
Abstract
Aims:
This systematic review aims to identify and synthesise available evidence to determine the clinical and radiographic outcomes of REP involving any disinfection irrigant together with a non-antibiotic intracanal medicament.
Methods:
Experimental and observational studies evaluating the outcomes of REP in immature non-vital permanent teeth in 6-16 year olds, where the protocol used any type of disinfectant irrigant together with a non-antibiotic intracanal medicament (non-setting calcium hydroxide) were included. Data was narratively synthesised and presented in respect to the primary outcome (elimination of symptoms and infection) and secondary outcomes (increase in root length/width; positive response to vitality testing; patient-reported outcomes; adverse effects).
Main findings:
1628 studies were identified, of which five met the eligibility criteria for inclusion in the review. Studies included one randomised control trial and four observational studies. All five studies showed an absence of clinical signs and symptoms for all teeth postoperatively with radiographic resolution or absence of pathology following the disinfection stages of the REP used. Choice of secondary outcomes were inconsistent but included further root development, coronal discolouration and root canal calcifications postoperatively. There was a high risk of bias in all five studies and subsequently the quality of the evidence base was judged to be low.
Principle conclusions:
REP using a non-antibiotic disinfectant approach appears capable of providing satisfactory outcomes for a non-vital immature permanent tooth. Further high-quality research is required before solid recommendations towards clinical practice guidelines for the disinfection portion of REP can be implemented.
Keywords
Learning Objectives
To determine the outcomes of Regenerative Endodontic Procedures (REP) involving any disinfection irrigant together with a non-antibiotic intracanal medicament in immature permanent teeth
To understand the fundamentals of REP
To understand the evidence base concerning the outcomes of REP with a non-antibiotic protocol through a systematic review
Introduction
Regenerative Endodontics
During tooth development, an erupting or erupted tooth may experience trauma, typically from an acute traumatic force or a chronic disease process, such as caries, which is sufficient to cause devitalisation of the pulp. As a sequalae of the pulp becoming non-vital, any further root development ceases, resulting in incomplete root formation. The tooth is then considered immature and pulpal necrosis develops leading to periapical pathology. Clinical signs can include pain, tenderness to percussion (TTP), mobility, swelling and a sinus.
For an adolescent presenting with a non-vital immature tooth, the ideal management would prevent pain and infection, and retain the tooth for function and optimum dental development. This is particularly important for the psycho-social wellbeing of the patient if the traumatised tooth in question is in the anterior region. 1 The options for treatment of a non-vital immature tooth with periapical pathology 2 have historically included:
No treatment – all patients have the option of no treatment, but the risks associated with this option include persistent pain and infection, and a greater chance of the tooth being lost in the future
Apexification – the creation of an apical barrier, of the open apex, at the root end after complete disinfection of the root canal. Restorative materials to form the barrier include non-setting calcium hydroxide (Ca(OH)2) or mineral trioxide aggregate (MTA) (Figure 1)
Extraction – the tooth is removed, which treats pain and infection but may lead to functional and aesthetic concerns
Extraction and transplantation – a vital donor tooth, commonly a premolar tooth, is atraumatically extracted and immediately implanted into the site of the extracted non-vital immature tooth
It is now accepted that there is another option of treatment, termed regenerative endodontics (Figure 1), centred around the principles of tissue engineering. 3
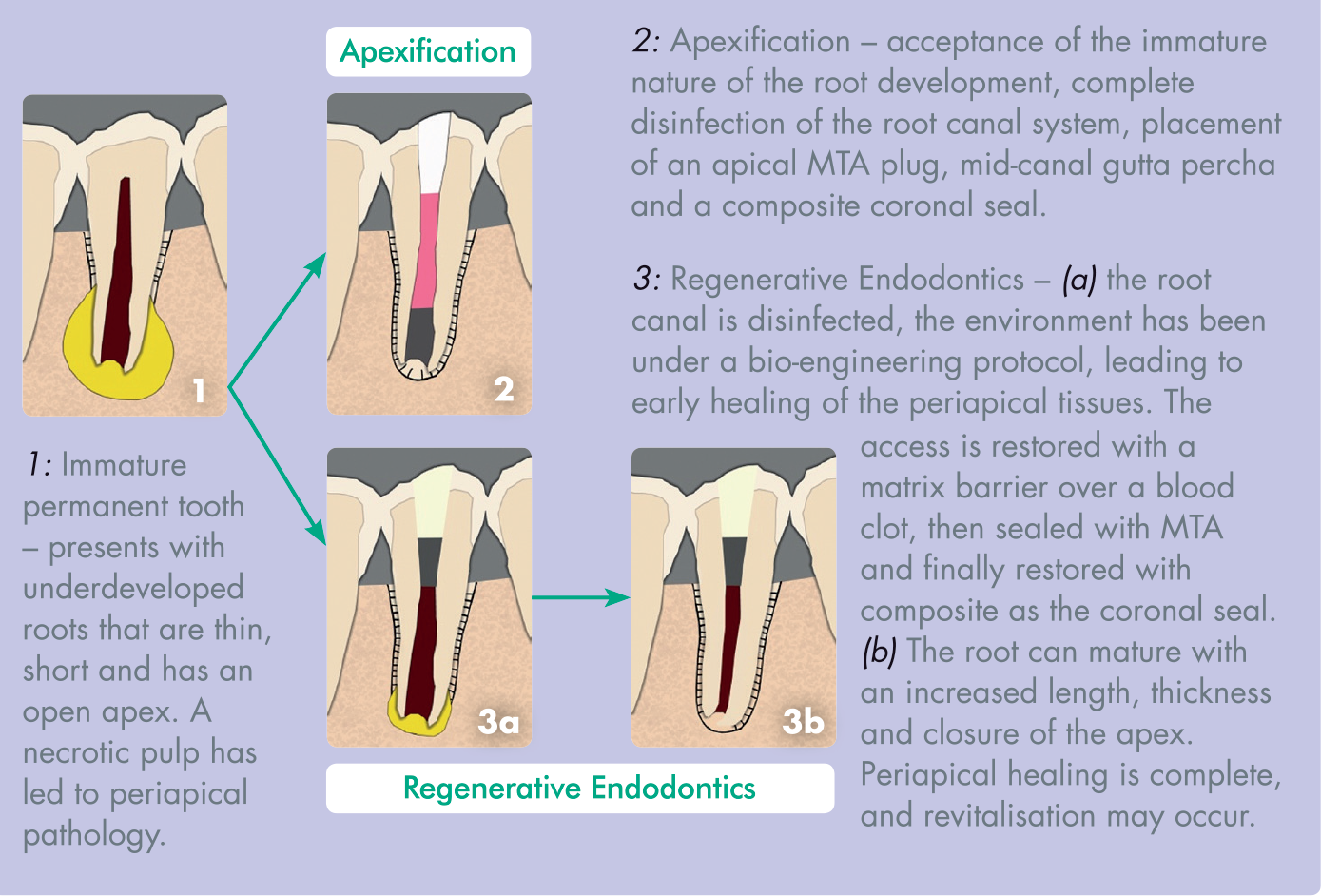
Diagrammatic representation of apexification vs. regenerative endodontics:
The recommended protocol by the European Society of Endodontology consists of the provision of the procedure over two appointments and is briefly outlined: 4
Phase 1 Access to the non-vital pulp under local anaesthesia and aseptic techniques Minimal mechanical disturbance of any pulp tissue in the canal Disinfection by irrigants Disinfection by intracanal medicaments (triple antibiotic paste or calcium hydroxide) Provide a coronal seal
Phase 2 – (2-4 weeks after phase 1) Assess success of phase 1, i.e. asymptomatic and lack of signs of infection (swelling and sinus) – if unsuccessful then phase 1 is repeated with replenished intracanal medicaments
Confirmation of success of phase 1: Access to the pulp under local anaesthesia (without any vasoconstrictor component to allow bleeding induction) and aseptic techniques Irrigate with 17% EDTA solution (chelating agent) Induce bleeding, via instrumentation, through the apex to fill the root canal with blood Place a collagen matrix above the formed blood clot Seal with MTA followed by the placement of a resin composite
Phase 1 aims to create a disinfected environment within the root canal and allows an environment for initial periapical healing to occur. Phase 2 aims to recruit stem cells of the apical papillae (SCAP) directly next to the root tip within the periodontal ligament and bone from below the root apex to regenerate the dentine-pulp complex within the root canal.
Regenerative endodontics is not a completely new concept within dentistry. Experimental studies were conducted in 1961 by Nygaard-Ostby and clinically applied, based on later developed experiments, by Iwaya 5 and Branchs and Trope 6 . It is, however, continued to be practiced with little clinically proven evidence base or strict guidelines, with a wide range of REP techniques shown in the literature. 7
The theoretical potential for this area of dentistry is great and this type of tissue bioengineering could provide great benefits to the management of patients.
Increasing evidence of the healing potential of the pulp 8 suggests it is possible to induce biological replacement of cells of the dentine-pulp complex, regenerate the pulp tissues, promote continued development of the root structure and even revitalise the tooth. 3 The preservation of the tooth tissues results in maintenance of the tooth together with its sensory and protective functions.9,10
Regenerative endodontics provides a challenge not found within traditional non-surgical endodontics. The open root apex provides no barrier for control of instrumentation and disinfection, but this also facilitates the stimulation of stem cells, scaffolds and growth factors to provide the desired outcomes of REP. 11
Ideally, the outcome of regenerative endodontics is maintenance of a functional tooth with completed root development, achieved through complete regeneration of all original tissues within the root canal system. Many interchangeable terms are used to describe the same endodontic process, including ‘reparation’, ‘revitilisation’ and ‘revascularisation’ as these describe different elements of outcome provision. Current histological evidence suggests the procedure can only achieve a ‘reparative’ outcome, as natural human tissues cannot regenerate once completely damaged.11,12
Disinfection within REP
The current recommendation for regenerative endodontic procedures (REP) advocates sufficient disinfection of the pulp space,4,13 provided through disinfection irrigants (solutions) and intracanal medicaments, which may be either non-setting calcium hydroxide or an antibiotic paste (double or triple antibiotic formula). 4 This protocol has resulted in favourable outcome rates that are comparable to apexification procedures, with the added potential benefit of the continued growth of the root structures and a return to positive vitality testing. 13
In the absence of infective micro-organisms within the damaged pulp, healing of pulp and periapical tissues can occur, as documented in the literature. 14 The disinfection process in REP provides an environment where the bio-engineering factors in the procedure can thrive: ‘the concentration of both irrigants and medicaments are important to find the balance between disinfection of the canal, attraction of dentine matrix for release of growth factors and survival and proliferation of SCAP’. 15
The disinfection process in REP starts with the use of irrigants, primarily sodium hypochlorite but it can also include saline, hydrogen peroxide or chlorhexidine. Sodium hypochlorite solution has excellent potency and antibacterial properties (bactericidal) with an effective concentration shown to be ideally 5.25% for non-surgical root canal treatments.16,17 Disinfection continues with the use of an intracanal medicament placed in the root canal and sealed with a restorative material to permit its function for a period of time. Calcium hydroxide is one intracanal medicament used as a non-setting paste, which is antibacterial 18 and has the ability to further significantly reduce bacteria within root canals after a disinfection irrigant has been used previously. 19 Triple antibiotic paste (TAP) is another intracanal medicament that has been used historically in REPs and continues to be used due to its antibacterial properties. 20
Justification for this review
Worldwide concern about over-prescription of antibiotics and the associated risk of antibiotic resistance has led to guidelines from the National Institute of Health and Care Excellence to reduce the use of antibiotics within the UK.21,22 These recommendations apply across healthcare, including dentistry, and have implications for antibiotic use in regenerative endodontics. The European Society of Endodontology (ESE) published a position statement in 2018 on the use of topical antibiotics in endodontics stating: ‘Taking into account the lack of solid evidence supporting the use of antibiotics in REP, the use of calcium hydroxide should be preferred over tri-antibiotic paste’. 23 This emphasises dental professionals’ responsibility to provide REP that use non-setting calcium hydroxide as the intracanal medicament instead of antibiotic pastes to create a disinfected environment, after disinfectant irrigants, for the pulp space.
A scoping search was conducted on Google Scholar and two key endodontic journals, the International Endodontic Journal and the Journal of Endodontics. This highlighted two recent systematic reviews that had collated all studies examining REPs using different disinfection irrigants with either non-setting calcium hydroxide or antibiotic pastes as an intracanal medicament.24,25 This means that intervention-specific outcome rates for REP protocol involving different disinfection irrigants, together with or without an antibiotic intracanal medicament, have not been identified and had the potential to be reviewed.
By identifying and synthesising relevant studies, this systematic review aims to distinguish intervention-specific outcomes for regenerative endodontic protocols containing specific disinfection factors. This important evidence synthesis is required to support evidence-based clinical guidelines for regenerative endodontic protocols. In addition, the review will identify future research priorities.
Research question
This research intended to examine the effect of non-setting calcium hydroxide medicament together with disinfection adjuvants on regenerative endodontic clinical and radiographic outcomes in immature permanent non-vital teeth of adolescents aged 6-16 years old.
Aims
To determine the clinical and radiographic outcomes of Regenerative Endodontic Procedures (REP) involving any disinfection irrigant together with a non-antibiotic intracanal medicament in immature permanent teeth.
Objectives
To identify empirical studies examining outcomes for REP involving any disinfection irrigant together with a non-antibiotic intracanal medicament
To synthesise and quality assess the studies
To identify the clinical implications of a non-antibiotic medicament regenerative endodontics protocol on future clinical practice and current guidelines
Methods
Prior to developing the review methods, PROPSERO was searched to identify any existing reviews in this area. PROSPERO is an international database of prospectively registered systematic reviews in health care. 26 No existing or planned reviews were identified.
Design
A systematic review approach was selected as the most appropriate method to identify and summarise the best available evidence on the chosen topic. Explicit, systematic and reproducible methods with a clear objective are used to minimise bias. 27
Ethics
An ethics checklist was submitted to the University of Central Lancashire (UCLan) prior to commencing the review. The ethics committee provided confirmation that no ethical approval was required.
Inclusion and exclusion criteria for study selection using the PICO model
Exclusions: Animal studies.
Exclusions: Studies using any form of antibiotic pastes as an intracanal medicament.
Exclusions: No exclusions.
Primary: Elimination of clinical symptoms (pain, sinuses and swelling)
Reduction in radiographic evidence of the presence of pathology
Secondary: Increase in root length and width
Positive response to vitality testing by either a thermal (cold) test or an electric pulp test (EPT)
Patient reported outcomes
Adverse effects
Owing to the limited evidence-base in the scoping searches, a wide range of study designs were included: experimental studies (randomised controlled trials; non-randomised controlled trials) and observational studies including prospective and retrospective studies with or without a control group with at least >5 participants. Case reports or case series with 5 or fewer cases, and non-empirical evidence (review articles, letters, expert opinion) were excluded. No exclusions were made based on setting or language.
Search strategy
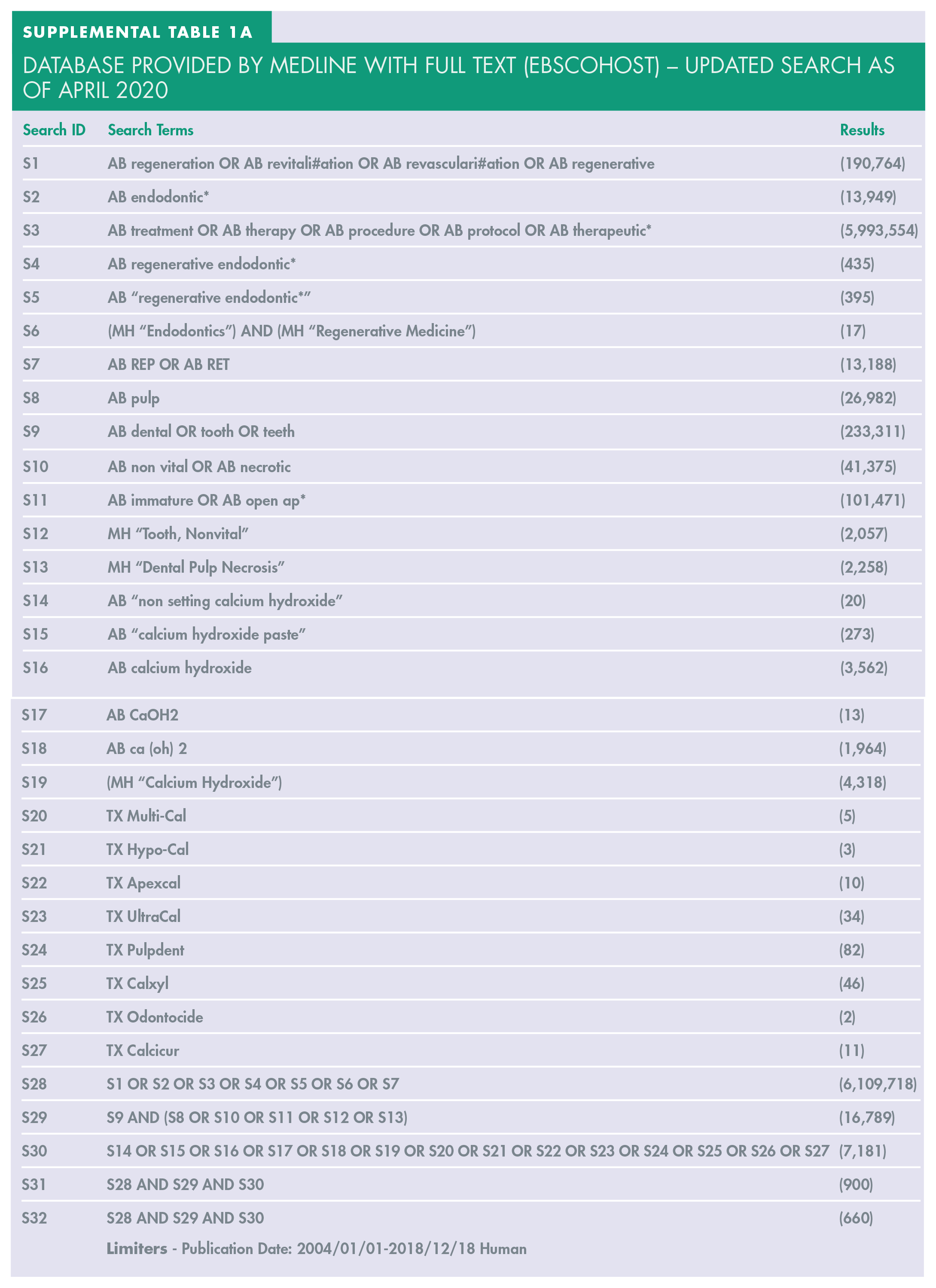
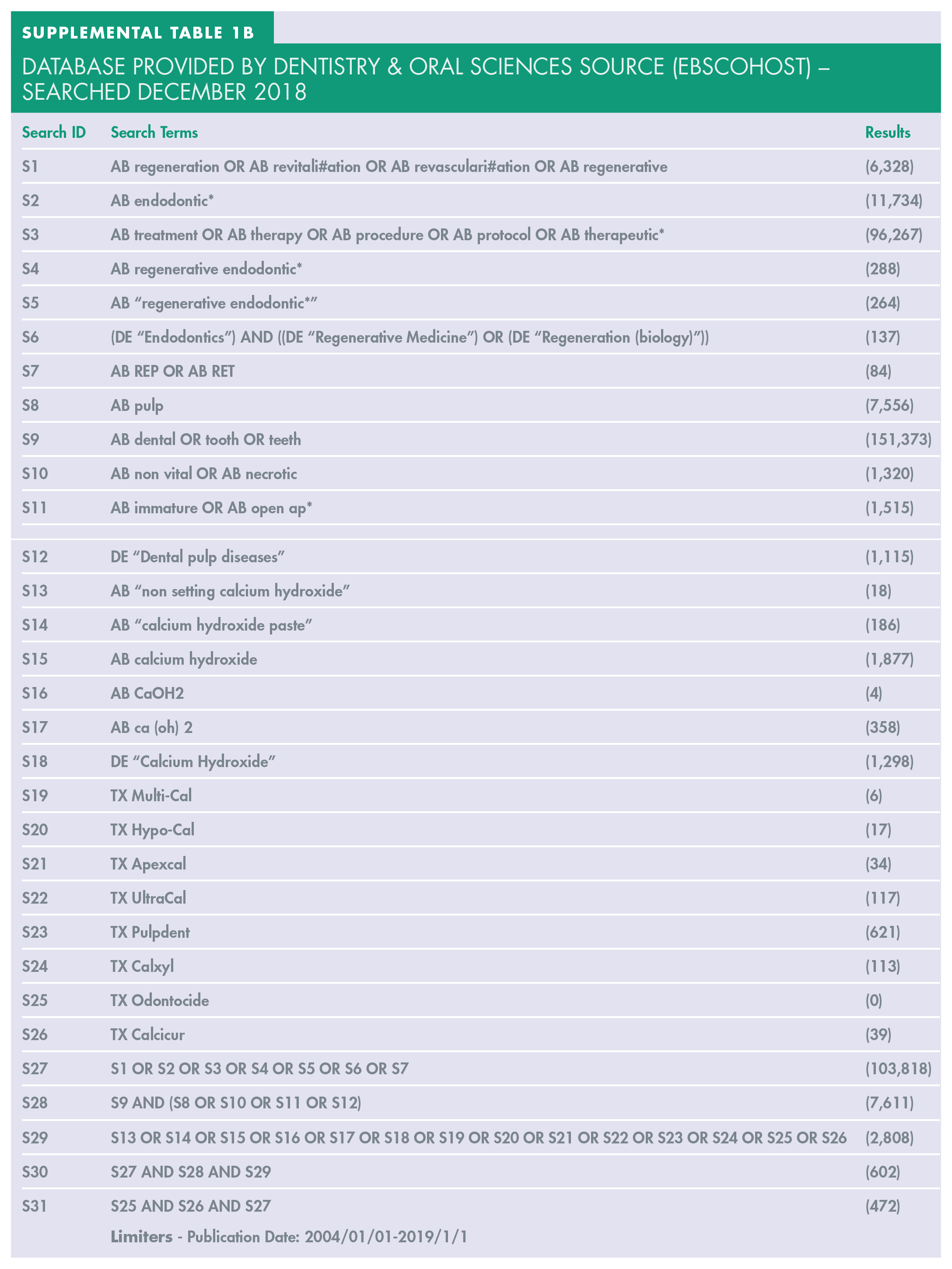
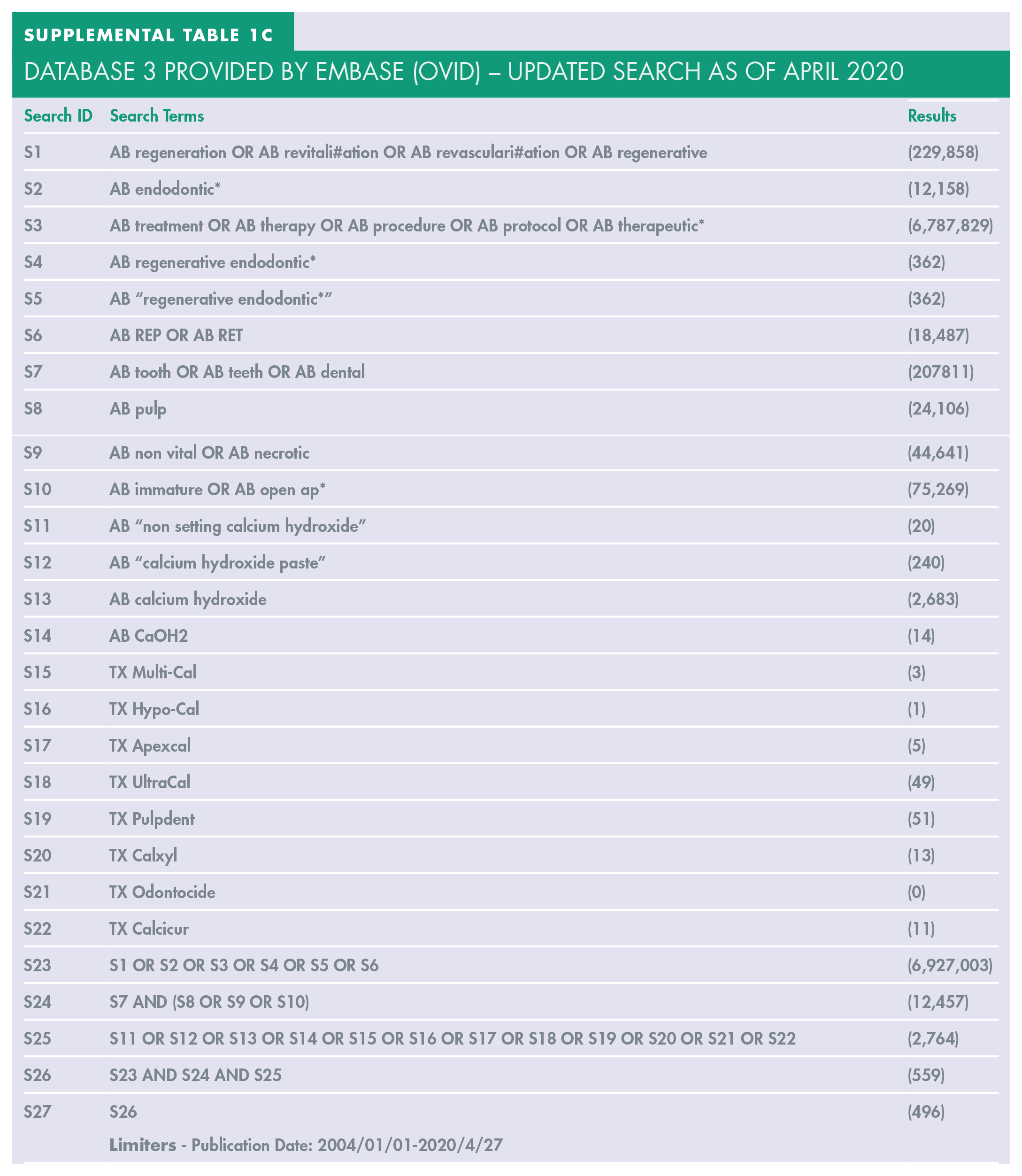
Three popular academic databases for health care research were chosen for the searches to allow a comprehensive search of the available literature (MEDLine with full text, Dentistry and Oral Sciences sources, Embase). In addition, handsearching was performed via Google Scholar and reviewing reference lists of included studies.
Five key search terms, derived from the research question, were used as concepts forming the basis of the search strategy:
Regenerative endodontics
Immature permanent tooth
Calcium hydroxide
Disinfection
Outcomes
No limitations were made on language of any studies. The searches were restricted to 1st January 2004 to the day of the search (18th December 2018). Prior to 2004, greater variation was present within REPs but a key study by Branchs et al. in 20046 established a more standardised approach to REP, which subsequent studies largely followed. The search was performed on 18th December 2018 and updated on 24th April 2020.
Study selection
Study identification and selection was performed by a single reviewer (AK). The records were imported into a reference management program, RefWorks (RefWorks, ProQuest LLC). A screening process of the search results included removal of duplicate studies, using the predefined inclusion and exclusion criteria by title, abstract and finally full text.
Data extraction
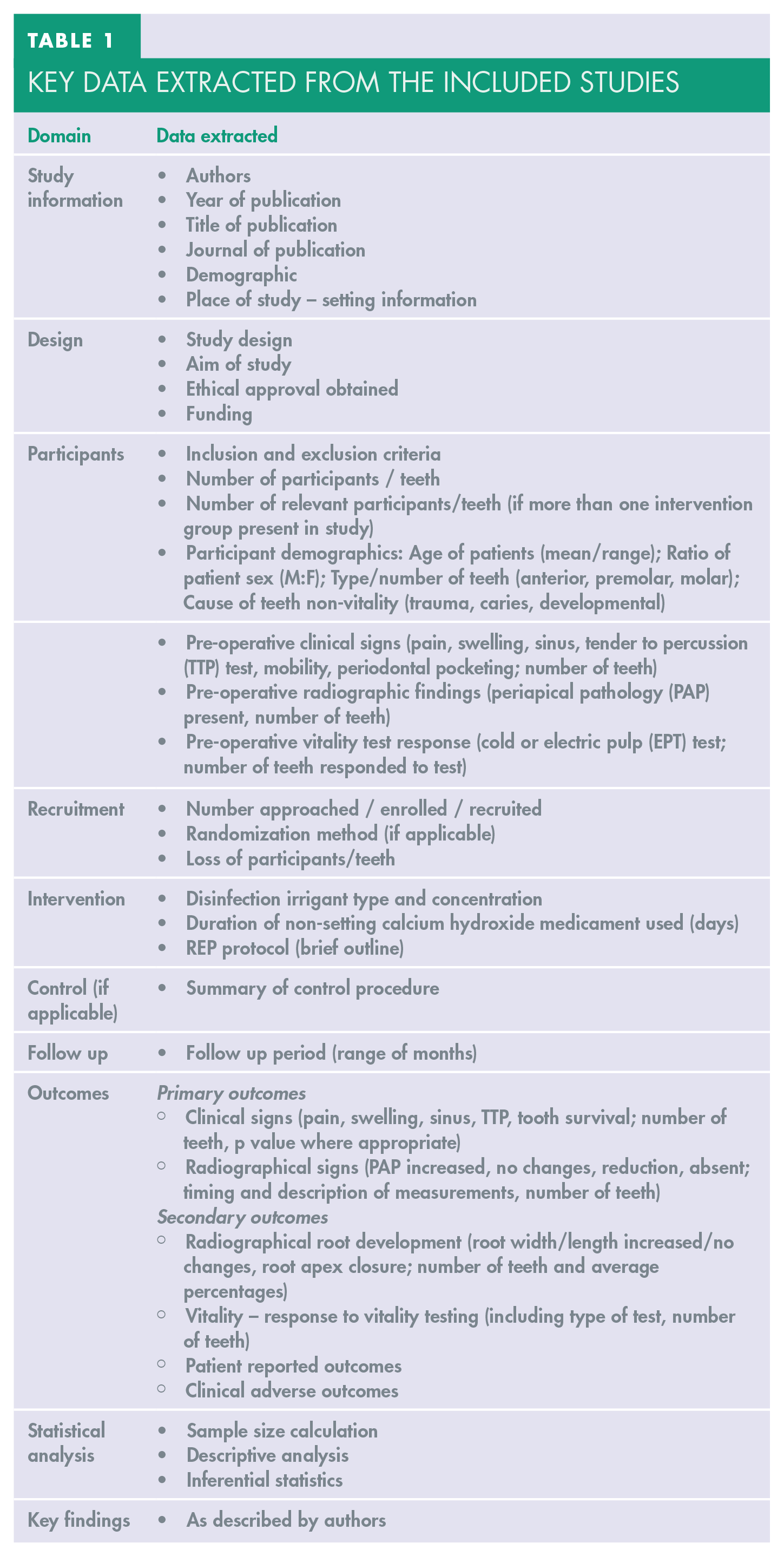
Data extraction was performed by a single reviewer (AK). Key data was extracted and presented to allow synthesis across and within studies in a table in Microsoft Word v16.17 (Microsoft Corporation). The key information extracted from the records is presented (Table 1). Any missing data was managed by contacting the corresponding author.
Key data extracted from the included studies
Data synthesis
Meta-analysis was planned for studies with adequate homogeneity in population, intervention and outcome measures. Where heterogeneity between studies precluded quantitative synthesis, a narrative synthesis was performed.
Quality assessment
The tools used to assess the risk of bias are the Cochrane Risk of Bias Tool 28 for any randomised control trials and the Quality Assessment Tool for Quantitative Studies by the Effective Public Health Practice Project 29 for any observational studies.
Results
Study selection
Searches of the three databases alongside handsearching provided a total of 1628 studies. The PRISMA flow chart showing study selection is given in Figure 2. Following de-duplication and exclusion by title and abstract, 17 studies were obtained for full text screening. Twelve studies we excluded with reasoning listed in Supplemental material 2. Five studies were included in the review.30,31,32,33,34
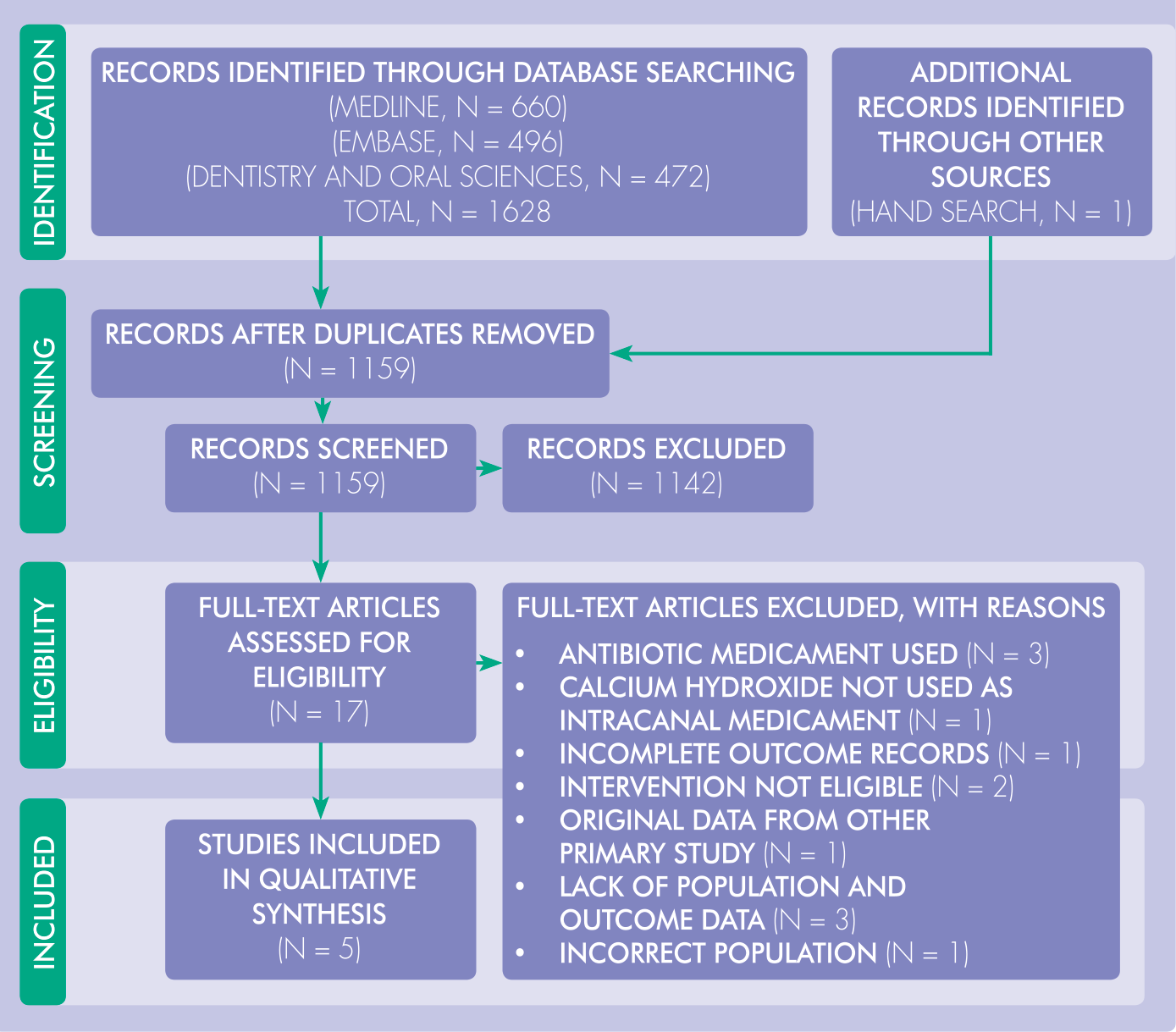
PRISMA flow diagram describing the study selection process
Study characteristics
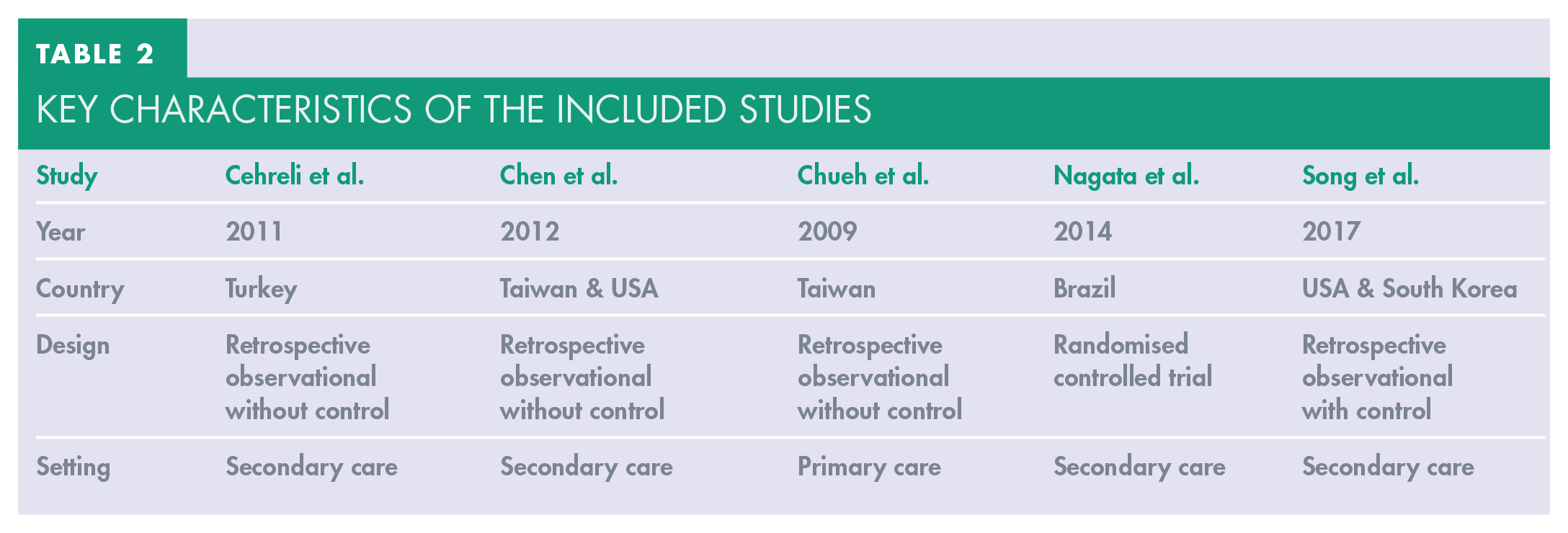
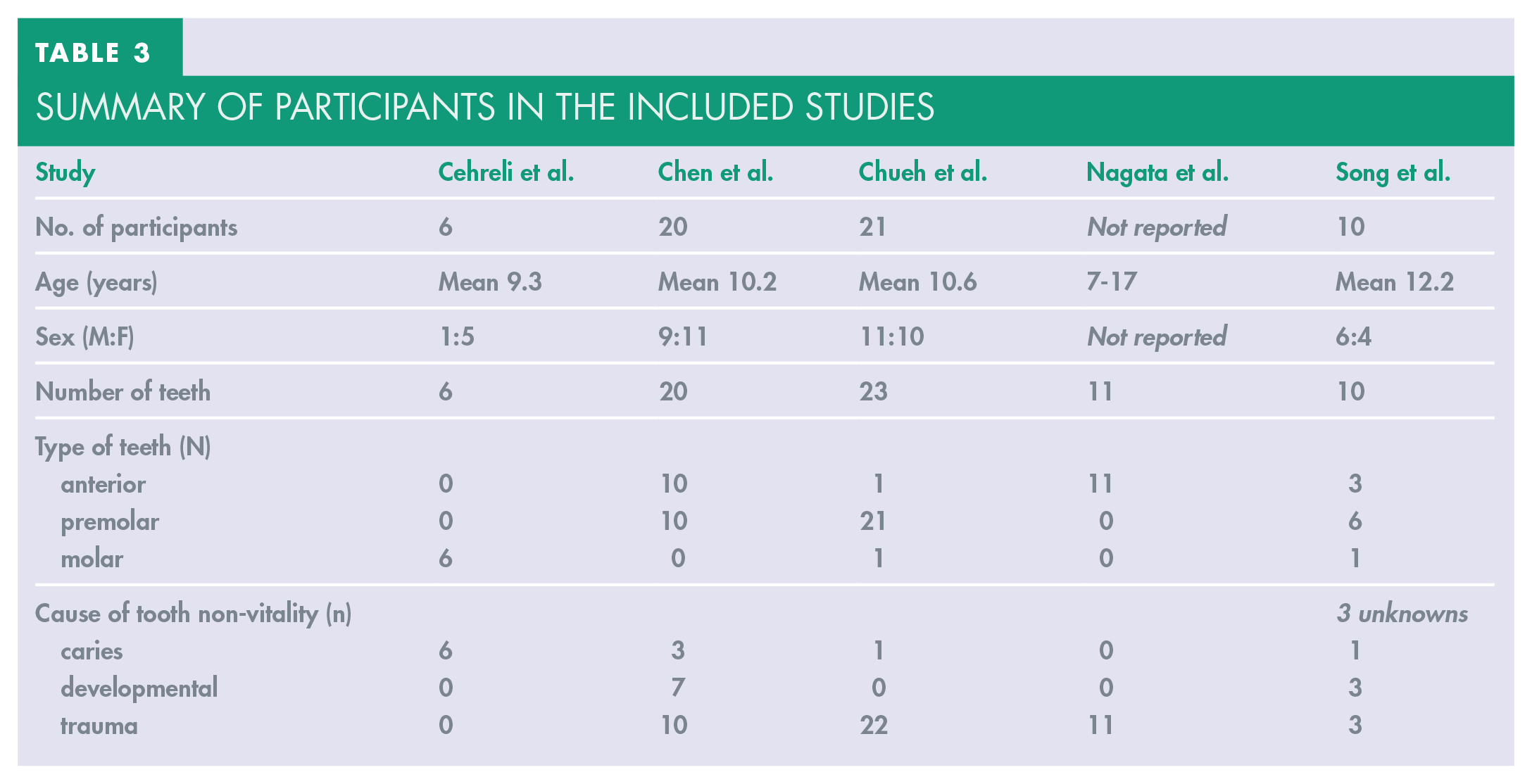
Key characteristics of the studies and the population details included in the review are summarised in Table 2 and 3.
Key characteristics of the included studies
Summary of participants in the included studies
The details of the intervention are summarised in Table 4. All four studies showed some similarities in the REP sequential stages including disinfection, review, re-disinfection and final coronal seal of the tooth using a mineral trioxide aggregate (MTA) restorative dental material. These steps were sufficient to classify the procedures as regenerative endodontics, however, there were other variations in the details of the REP demonstrating heterogeneity in the intervention between the studies.
Interventions and comparators used in the included studies (NaOCl = sodium hypochlorite, CHX = chlorhexidine gluconate)
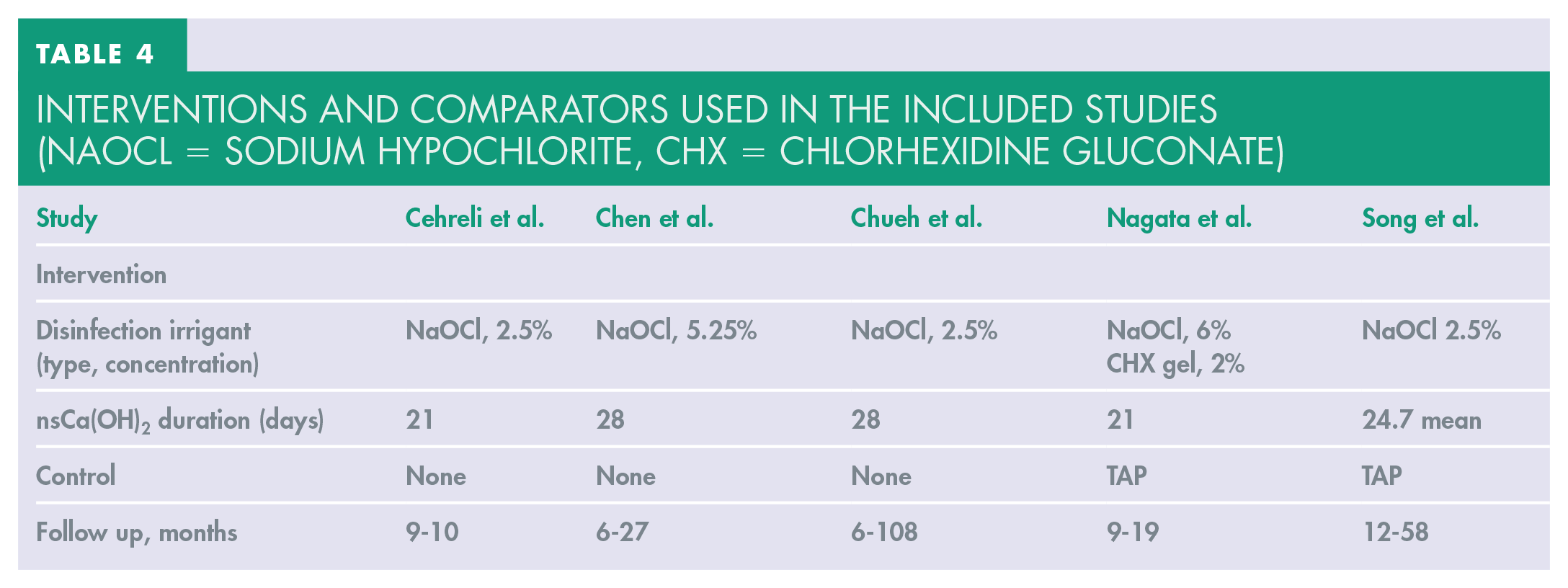
Of the five studies only one 34 had quoted following the recommended guidelines from the American Association of Endodontists or European Society of Endodontology for REP.4,13
Due to heterogeneity in the study population, interventions, outcome measures and follow up regimes, meta-analysis of data was not possible. Instead a narrative synthesis was used on the outcome data.
Primary outcome
Pre-operatively, of the 70 teeth included across the five studies, 62 showed pre-treatment radiographic evidence of periapical pathology. 70 teeth were non-responsive to vitality testing, although two studies did not report any quantitative vitality testing data.32,34
Post-operatively, the studies reported that all teeth had survived. Clinical signs indicative of infection (pain, swelling, sinus, TTP) were absent for all 70 teeth. There was a trend for reduction in periapical pathology size early in the REP (reported at 3-12 weeks) and complete absence of periapical pathology at 8-12 months (Table 5).30,32,33,34
Primary outcome data
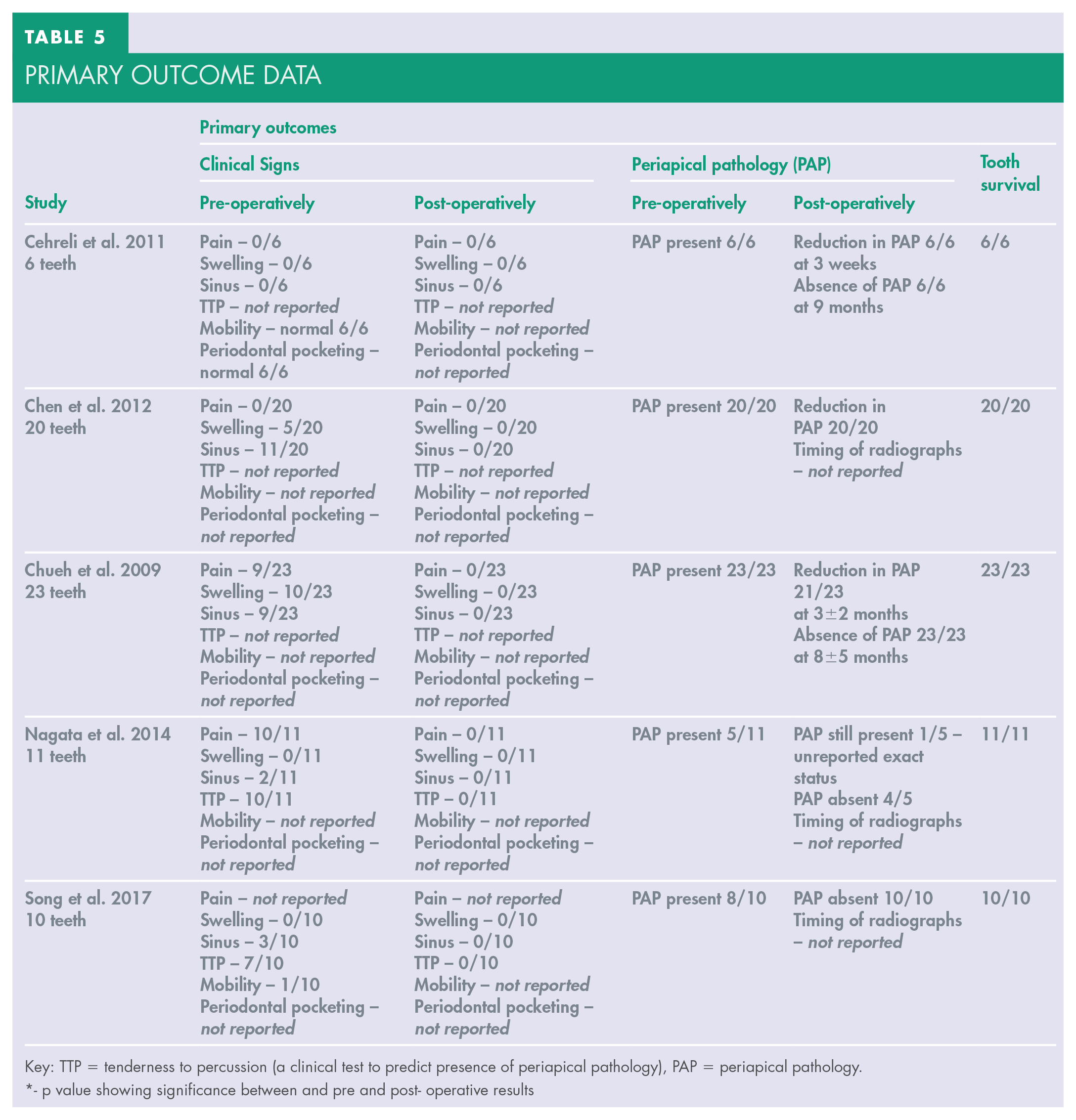
Key: TTP = tenderness to percussion (a clinical test to predict presence of periapical pathology), PAP = periapical pathology.
- p value showing significance between and pre and post- operative results
Secondary outcomes
The secondary outcomes reported were variable and included:
Complete root development 32
No studies reported any patient-reported outcomes.
Methodological quality and risk of bias
The five studies were quality assessed to estimate the overall quality of the evidence and confidence in the results (Table 6 and 7).
Quality assessment of quantitative retrospective observational studies using the Effective Public Health Practice Project Tool (EPHPP) 30
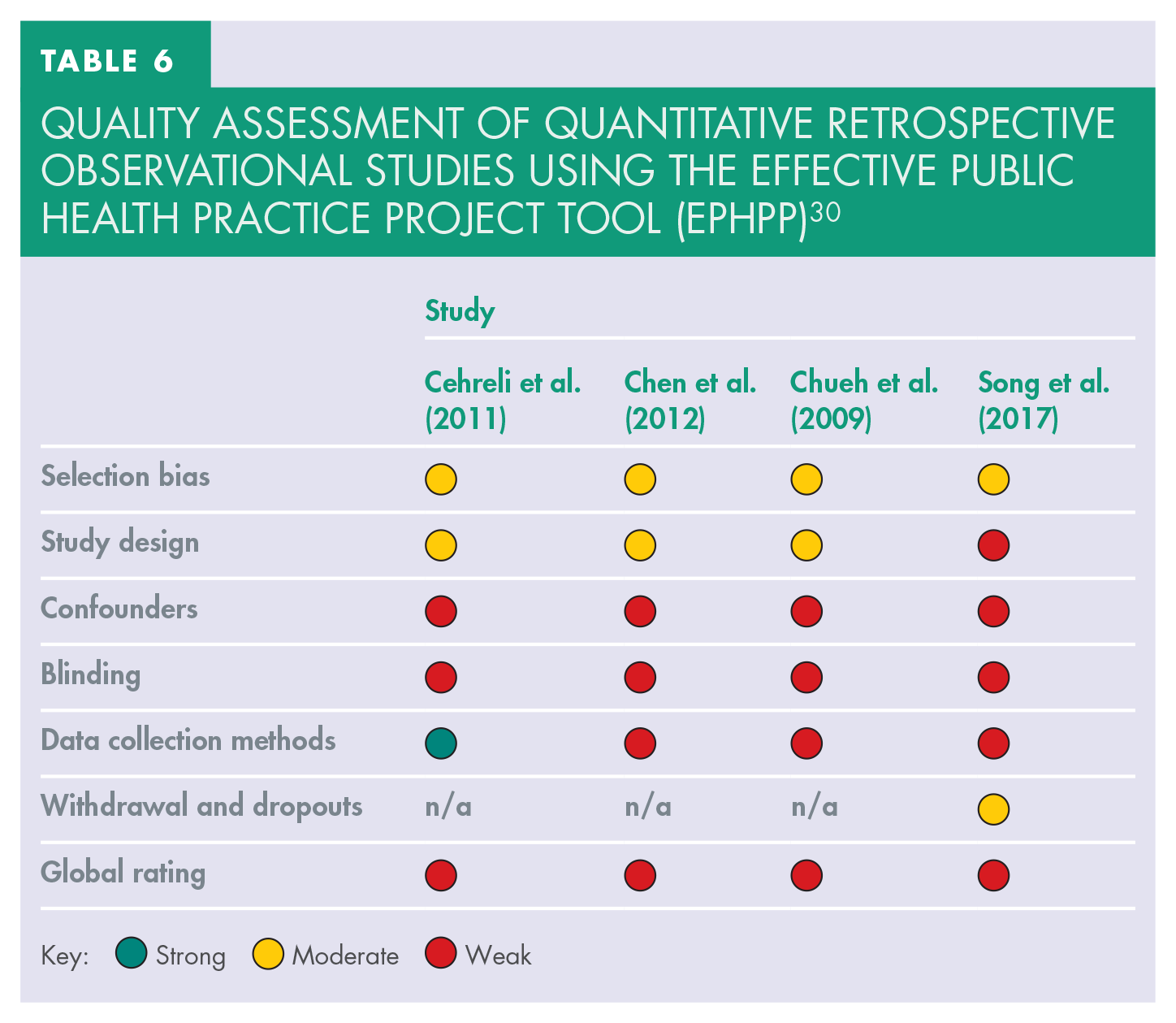
Key: Strong Moderate Weak
Quality assessment of randomized controlled trial using the Cochrane Risk of Bias Tool 29
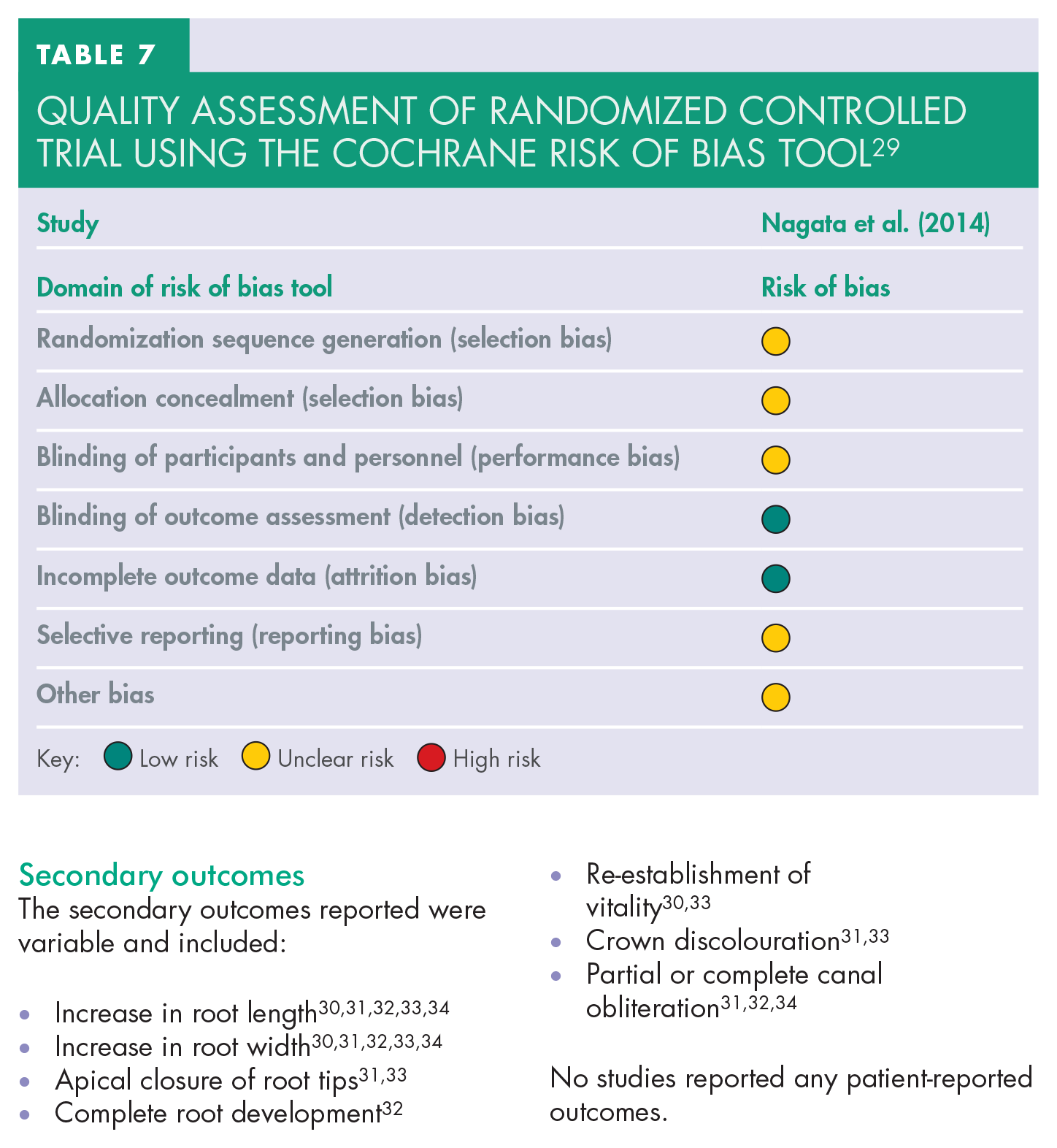
Key: Low risk Unclear risk High risk
Discussion
Primary outcomes
Overall, the management of infection in all five studies resulted in survival of all teeth and elimination of all clinical signs of infection. The mean recall period for the 5 studies was 21.6 months (ranging from 9-108 months). Initial radiographic signs of pathology also showed signs of a reduction or absence within 6-9 months. Elimination of clinical signs of infection occurred even earlier, at 21-28 days, suggesting the healing period for a patient is relatively rapid and is comparable to other endodontic treatment options for managing non-vital teeth.
In all studies, disinfection was established by the combined use of a sodium hypochlorite irrigant (2.5-6%) and a non-setting calcium hydroxide intracanal medicament. One study used 2% chlorhexidine gel together with the sodium hypochlorite irrigant; the justification for this additional disinfectant is due to the ability to immediately reduce E. faecalis microbes by this combination of disinfectants. 17 Variation in the concentrations of the disinfectant irrigant and its delivery prevented direct comparisons between studies. Nonetheless, the studies consistently used a sodium hypochlorite irrigant and a non-setting calcium hydroxide intracanal medicament, suggesting this combination successfully creates the disinfected environment regardless of sodium hypochlorite concentration.
Secondary outcomes
Improvements in root development, which would be expected to have a clinical impact on the functionality and survival of the teeth, were demonstrated in the outcomes. It was not possible to directly compare root development to specific REP interventions. It can be postulated that regardless of the specific REP details, a sufficiently disinfected environment was created to allow a biological response with appropriate cells to support the continued root development. This is supported by previous research which indicates that the single most important variable for further root development in REP is the disinfected root canal. 35
Discolouration found after REP can be attributed to either one of the intracanal medicaments (triple antibiotic paste (TAP) or non-setting calcium hydroxide) or the coronal seal restorative material (MTA). However, it is difficult to control the effect of TAP on discolouration and this is suggested as a reason to remove TAP from REP.20,38 It may be beneficial to recommend the use of a non-antibiotic intracanal medicament in a REP to limit the chances of discolouration, particularly for anterior teeth and teeth that have suffered trauma causing devitalisation.
Partial or complete root canal obliteration as a result of regenerative endodontic procedures is referred to as ‘revascularization associated intracanal calcifications’ (RAIC). 34 One of the studies showed that a thin calcific barrier (partial obliteration or blockage) within the pulp canal tends to be present after regenerative endodontic procedures, more so than partial obliteration or atresia (total blockage). The prevalence of RAIC (62.1%) is increased with an intracanal medicament of non-setting calcium hydroxide use rather than TAP. 34 This is supported by evidence that non-setting calcium hydroxide can be used in apexification procedures where a calcific barrier outcome at the incomplete apex of an immature tooth is desirable. 2
The overall prevalence of canal obliterations in this review is close to that quoted by Song et al. (2017). 34 This is clinically relevant if the regenerative endodontic approach was to fail as further treatment options would be non-viable with the presence of RAIC. This may then actually be considered a contraindication for a non-antibiotic medicament use in REP.
Irrigant recommendations
The use of sodium hypochlorite in endodontics has a long and proven history of efficacy to create a desired disinfected environment in root canals.16,17 The ideal concentration of sodium hypochlorite has been shown to be 1.5-3% for regenerative endodontic procedures and is reflected in recommended REP guidelines. 4 This effectively disinfects but also allows the survival and differentiation of SCAP. 37
This review provides no evidence to contradict maintenance of the recommended guidelines of 1.5-3% sodium hypochlorite use, but this review also cannot support or make advancements to the guidelines.
It is recognised that as an adjunct to the use of sodium hypochlorite, the use of EDTA 17% solution is indicated and provides the final irrigation. Evidence shows EDTAs importance in the conditioning of dentine and exposing growth factors that aids cellular migration, adhesion and differentiation within REP. 38
Intracanal medicament recommendations
The debate over which intracanal medicament to use in REPs currently appears to carry greater weight and importance than the type of disinfectant irrigant to use in REPs.4,39 The ESE position statement has advocated a non-antibiotic intracanal medicament regime in regenerative endodontics due to the lack of evidence for using topical antibiotics in REPs. 23 Evidence suggests the disadvantages of topical antibiotics and advantages of non-setting calcium hydroxide as the intracanal medicament include:
MTA retention, as an ideal restorative coronal sealing material after REP, is best with the use of non-setting calcium hydroxide as an intracanal medicament 40
Non-setting calcium hydroxide shows no detrimental effect on the survival of SCAP that are key to the bio-engineering process of regenerative endodontics 41
Statistically insignificant differences in bacterial reduction when comparing non-setting calcium hydroxide to a clinically used concentration of 0.1mg/ml of TAP. Only a concentration of 10mg/ml of TAP significantly reduced bacterial numbers, yet coronal discolouration is credited to TAP, especially at these higher concentrations 20
Too low concentration of TAP (<1mg/ml) reduced its antibacterial efficacy 35
This evidence above originates from ex-vivo studies and there is a lack of clinical, in-vivo studies that can be used to guide appropriate clinical recommendations for the implementation of regenerative endodontic procedures.
This review confirms the evidence available for the use of non-setting calcium hydroxide as the only intracanal medicament in REPs is weak. Still, it could be argued that where evidence is equivocal but non-setting calcium hydroxide does not possess the disadvantages of TAP, it may be practical to use a non-antibiotic intracanal medicament.
Strengths and limitations
The strengths of this systematic review are:
Development of a clinically relevant question and the thorough review process used
Use of a strict inclusion and exclusion criteria
Application of a rigorous search strategy
Validated risk of bias tools were used to assess the validity and reliability of the studies
This systematic review has some limitations which then reflects on the restriction of the clinical application of the review findings:
Search bias – limitation of the number of databases searched
Reviewer bias – only one reviewer was implemented
Publication bias
Missing data – lack of retrievable data from two studies, which had to be subsequently excluded, due to non-communication from authors
Lack of standardisation in the intervention or outcome measure of the studies
Level of bias in the included studies
The inclusion of only four retrospective observational studies and one randomised control trial judged to be at high risk of bias means the results need to be interpreted with caution. Small sample sizes with selection bias, a lack of clarity in the intervention and outcome measures, a high risk of confounders and lack of blinding for analysis contribute to the high levels of bias.
Current and future research
The level of evidence in regenerative endodontics has been previously judged to be low. 7 Current guidelines recommend that apexification should be the first option when considering the presentation of a non-vital tooth with incomplete root formation and periapical pathology, unless the roots were too small to be functional post-treatment of which extraction is the best option. 42
This review, alongside the previously cited reviews24,25,42 agree that future research in REP is required. Long-term robust double-blinded randomised control trials with large sample sizes are essential to measure the true impact of REP and their outcomes. This would include controlled comparisons of different interventions, such as non-setting calcium hydroxide versus TAP, or different types and concentrations of disinfectant irrigants while maintaining a consistency in the intracanal medicament used in the REP. This will support agreements on a preferred evidence-based REP, which can then be compared to all options of non-vital immature permanent teeth in subsequent studies.
Conclusion
With the limitations of this study, it may be concluded that REP using a disinfectant irrigant of sodium hypochlorite together with an intracanal medicament of non-setting calcium hydroxide is capable of providing a disinfected environment in a non-vital immature permanent tooth root canal to eliminate clinical signs and symptoms and reduce or eliminate radiographic signs of pathology. However, the evidence base currently is weak.
REP is an advancing area of dentistry with great potential, but more long-term, robust and high levels of evidence are required to provide further recommendations to regenerative endodontics and support the position statements of the ESE. 23
Supplemental material
Supplemental Tables 1: Database search results
Database provided by MEDLINE with full text (EBSCOhost) – updated search as of April 2020
Database provided by Dentistry & Oral Sciences Source (EBSCOhost) – searched December 2018
Database 3 provided by Embase (Ovid) – updated search as of April 2020
Studies excluded following review of the full text with reason for exclusion
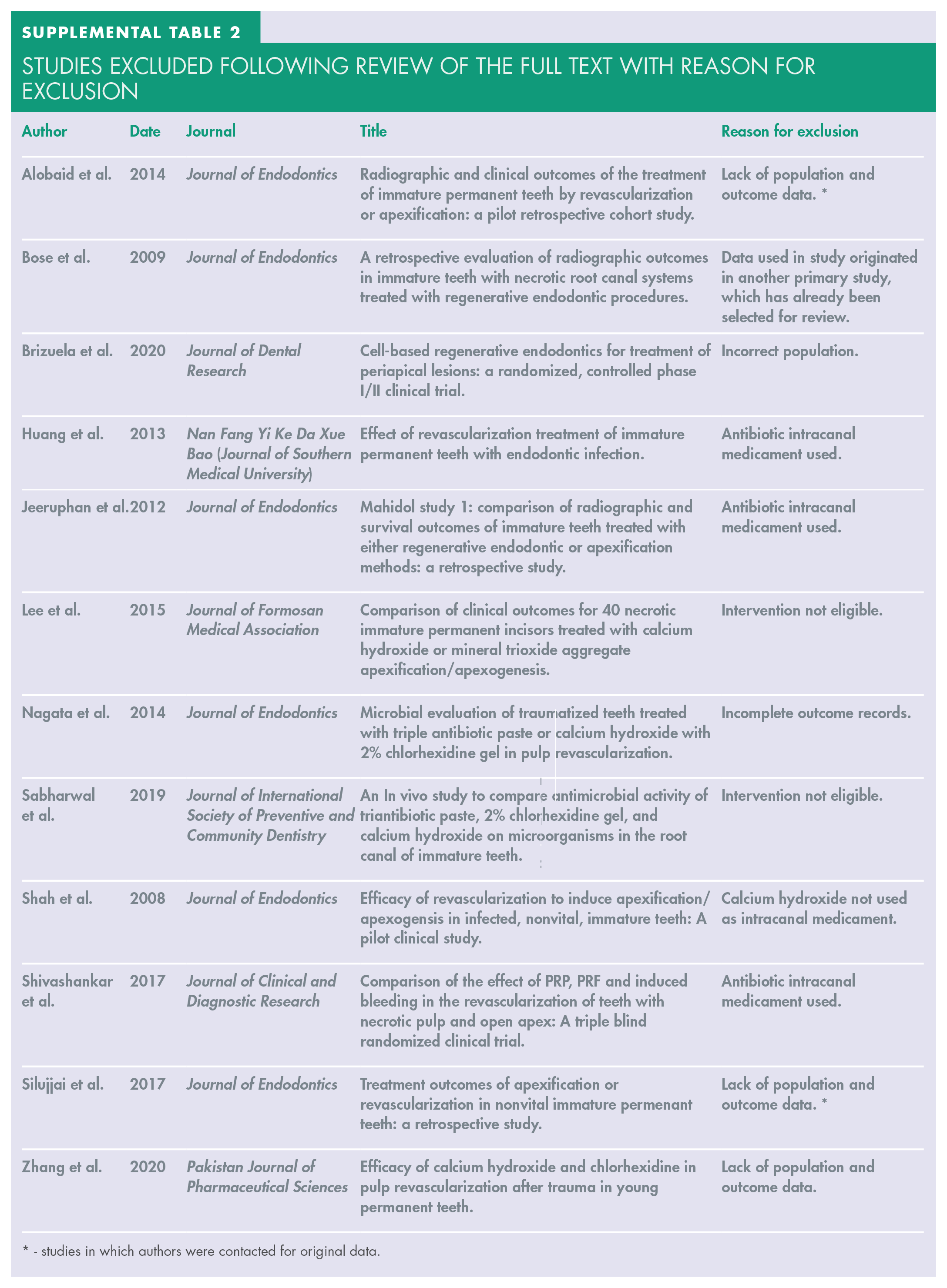
- studies in which authors were contacted for original data.
Data extraction

Abbreviations - nsCa(OH)2 = non-setting calcium hydroxide, TTP = tenderness to percussion test, PAP = periapical pathology, NaOCl = sodium hypochlorite, CHX = chlorhexidine gluconate, n/a = data not available, LA + adren’ = local anaesthesia and adrenaline.
Footnotes
Acknowledgements
Illustrations courtesy of S Batty (Senior Lecturer BA (Hons) Interior Architecture & Design, MA Design (Interior), Sheffield Hallam University).