
Abstract
The general assessment and extra oral examination of the dental patient can identify undiagnosed or undisclosed medical conditions, such as malignancies, endocrine conditions and signs indicating raised cardiovascular or cerebral vascular risk. This knowledge may influence dental treatment, and could impact the morbidity and mortality of the patient. This article gives an overview of the general and extra oral examination of the dental patient.
Learning Objectives
To understand the importance of performing extra oral examination in the dental setting
To understand the association between clinical findings on extra oral examination and associated medical comorbidities
To establish a systematic and reproducible pattern for extra oral examination
Introduction
Dentists, dental hygienists and therapists are clinicians forming part of the wider healthcare team involved in the management of the dental patient in totality. Dentists not only diagnose and treat dental conditions involving the teeth and the gums; they are also ideally positioned to examine face, skin, lymph nodes and the joints and muscles of the head and neck. The assessment of the patient can be divided into general examination and extra oral (head and neck) examination followed by intra oral examination. This article will cover the general and extra oral assessment.
The assessment of the patient commences the moment they walk into the room. Information can be obtained from their general and facial appearance, skin, mobility and even smell. These aspects can all be informative and provide clues to the patient’s medical history.
The general appearance and demeanour of the patient can also provide information on their medical problems. Is the patient happy, anxious or scared? Do they look tidy, neglected or unkempt? Note their physical appearance, their body build (obese, slim, thin or cachectic). As clinicians, we almost automatically observe these features, but it is beneficial to note any unusual findings.
The following categories are useful to consider:
Signs of distress or anxiety
Posture, motor activity, gait
Dress, grooming, personal hygiene
Skin colour and any obvious lesions
Facial expressions
Body build
Odours (body or breath), e.g. smoker, alcohol, ketones, renal disease
Gait
As the patient walks in, note the way they walk (gait), or their need for walking aids as this can provide information. A patient who requires a stick or wheelchair should be asked about the reason for this need. The medical history may include a previous stroke, a painful gait due to degenerative changes in the spine, hip or knee or injury. Issues of mobility are important as they may influence where it is best to carry out dental treatment, e.g. on the ground floor. Does the patient need assistance into the dental chair? If so, what type of assistance? A number of pathological gaits have been described, such as the classic shuffling gait seen in Parkinson’s Disease, and ataxic gait, as seen in cerebellar disease, which some describe as ‘gait of acute alcohol intoxication’ where there is a clumsy, staggering movement with legs wide apart. This may present secondary to a cerebrovascular accident (CVA). Identifying that the gait is abnormal allows the awareness of possible relevant medical history even before the patient utters a sound.
Skin
The patient may have the yellowish skin of jaundice or show other signs of liver disease. It is then important to consider altered drug metabolism and an increase in risk of bleeding and malignancy. They may show signs of sun damage in pale skin type, such as pigmented or crusted lesions, that may represent basal cell carcinomas, squamous cell carcinomas, or even melanomas.
Facial appearance
A patient’s facial appearance or expression may provide clues to their conditions. Moon faces of Cushing syndrome, mask like faces of Parkinson’s, or prognathism of acromegaly. Malar flush may indicate that the patient has mitral stenosis, pulmonary hypertension, polycythaemia, or it may simply be idiopathic.
Clothing/dress
Are they appropriately dressed for the weather? Patients with hypothyroidism feel the cold, whilst those with hyperthyroidism may have thin clothes on in winter. Patients with bipolar disorder may attend with bizarre dress sense, colourful or strange garments. As the majority of patients with mental health problems are cared for entirely in primary care, they are likely to present in dental practice. These individuals need to be identified so that their care can be modified if required 1 .
Hands
We often shake hands when greeting patients. Hands can provide clues, not only of medical conditions, e.g. rheumatoid or osteoarthritis, but also of the patient’s ability to carry out oral hygiene. We all recall the numerous causes of clubbing, including lung disorders and inflammatory bowel disorders amongst others.
Communication
The importance of communication skills and tailoring communication to the individual cannot be underestimated. The need to consider the patient is paramount, be they a child, adult, or adult with special needs. This is not covered in this article, but Dougall and Fiske 2 provide useful tips beneficial not just when treating special care patients.
Extra oral examination
Assessment of the face
Start by looking at the standing patient. Assess the symmetry of the face as well as the head and neck region. This can also be done if the patient is sat upright in the dental chair. Most of us have some asymmetries, but significant asymmetries on comparison of one side to the other should be noted. This asymmetry may be bony or soft tissue in nature. It may be acute or chronic, or it may be secondary to previous surgery, e.g. tumour resection or CVA. It may have occurred following injury, such as a fall, and the patient presents to the dentist with deranged occlusion and facial asymmetry due to a mandibular fracture.
Examination of the eye
Looking at a patient’s eye can give the dentist an insight into what possible systemic conditions the patient may have. Corneal arcus or xanthelasma may indicate dyslipidaemia and a possible increased risk of cardiovascular disease, diabetes or stroke. Proptosis (bulging eye) may signify endocrine disorder (Graves’ disease), or occasionally even malignancy. Acute presentation of proptosis is less likely at the dental surgery, but if seen following a facial injury, it may represent a retrobulbar haemorrhage. This is an urgent vision threatening condition, which needs immediate referral to emergency department for decompression, usually by oral and maxillofacial teams. The eye may show signs of medical conditions already known to the patient, but if they are not known, advising the patient to seek medical attention may influence their outcome.
Examination of the neck
Inspection of the neck
Medical examination starts with inspection, followed by palpation and percussion. Inspect and identify scars on the neck that may indicate previous surgery (thyroidectomy, tracheostomy or neck dissection for head and neck cancer). Identify any masses in the neck.
The following are key features that are important to note for lumps in the face, neck or intra-oral:
Site
Size
Shape
Surface
Colour
Consistency
Compressibility
Temperature
Tenderness
Trans illumination
Edge / Margin
Pulsatility
Fixation
Assessing a neck lump (Figure 1)
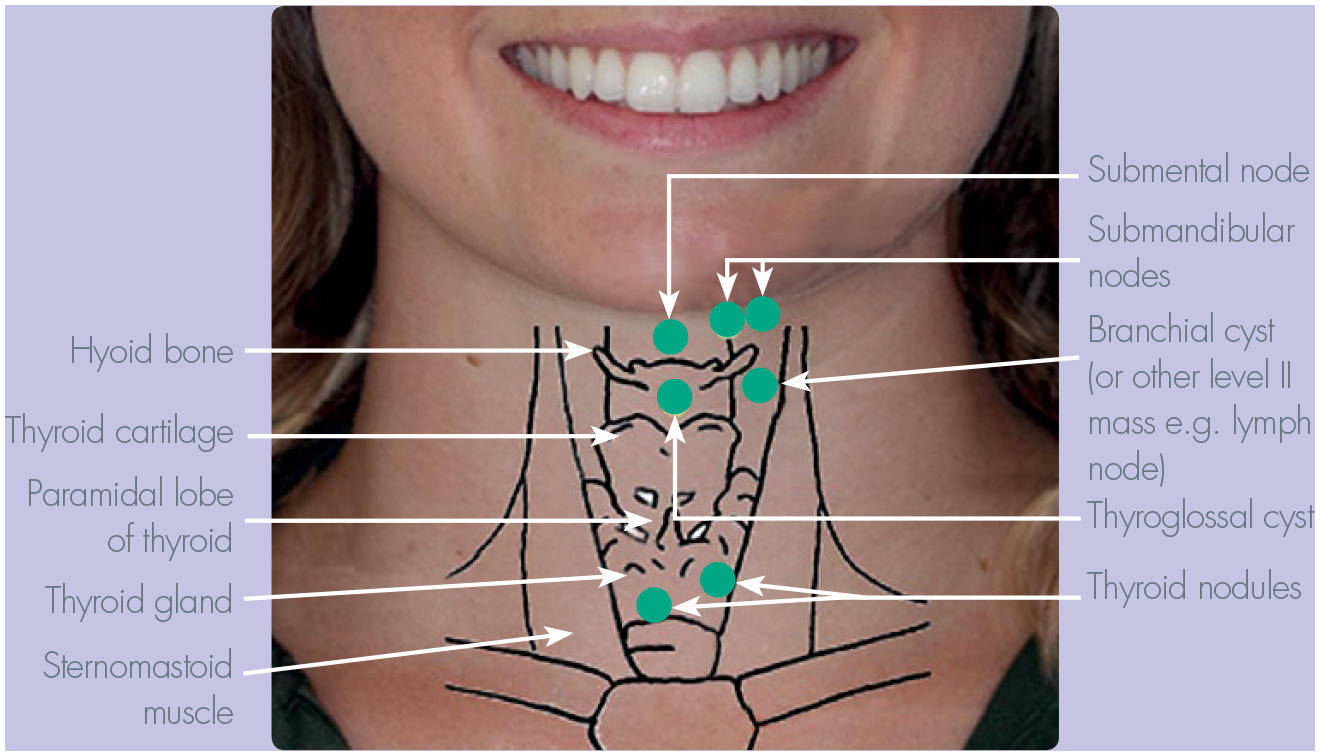
Normal anatomy and location of potential neck lump
The location of the lump provides clues as to the possible diagnosis. It is customary to divide the neck in the central and lateral neck lumps/mass and a mass or lump in the anterior or posterior triangle of the neck (Figures 1, 2 and 3). Consideration of the normal anatomy in terms of the layers of tissue from superficial to deep will help formulate the differential diagnosis: skin (sebaceous cyst), fat (lipoma), bone (osteoma). Similarly, knowledge of the normal anatomical structure in the region of the lump, mass or swelling will also provide clues to the likely diagnosis. Enlarged lymph nodes often present as multiple palpable lesions, whilst most other lesions are usually single (with the exception of thyroid nodules).
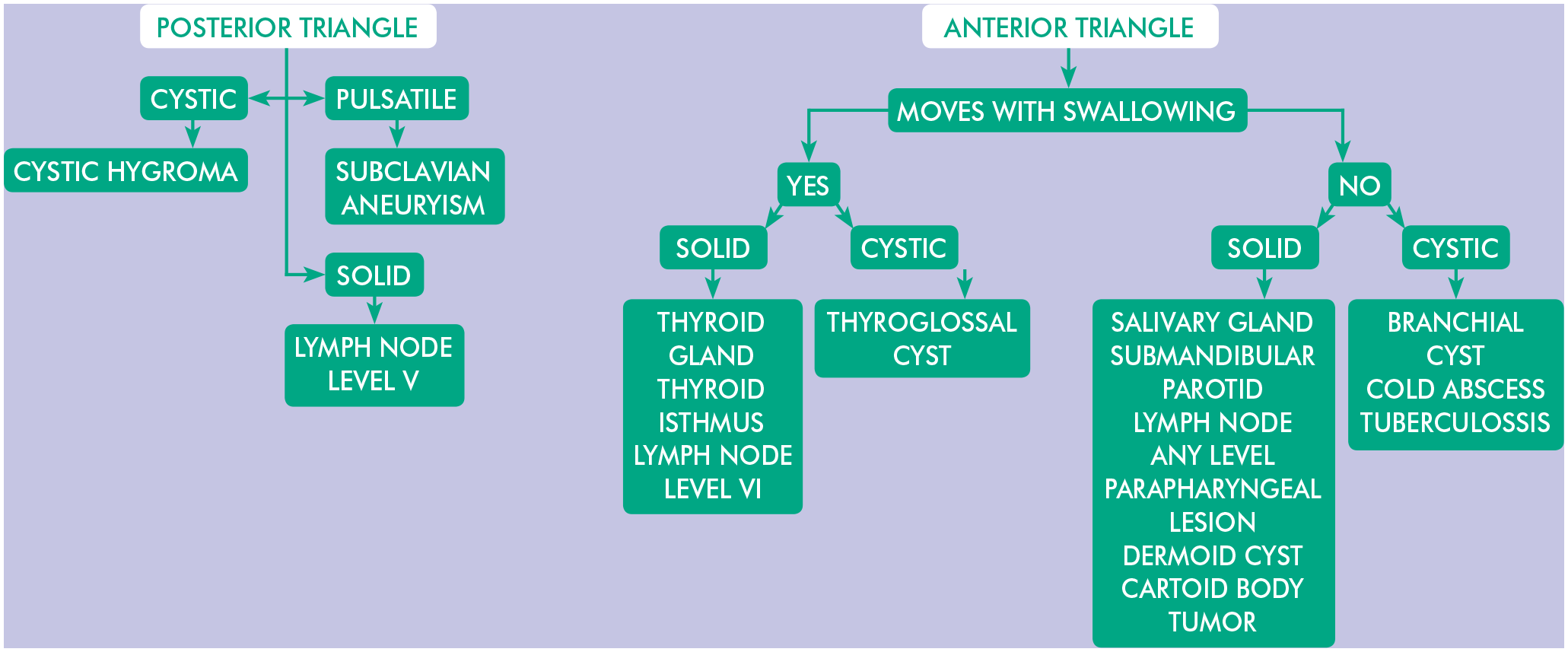
Neck lump in relation to site
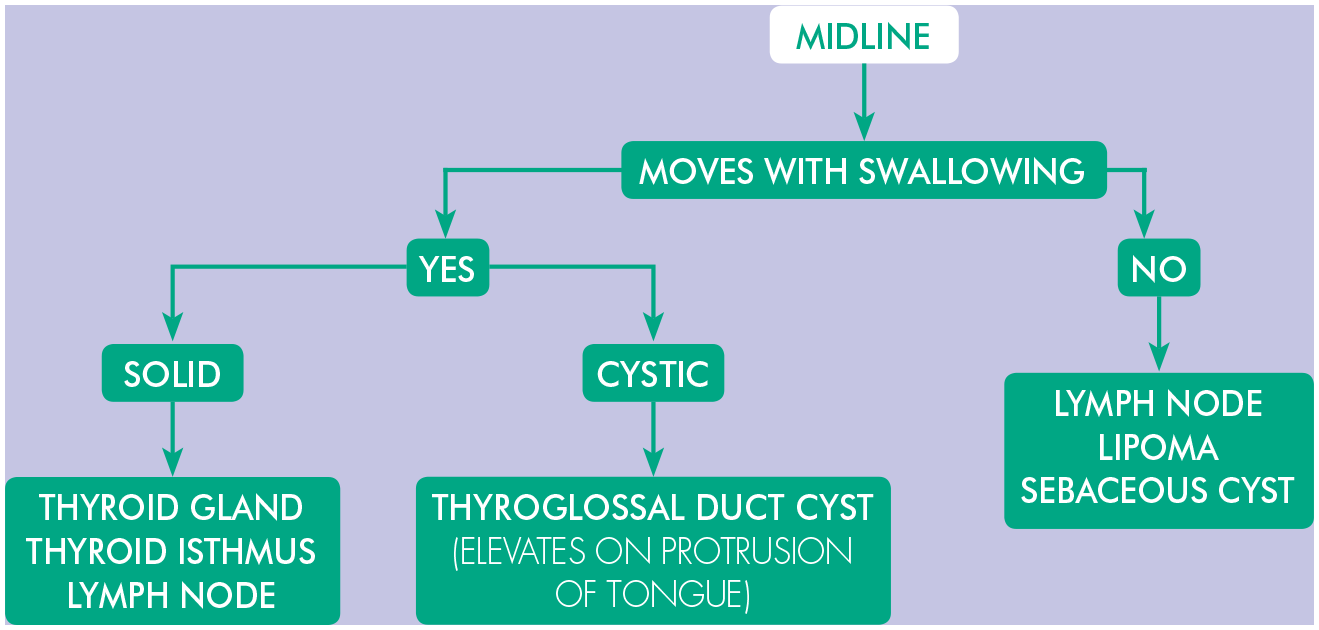
Neck lump in relation to site
Palpation of lymph nodes
Examination and palpation of the cervical lymph nodes should be carried out routinely to assess for palpable and or tender lymphadenopathy (Figure 4). Lymph nodes are normally not palpable. If they are palpable then note the size, site, number consistency, tenderness and mobility of the nodes. Look for possible reasons for the lymphadenopathy, signs of infection within the drainage pathway and systemic infection, and always consider malignancy. Ask about risk factors (smoking and alcohol intake), and red flag signs for oral cancer (weight lost, change of voice, dysphagia, otalgia, night sweats). Assess for risk of oral cancer if an adult presents with an unilateral enlarged lymph3,4.
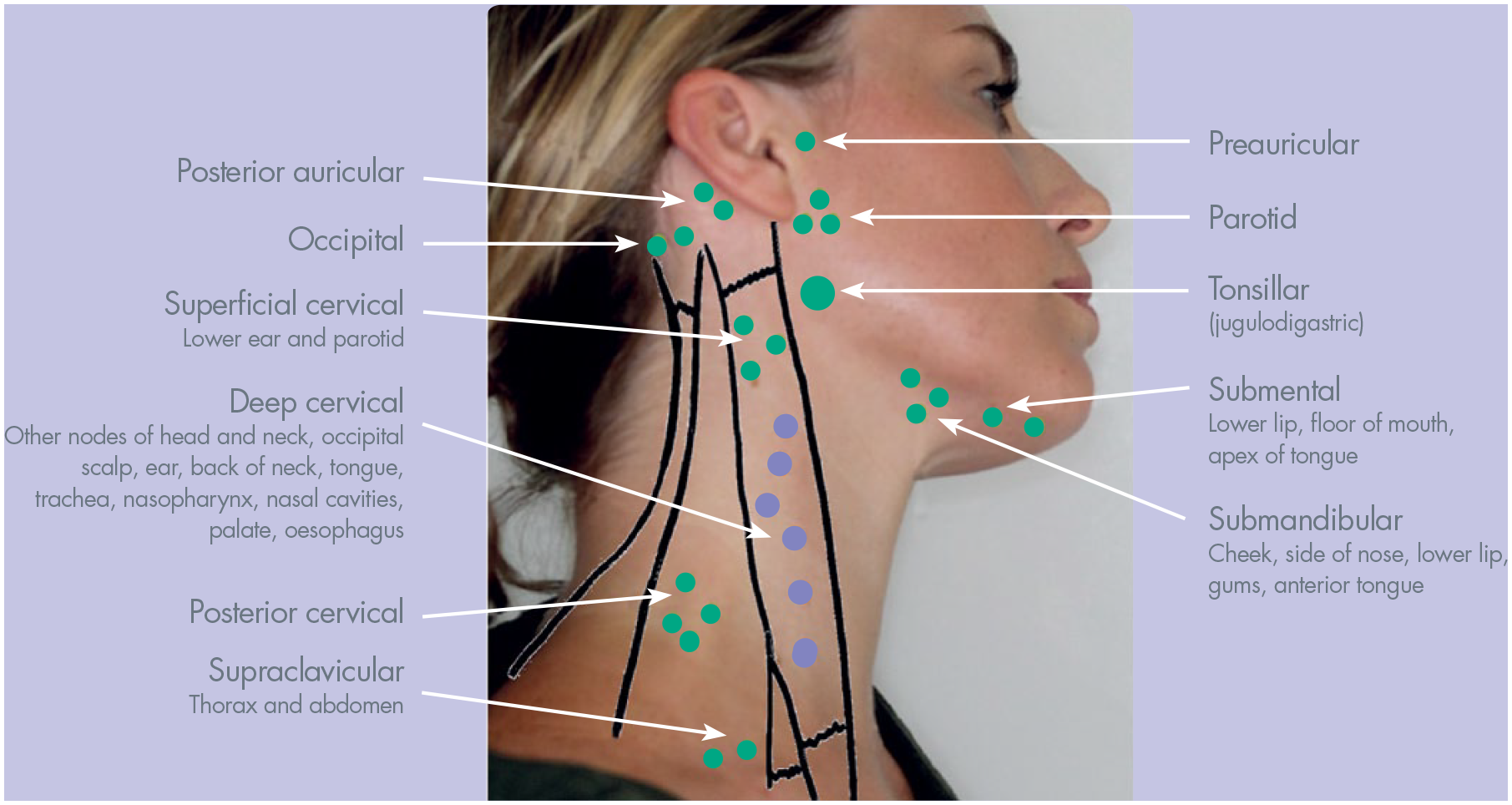
Lymph nodes in anterior and posterior triangle of neck
Ask the patient to sit up in the dental chair, stand behind them and palpate the cervical lymph nodes. Patients tend to try to help by extending their neck, which makes examination difficult. The neck should be relaxed and slightly flexed. Palpate each group in order, using the pads of the fingertip in a slight rolling motion. The suggestion is to palpate each side of the cervical chain independently to avoid the theoretical risk of carotid massage.
Lymph node groups to palpate:
Submental
Submandibular
Pre-auricular
Post auricular
Occipital
Cervical chain (upper, middle, lower)
Supraclavicular
If there is a submandibular mass/swelling, bimanual palpation will often help to determine if the mass is the submandibular gland. This is carried out by having one finger inside the mouth gently palpating the floor of the mouth. The other hand is pushing the submandibular mass upwards and feeling the mass between the hands. One may feel a salivary stone if there is a history of meal time symptoms, such as swelling in association with food.
TMJ examination (Figure 5)
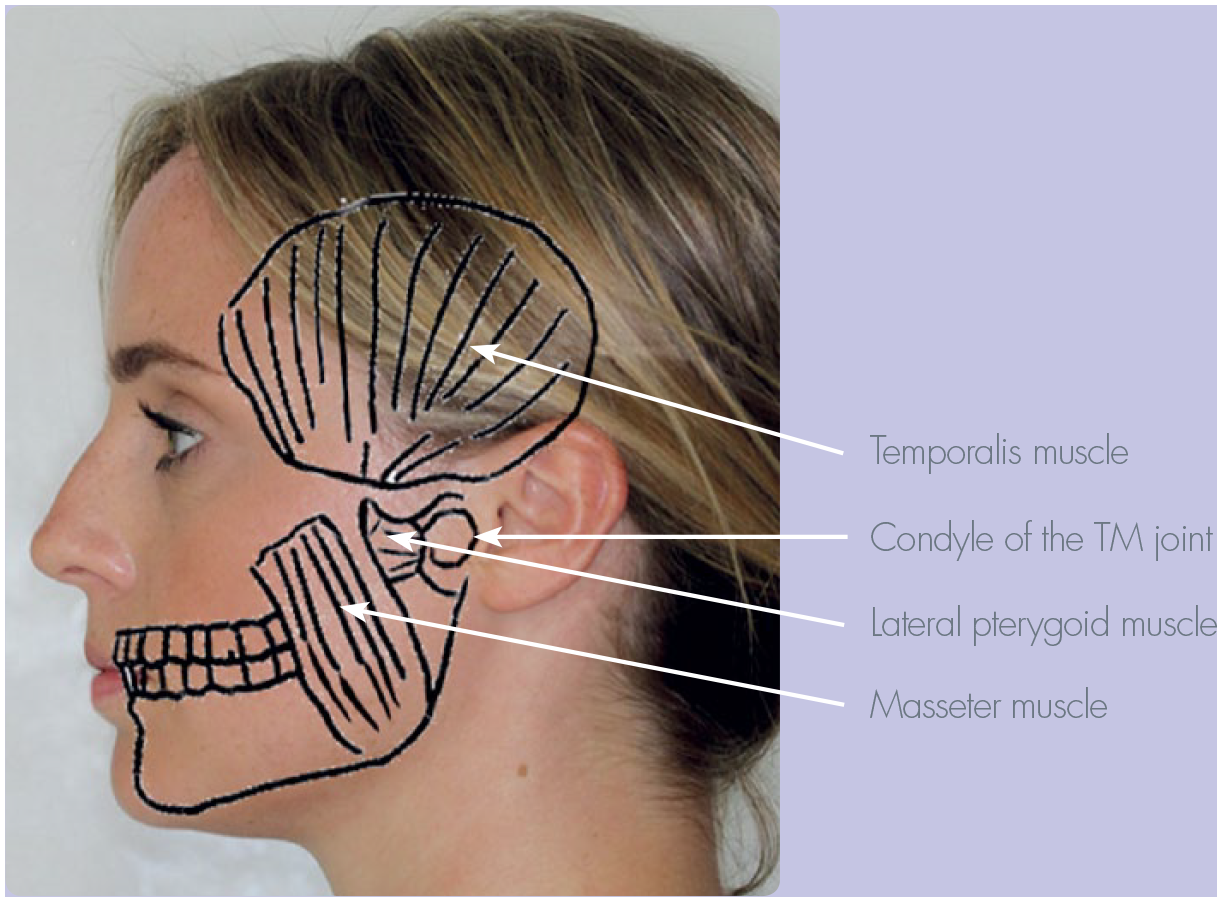
TMJ and muscles of mastication
Examination of joints classically follows the pattern of LOOK, FEEL, and MOVE. Look for redness or swelling over the TMJ. Press gently over the TMJ and ask if it is painful. Ask the patient to open and close their mouth and palpate and listen for clicks or crepitus. Note any deviation in mouth opening and the side of the deviation. The mandible often deviates to the side of pathology. Record any limitation in mouth opening. Normal maximum mouth opening is 40-50mm with 35mm opening being an acceptable range of jaw opening 5 . Assess for extent of protrusion and left and right lateral excursion. Note if one side is more limited than the other. Assess the masticatory muscle, the masseters, temporalis and lateral pterygoid muscles. Request that the patient clench and feel the bulk of the masticatory muscles by direct palpitation for masseter and temporalis. Assessment of the inferior head of the lateral pterygoid muscles is classically carried out intra-oral by gentle palpation laterally behind the maxillary tuberosity. Although this is routinely carried out by many clinicians, there is some concern over its validity and reliability 6 .
Ask the patent to clench and palpate the masseter and temporalis muscles extra-orally. Ask if there is tenderness of the muscle as you palpate. There may be trigger points within the muscle that is more tender. Extra oral palpation of the masseter muscle provides information on the superficial fibres, whilst feeling the bulk of the masseter muscle with a finger inside the mouth and thumb on the outside provides additional information on the deep fibres.
Temporomandibular disorder is characterised by one or more of the following features: tenderness on palpation over the TMJ, joint sounds, masticatory muscle tenderness and deviation mandible, along with signs of parafunction: scalloping of tongue, linear able on buccal mucosa, sign of tooth substance wear and possible tooth fracture.
Cranial nerve examination
The most likely cranial nerves a dentist may need to examine are the trigeminal (V) and facial (VII) cranial nerves. Infections of the mandible, including osteomyelitis, may present with altered sensation. Objective assessment and documentation of the neurology will be important as infection, trauma (fractured mandible), iatrogenic following surgery and malignancy are all possible causes of altered sensation. Sensory changes due to infection often improves as the infection resolves, in contrast to malignancy. A patient presenting with a swollen face likely to be a parotid swelling requires examination of the facial nerve (VII). The most common parotid tumour is pleomorphic adenoma, which is a benign tumour. However, facial nerve involvement in association with a parotid mass would be suggestive of a malignant tumour.
Trigeminal Nerve (V cranial nerve) provides the sensory supply to the face and motor supply to the muscles of mastication. There are three sensory branches of the trigeminal nerve: ophthalmic, maxillary and mandibular. The motor supply is assessed by observing and feeling the bulk of the masseter and temporalis muscles. Power can be assessed by asking the patient to then open their mouth against resistance.
The facial nerve (VII cranial nerve) supplies motor branches to the muscles of facial expression. This nerve is assessed by asking the patient to raise their eyebrows, close their eyes and keep them closed against resistance, puff out their cheeks and reveal their teeth (See Figure 6). The images show a patient with a left sided lower motor neuron facial nerve palsy as shown by the involvement of the left forehead. There is asymmetry in the parotid gland region with concavity on the left side indicative of previous surgery.

Facial nerve examination
Safe guarding concerns
The initial consultation and examination may raise concerns to the clinician about the possibility of safeguarding. There is a potential link between severe dental decay in children, resulting in the need for incision and drain, with dental neglect and overall general neglect 7 . The safeguarding tool 8 has useful information. For children, concern can be discussed with the GP.
Summary
A comprehensive general and extra oral examination of the patient can be performed without undue increase in time in the dental practice setting. Although seemingly lengthy, many aspects of the inspection can be carried out as the patient enters the surgery. This, in conjunction with a thorough medical history, will provide information to allow the safe and holistic care of dental patients. Utilisation of preformed questionnaires or pre-set fields in electronic notes would ease the documentation. Dentists and dental care professionals are trained and work within an area where they may identify unknown medical conditions. They can make a difference to a patient’s prognosis with a timely referral or simply advise that they seek medical attention.