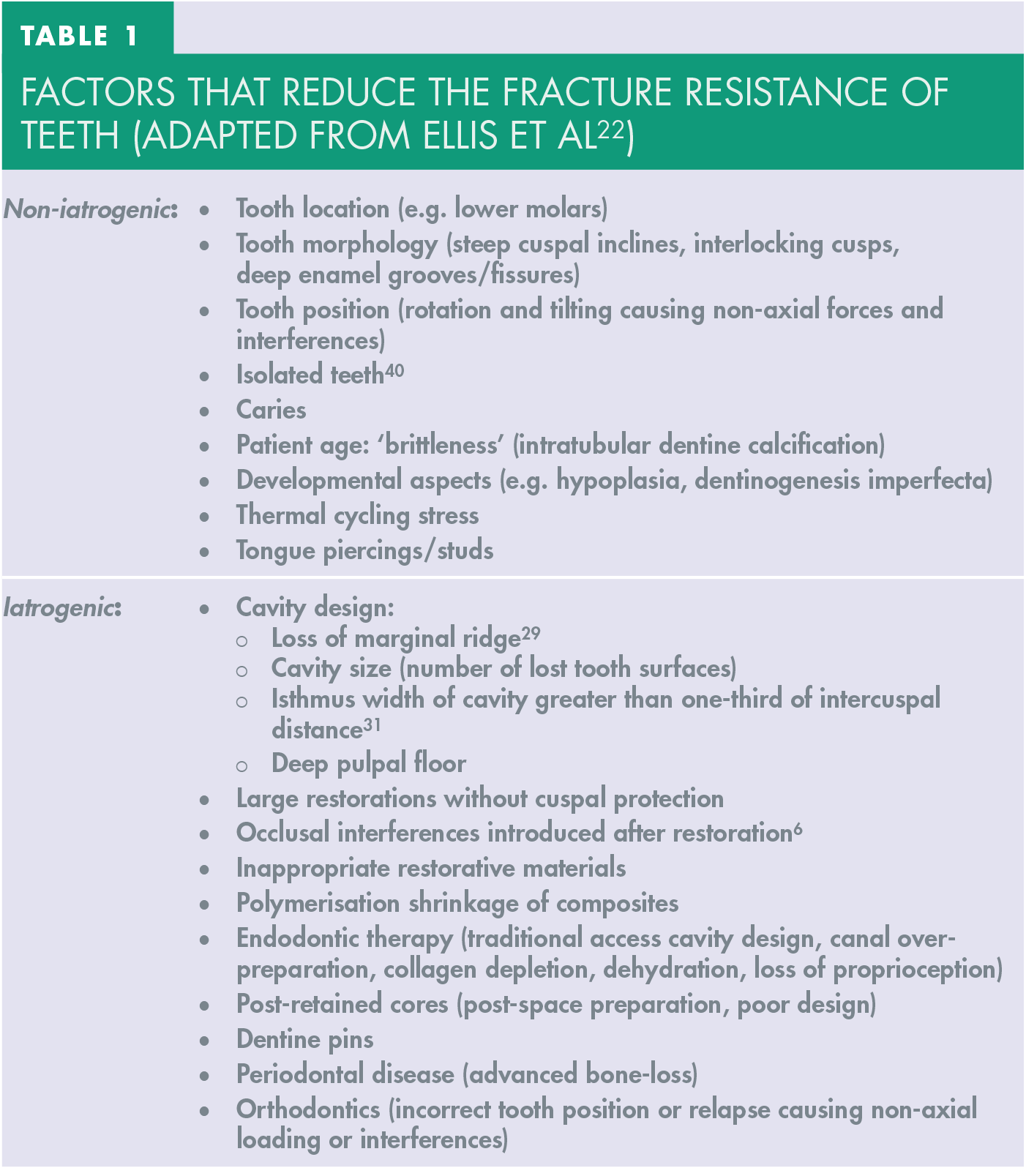
a. Integrity of interaxial dentine
b. Presence of marginal ridges
c. Intact pulp chamber roof
Classification of tooth fractures
Tooth fracture can be either incomplete or complete.3,20,21,28,30
– Incomplete: this is a ‘crack’ that extends from the external surface of the tooth, typically occlusal, through the enamel into dentine, and sometimes extending to the pulp space, causing pulpal disease
– Complete: a fracture that extends from the occlusal surface to another external surface of the tooth or root
Cracks in teeth usually occur in a mesio-distal direction in the crown of a tooth, and then propagate longitudinally into the cervical root level due the direction of the load applied on the tooth surface (i.e. from the occlusal surface). They can then extend and terminate at the cemento-enamel junction, or extend into the root dentine to involve just an individual cusp 7 (a cuspal fracture or ‘cracked cusp’, see Figure 2).

Cuspal fracture (Reprinted with permission from the American Association of Endodontists 31 )
If the fracture extends to the external surface of the root surface below the cervical gingival margin and across the tooth, this ultimately results in a split tooth and the fragments either side of the fracture become separable (Figure 3).
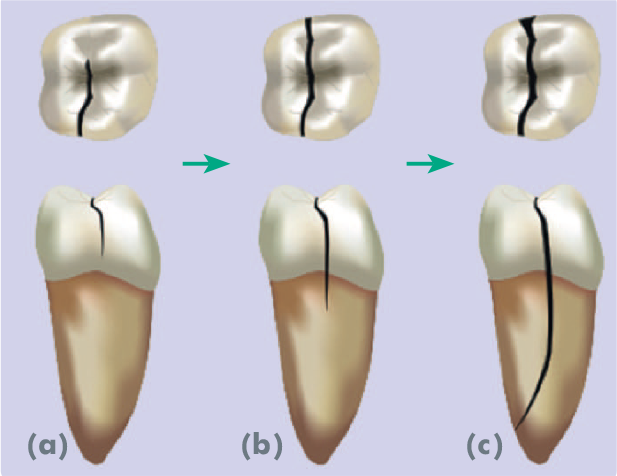
Progression of tooth fracture to split tooth (Reprinted with permission from the American Association of Endodontists 31 )
Vertical root fractures are defined as solely occurring within the root structure, are longitudinal, and extend from the root canal to the periodontium (Figure 4). This fracture type will only be mentioned here.
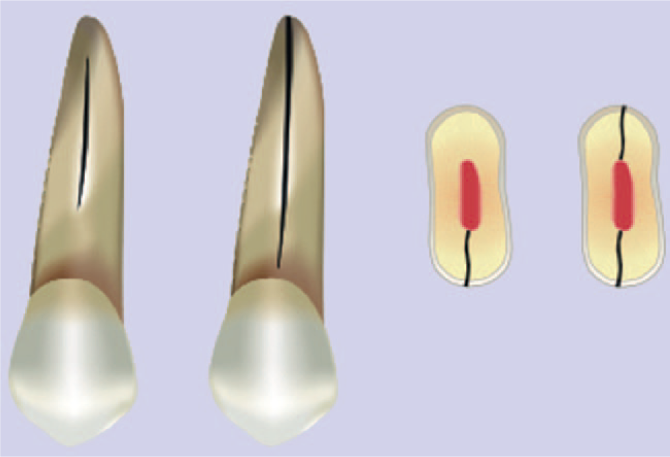
Vertical root fracture (Reprinted with permission from the American Association of Endodontists 31 )
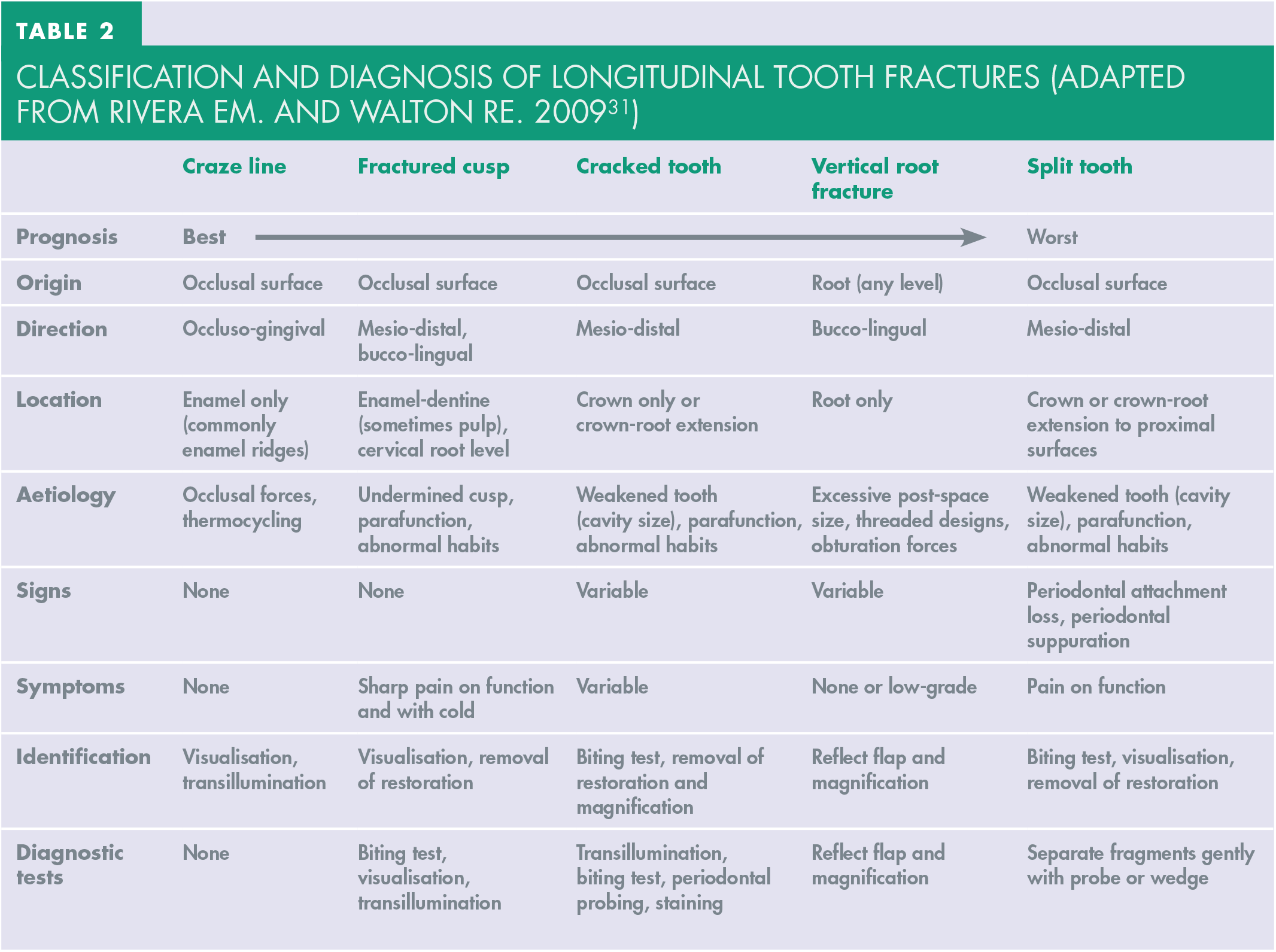
A summary of the classification and investigations for diagnoses for each type of fracture are summarised in Table 2.
Classification and diagnosis of longitudinal tooth fractures (Adapted from Rivera EM. and Walton RE. 2009 31 )
Examination and diagnosis
Visualisation with magnification is critical in identifying fractures, diagnosis, and their management. Use of an operating microscope to 16x magnification can significantly improve a clinician’s ability to diagnose. 7 In addition, transillumination by aiming an LED light source perpendicular to the fracture plane at the cervical level causes diffraction of the light at the fracture interface (Figure 5). Plaque disclosing dyes or methylene blue may be useful but should be used with caution and with magnification in order to distinguish between benign craze lines, anatomical grooves, and deeper structural fractures (Figure 6).
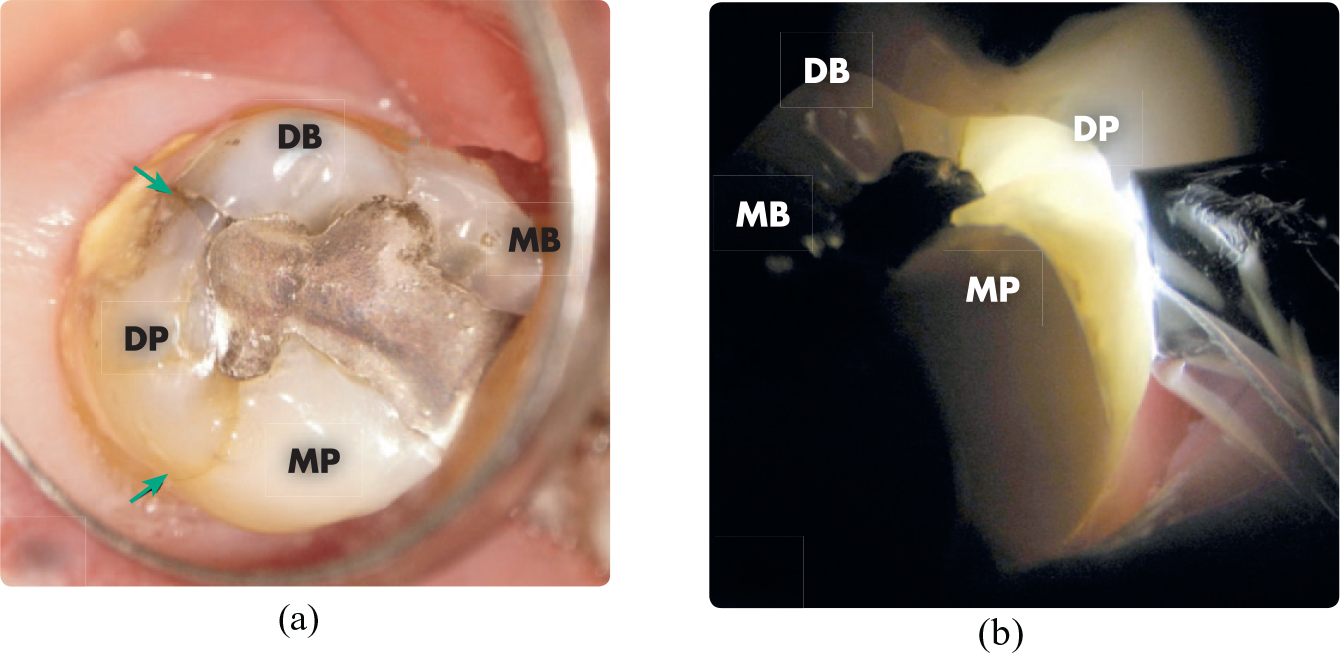
Fractured cusp normal light, and under transillumination
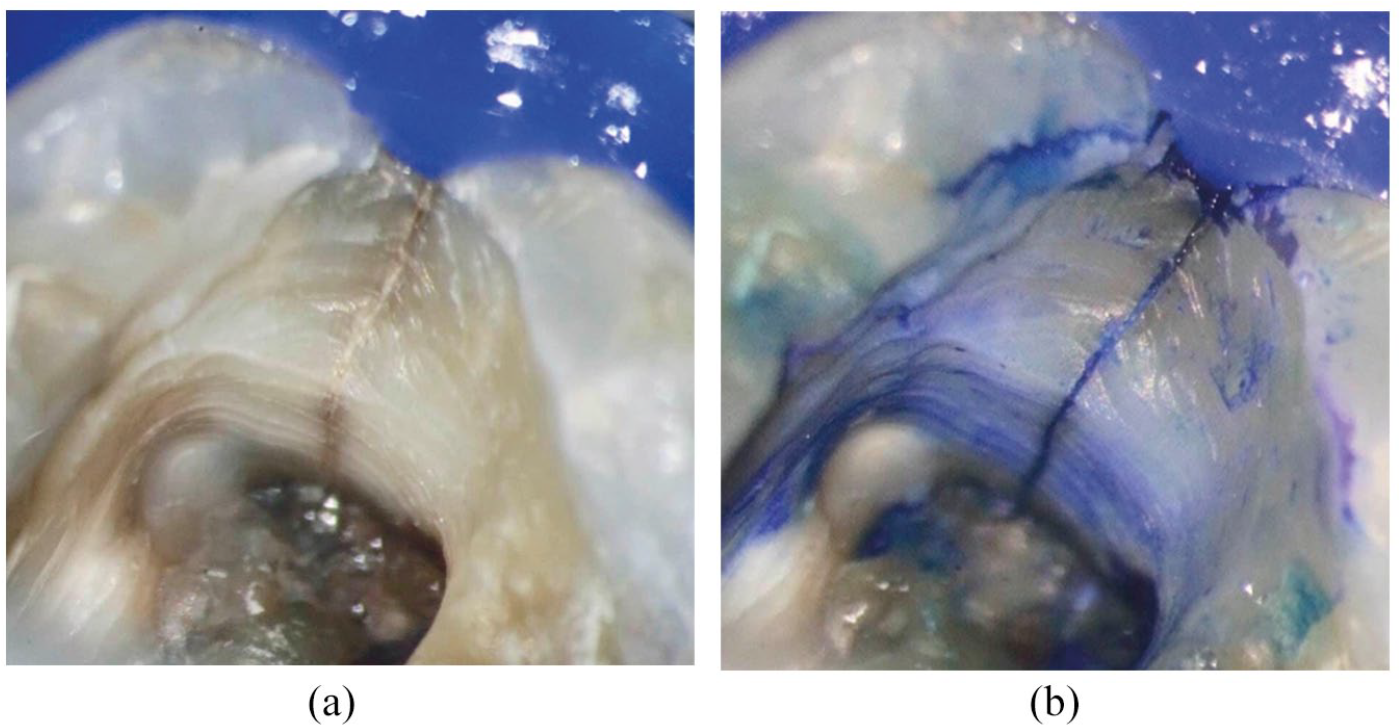
a Cracked tooth b Enhanced visualisation with blue dye (Courtesy of Dr Gustavo Pipita Martinez)
Periodontal assessment is also imperative. An isolated periodontal pocket, in the absence of plaque-related factors, is often pathognomic of a vertical tooth fracture that extends below the gingival margin and onto the external surface of the root and causes marginal periodontal attachment loss along the fracture line.
Radiology and CBCT
Conventional radiography may identify changes that would suggest a tooth fracture (e.g. dystrophic pulpal calcification). However, crack identification is difficult and only noticeable if the radiographic beam coincides with the direction of the fracture plane and there has been some separation.
Cone-beam computed tomography (CBCT) has been advocated as a more accurate alternative to conventional radiography. 17 However, currently, there is insufficient evidence that this is a reliable tool for detecting vertical tooth fractures in root-filled teeth due to the voxel size of the images generated by current devices and radiographic artefacts that are created by radiopaque materials (e.g. root fillings, metal posts).18, 19 It may useful as an adjunctive diagnostic tool in cases where other predisposing factors (e.g. parafunction, crack visualisation, proximal periodontal bone loss) are present 41 and a CBCT scan is taken for endodontic treatment planning.
Management
Craze lines
These are confined to the enamel and are a natural occurrence in teeth and can increase with age due to longevity in function. These are easily visible in anterior teeth but also noticeable in marginal ridges and buccal and lingual enamel of posterior teeth. They do not require treatment other than for aesthetic reasons.
Fractured cusps
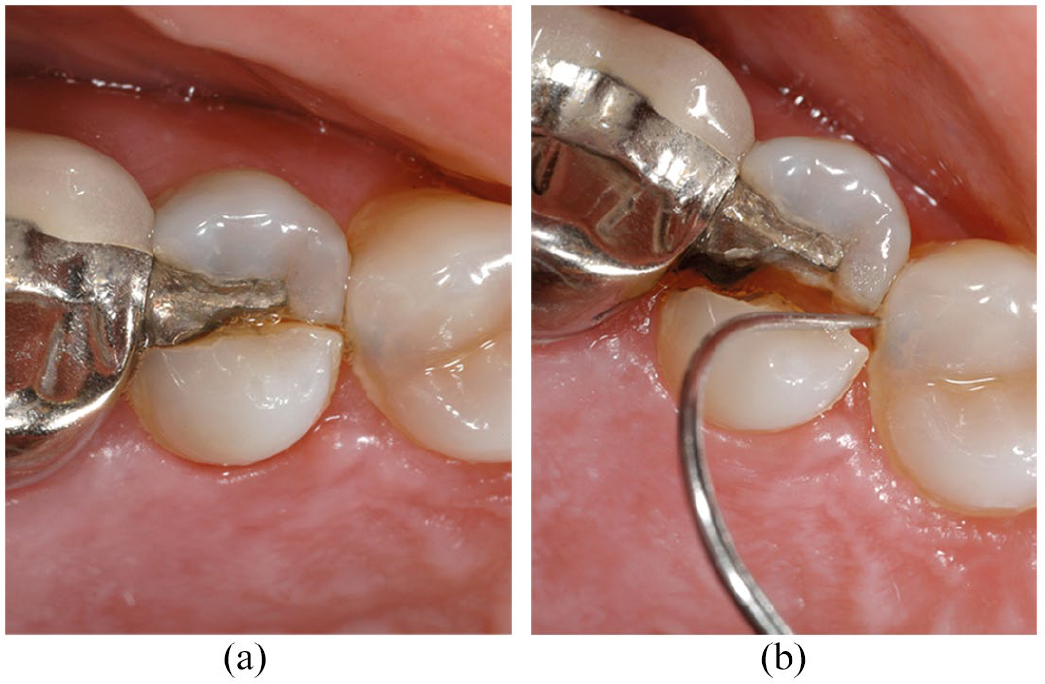
These tend to occur on single cusps (Figures 2 and 5) and include a bucco-lingual component of fracture direction. This can result in an oblique fracture and loss of the entire cusp close to or just below the gingival margin. These may be an incidental finding and be asymptomatic. However, patients will occasionally present with localised cold hypersensitivity and commonly will experience pain during mastication, specifically on release of biting: so-called ‘cracked tooth syndrome’. This is due to the stimulation of sensory nerve fibres within the dentine tubules from the odontoblastic layer and due to ‘hydrodynamic’ movement of fluid within the tubules 32 after flexure and repositioning (‘recoil’) of the cracked cusp. A ‘bite test’ is a useful diagnostic test to localise an affected cusp, 27 using commercially available devices such as the Tooth Slooth II (Figure 7).

Bite tests on individual cusps with a Tooth Slooth II’
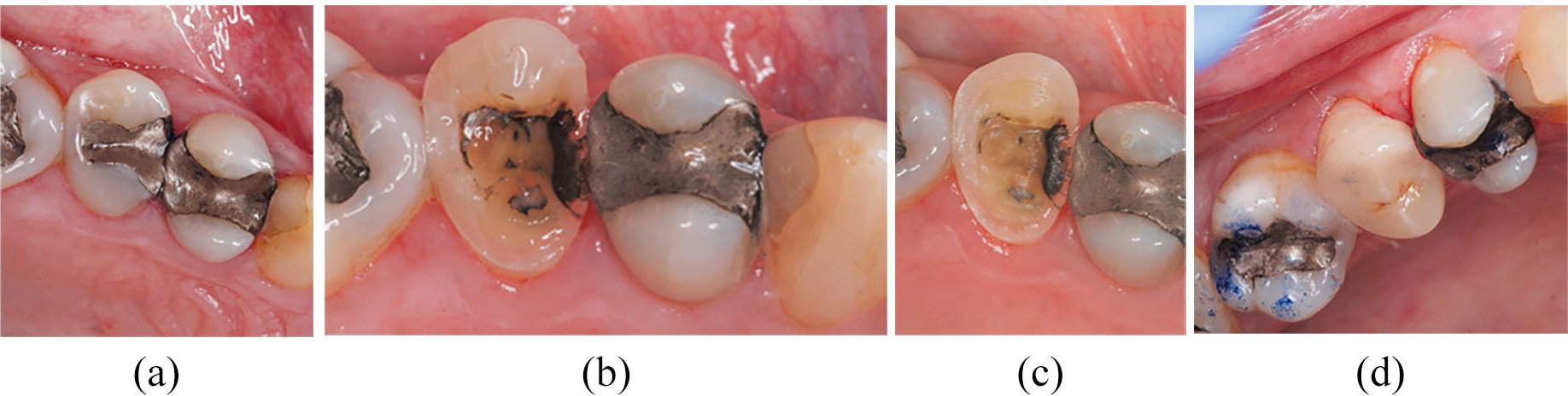
Treatment involves removal of any restoration to identify the location and extent of the fracture. Reduction of the fractured cusp(s) will reduce the patient’s symptoms and reduce the risk of further fracture, with protection of the segment either by direct resin-composite overlay or indirect partial-coverage restoration. 14 If the cusp has detached just subgingivally, then localised ‘margin elevation’ using, for example, an electrosurgery, device, can be used to cut back the gingival margin to the dentine margin to allow isolation, and restoration of the core in readiness for crown preparation (Figure 8).
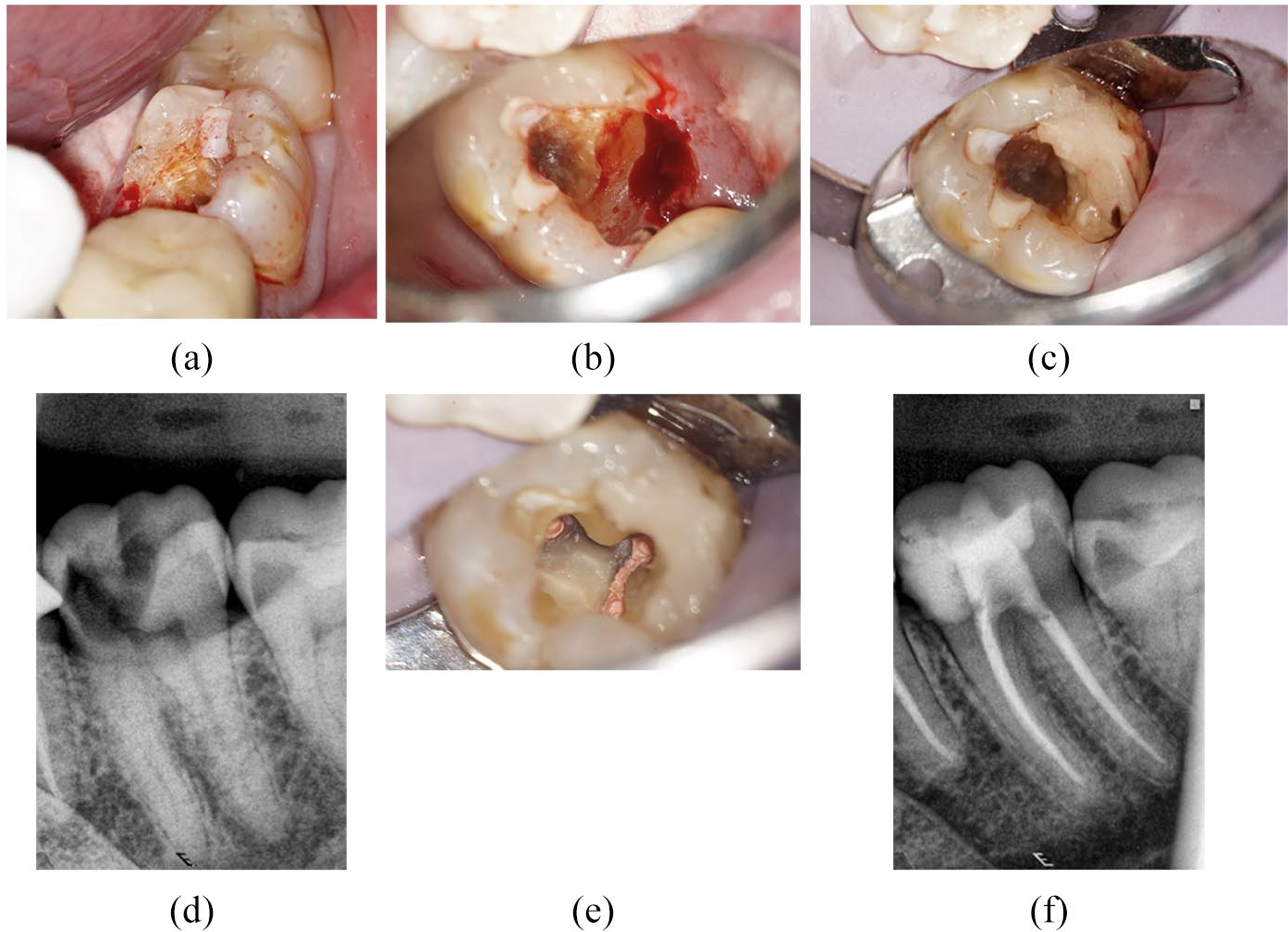
Oblique subgingival fracture and loss of a cusp, provisional core, endodontic treatment
If multiple cusps have fractured, then a decision needs to be made on whether or not there is sufficient ferrule (defined as the height of natural tooth structure extending from the crown margin coronally) to retain a new restoration in the longer term.
If the pulp shows signs of irreversible damage but the cusp is not separated, then endodontic treatment will be required with temporary protection (e.g. stainless steel orthodontic band, temporary crown, or reduction of the cusp from occlusion) until the definitive indirect restoration can be provided. 15 If the cusp shows signs of separation it should be removed and, if the pulp is exposed or there are pulpitic symptoms, endodontic treatment is indicated prior to providing the definitive indirect restoration.
For vital cracked teeth, the overall prognosis of this type of case is very good, although the vitality of the pulp needs to be closely monitored. With time, biofilm will penetrate either directly via the crack or through adjacent dentinal tubules to eventually cause pulp necrosis, 35 and 21 to 29% of such cases will eventually require endodontic treatment.12, 13
Cracked tooth
This presents as an incomplete fracture usually in a mesio-distal direction and extending through one or both marginal ridges (Figure 6a) and through the proximal surfaces and is often central. Crack propagation is variable and time dependant, sometimes due to masticatory accidents, and affected by patient habits (e.g. parafunction) in addition to other factors (see Table 2). Thermal stresses may be a cause and a result of differential expansion/contraction between a restoration and the surrounding tooth structure 33 as well as thermocycling of the restorative material.
Signs and symptoms can be similar to that of cuspal fracture and can range from being slight, of ‘cracked tooth syndrome’, irreversible pulpitis, pulp necrosis, or even eventually an acute or chronic endodontic abscess. Endodontic involvement will depend on longevity, depth of fracture penetration, and leakage or caries around existing restorations.
If the fracture extends to below the gingival margin, a periodontal pocket can develop over time due to biofilm retention within the crack, leading to localised vertical bone-loss. Radiographically, the resorptive pattern extends along the approximal root surface related to the fracture line and can merge with an apical radiolucency: the so-called ‘J-shaped’ lesion. However, this is not always pathognomic of a vertical tooth/root fracture and should only be considered in conjunction with other investigations and special tests. Recently, CBCT has proved to be a valuable non-invasive and diagnostic tool to identify subtle or early changes in bone resorption along a potential root fracture line. 34
If symptoms are absent or low-grade and pulp vitality is within normal limits, restoration with a conservative preparation to maximise the available enamel margin for an indirect resin-bonded ceramic restoration to overlay the occlusal surface (Figure 9) is indicated. If endodontic treatment is required, immediate reduction of functional or load-bearing cusps is essential (Figure 10), direct composite overlay type core or temporary crown, and eventually a definitive indirect full-coverage restoration is essential to, hopefully, prevent the fracture from propagating any further. 40
Conservative overlay preparation of a vital cracked Upper 2nd premolar for a resin-bonded indirect ceramic restoration (Courtesy of Dr Amin Aminian, Specialist in Prosthodontics)
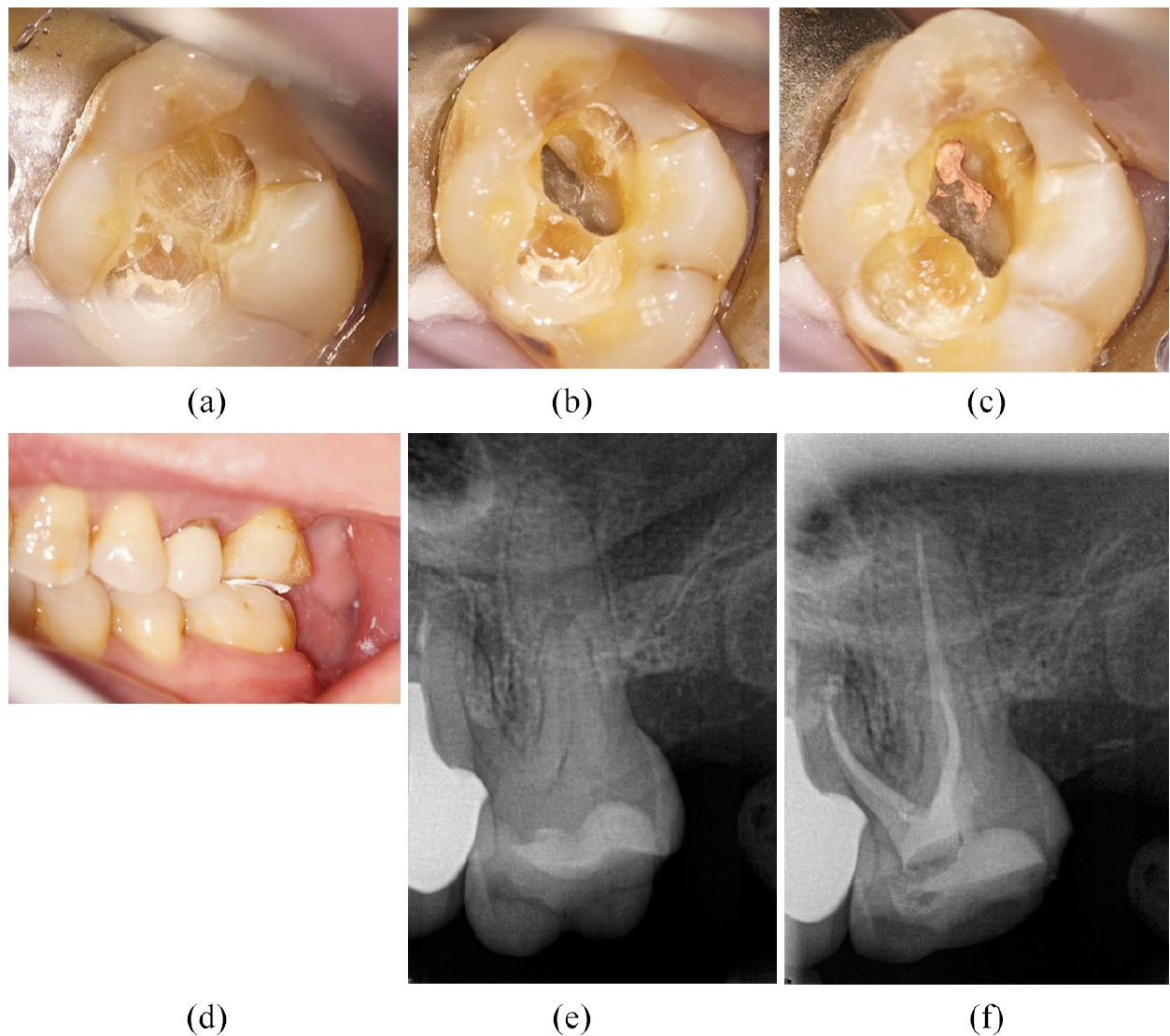
Mesio-distal fracture not extending into pulp chamber floor, requiring endodontic treatment. Tooth adjusted ‘shy’ of dynamic and static occlusion
The prognosis is determined by the extent of the fracture in relation to the cervical (radicular) root level:
– Survival of teeth with cracks just to the cervical dentine is 90 to 92% up to five years36, 37
– Survival of teeth with crack extension into the canal orifice but with no periodontal involvement is 82% up to five years 36
– Survival of teeth over two years with radicular cracks and periodontal pocketing is lower at 74%38, 39
Therefore, on investigation, fracture lines must be visualised and tracked to their full extent under magnification. If they extend into the pulp chamber floor or for more than 5-7mm below the canal orifice level onto the pulp chamber floor, then the prognosis is very poor.
Split tooth
This fracture is defined as a complete fracture initiated from the crown and extending subgingivally, usually in a mesio-distal direction through proximal marginal ridges. It is essentially the terminal stage of tooth fracture (Figure 11).
Split tooth
The presentation is usually with mobility of one or both fragments, periodontal loss of attachment at the fracture site, possibly developing suppuration as a periodontal abscess.
The prognosis for these is hopeless and the fragments need to be removed to limit bone loss, particularly if a dental implant is to be considered.
Conclusion
A summary of restorative and endodontic treatment strategies for fractured teeth is shown in Figure 12. For fractured teeth that require endodontic treatment, modifying factors are advisable in order to reduce the risk of catastrophic fracture immediately after the endodontic treatment and before placement of the indirect restoration. 37
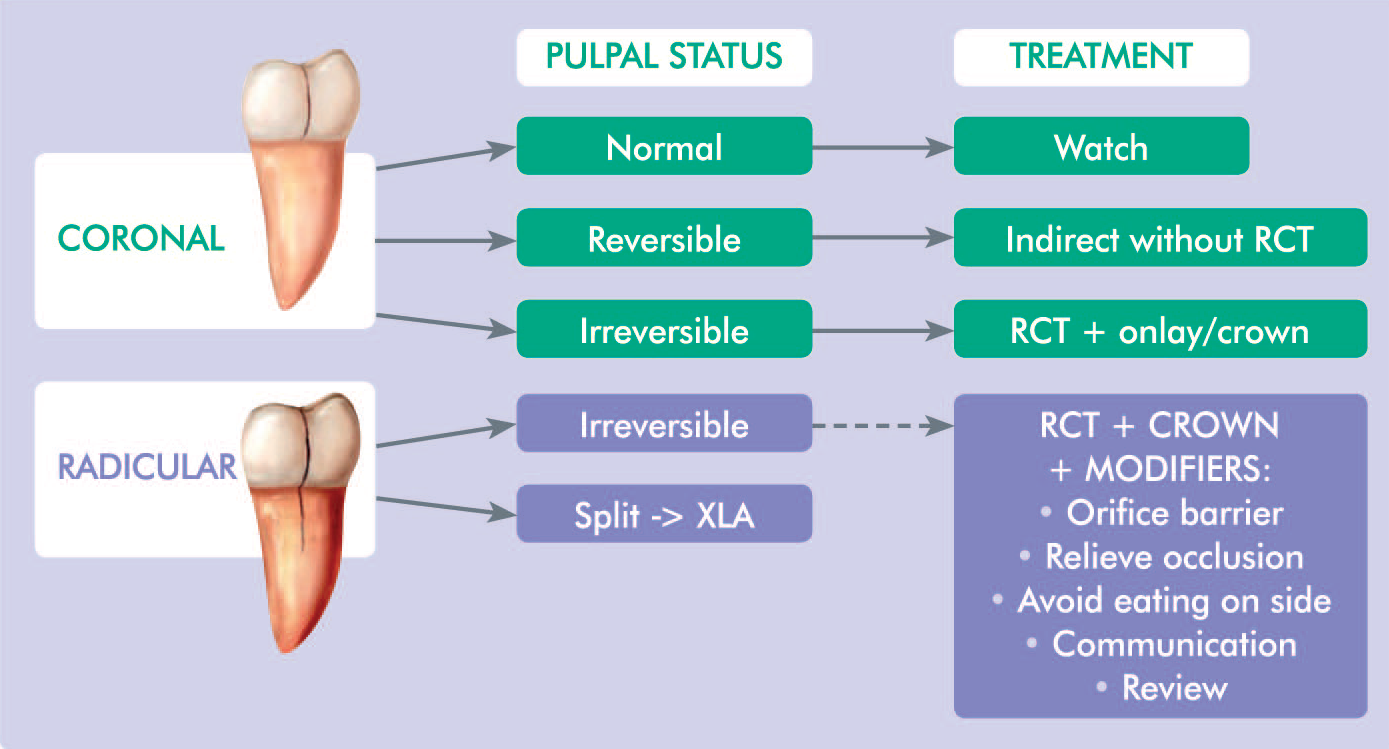
Treatment Strategies for Tooth Fractures
It is essential in operative dentistry that the clinician understands biomechanical effects of occlusal forces on a tooth in order to mitigate and manage the event of a fracture of a tooth. This encompasses the knowledge of the relationship between occlusal anatomy, intercuspal contacts (dynamic and static) in designing and providing new restorations. Involvement of the pulp and the quality of ferrule require further consideration when deciding the viability of a fractured tooth. Ultimately, this will maximise the longevity of restorations and the survival of teeth.