
Abstract
Background:
Negative attitudes toward people who use drugs (PWUD) can hinder their engagement in healthcare and contribute to poor clinical outcomes. While harm reduction-informed care may improve healthcare worker attitudes and patient experiences, limited research has examined its acceptability within HIV clinical settings.
Objectives:
This study aimed to assess healthcare workers’ attitudes toward PWUD and their acceptance of harm reduction principles within HIV care clinics and to examine associated sociodemographic and work-related factors.
Design:
Cross-sectional quantitative study.
Design:
In 2022, 128 healthcare workers from three HIV care clinics in Birmingham, AL and Pittsburgh, PA, completed a self-administered electronic survey via REDCap. Multivariable linear regression was used to examine associations between attitudes toward PWUD and acceptance of harm reduction practices, adjusting for relevant covariates.
Methods:
Overall, healthcare workers reported generally positive attitudes toward PWUD, though variations by location, race, and years of experience were observed. More negative attitudes toward PWUD were associated with lower harm reduction principles acceptance (b = −0.29, p = .001). Independent predictors of lower harm reduction acceptance included working in Birmingham versus Pittsburgh (b = −0.34, p = 0.001) and being identified as Black or African American versus White (b = −0.45, p = 0.001). Healthcare workers with 6–10 years and > 20 years of experience working with people with HIV reported higher harm arm reduction acceptance (b = 0.45, p = 0.003 and b = 0.62, p = 0.02, respectively), compared to those with ⩽5 years of experience.
Results:
These findings underscore the need for targeted interventions that improve harm reduction acceptability among HIV care workers, particularly those shaped by location, race, healthcare worker experience, and attitudes toward PWUD, to support the integration of harm reduction into HIV clinical practice.
Plain language summary
Healthcare providers can have poor attitudes towards people who use drugs. These stigmatizing attitudes make it harder for patients who use drugs to stay in care. This can cause poor healthcare outcomes. We believe that using harm reduction strategies in healthcare might help. Harm reduction does not assume that all people who use drugs want to or are able to stop their drug use. Harm reduction also says that all patients should be treated with respect and that patients should have a say in their own healthcare planning. However, there’s not much research on how well harm reduction is accepted in HIV care settings or what kind of providers are more open to these approaches. To understand this better, we did an online survey with 128 healthcare workers from three HIV clinics in Birmingham, Alabama, and Pittsburgh. We did this survey with healthcare workers who provide medical care, like doctors and nurses, as well as healthcare workers who do not provide medical care but see patients in their settings, like front desk staff. The point of the survey was to see their attitudes towards people who use drugs and their acceptance of harm reduction ideas. We found that providers who took our survey were less likely to accept harm reduction if they were from Birmingham rather than from Pittsburgh. Black providers were less likely to accept harm reduction than white providers. Healthcare workers who had poor attitudes towards people who use drugs also were less likely to accept harm reduction. Providers with more years of experience caring for people with HIV were likely to accept harm reduction. Since harm reduction care might improve outcomes for people with HIV including those who use drugs, it is important for us to find ways to help providers build harm reduction into their practices.
Background
People who use drugs (PWUD) experience stigma in healthcare settings, contributing to poor clinical outcomes.1,2 Historically, healthcare workers have endorsed abstinence-based or punitive approaches in caring for patients who use drugs, viewing addiction as a moral shortcoming rather than a medical issue. 3 PWUD are frequently confronted with negative attitudes and multiple experiences of stigma within healthcare settings, and healthcare workers have expressed either a lack of readiness or a lack of satisfaction when working with these patients.4–8 Previous research demonstrates that some healthcare workers hold negative perceptions of PWUD, characterizing them as violent, disobedient, and responsible for their own conditions. 7 These negative attitudes and stigma impact how PWUD engage in medical treatment. PWUD experience reductions in the quality of healthcare services provided,7,9–11 in turn resulting in poor healthcare outcomes, including suboptimal retention in care,12–14 discontinuity of treatment, 15 fatal and non-fatal overdose events,16,17 injection-related infections,18,19 reliance on non-prescription medications to manage pain, 20 and discharging oneself against medical advice. 21
Stigma experienced in healthcare settings is particularly salient for people with HIV (PWH), for whom engagement in care is significantly associated with viral suppression.22–25 The same structural factors that increase risk of HIV infection (e.g., income inequality, access to healthcare) 26 also increase the likelihood of developing substance use disorders; PWH have nearly a 48% substance use disorder prevalence rate. 27 Substance use can significantly impact HIV care, complicating treatment adherence and exacerbating health issues. 28 PWH who use drugs tend to experience greater morbidity and mortality rates compared to PWH who do not use drugs, even when adjusting for age. 29 On the whole, PWH who use drugs experience intersecting stigmas tied to drug use, HIV status, and criminalization, which impede patient-healthcare worker relationships. 30
While therapeutic attitudes among healthcare workers do not always reflect overt prejudice, negative attitudes—such as reluctance to engage with PWUD—are closely linked to stigmatizing behaviors in clinical settings. These attitudes can contribute to the enactment of structural stigma within healthcare environments. In this way, healthcare worker attitudes represent a key pathway through which stigma influences clinical interactions and patient outcomes.7,31 Harm reduction has gained prominence as a pragmatic and humanistic approach to addressing negative outcomes associated with substance use and harmful drug policies.32–37 There is ample evidence of associations between harm reduction strategies and reductions in illicit opioid use38,39 and fatal overdose. 40 Syringe service programs decrease the transmission of HIV among people who inject drugs 41 and are highly cost-effective,42–44 and medications for opioid use disorder (MOUD) are known to reduce overdose deaths, illicit opioid use, and improve patient’s quality of life.41,45 Moreover, MOUD reduces hospitalizations, healthcare costs, and overall healthcare resource utilization. 46
While harm reduction is commonly associated with a range of services designed to reduce the adverse outcomes of substance use (e.g., syringe services, naloxone distribution) rather than solely focusing on abstinence as the ultimate treatment objective, harm reduction is also a relational approach to care that emphasizes the patient-healthcare worker relationship, that is, relational harm reduction. Relational harm reduction operates as a compassionate and non-judgmental approach that is non-punitive, supports patient autonomy, and focuses on improving the engagement of PWUD with the healthcare system.47,48 Recent work amplified conceptualizations of harm reduction first established by people with lived and living substance use experience to operationalize opportunities for healthcare workers to incorporate relational harm reduction approaches in clinical settings. 47
Despite the compelling evidence supporting the importance of harm reduction approaches to care, studies have revealed mixed attitudes among healthcare workers toward accepting these strategies. Some work to date has explored acceptance of harm reduction, finding that harm reduction acceptability varies by healthcare worker role, 49 treatment settings, and geographic locations. 50 However, these findings are limited, largely focus on structural harm reduction approaches but not relational, and do not consider the full healthcare team including both clinical and non-clinical healthcare workers.
Both clinical and non-clinical staff (e.g., front desk staff, administrators) play pivotal roles in shaping how PWUD perceive their care. While previous research has demonstrated the influence of clinical staff members’ acceptance of harm reduction and perceptions of care among PWUD, 51 there is a noticeable gap in studies focusing on both attitudes toward PWUD and the acceptance of harm reduction among non-clinical staff. Front desk staff are the initial points of contact for patients and may influence the degree to which they feel welcomed or stigmatized, and thus shape their healthcare experiences. Therefore, it is crucial to understand how attitudes among these and other non-clinical staff may contribute to patient engagement for the population of PWH who use drugs. 52 These gaps in knowledge hinder our ability to effectively tailor interventions and training programs for healthcare worker teams that may improve harm reduction acceptability and ultimately health outcomes of PWH who use drugs. To our knowledge, no study has examined the relationship between clinical and non-clinical staff members’ attitudes toward PWUD and their acceptance of harm reduction, particularly across different roles. Within HIV care clinics, this study aims to (1) test the association between staff’s attitudes toward working with PWUD and their acceptance of harm reduction and (2) explore characteristics of staff, including sociodemographics, that are associated with their substance use stigma and harm reduction acceptability levels.
Methods
This observational cross-sectional study was conducted in Birmingham, Alabama (AL), and Pittsburgh, Pennsylvania (PA), USA, with a non-random purposive sample. 53 The study is reported according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) for reporting cross-sectional studies. 54
All healthcare workers—both clinical and nonclinical staff such as front desk personnel, social workers, nurses, medical assistants, and physicians—working at one of three HIV care clinics serving PWH who use drugs (one clinic in Birmingham, AL and two in Pittsburgh, PA) were invited to participate in a one-time, web-based survey to develop a deeper understanding of healthcare workers’ attitudes toward PWUD, as well as the ways that these attitudes are associated with the acceptance of harm reduction.
Site-specific co-investigators or research team members distributed the survey using email messages that included confidential REDCap 55 links. All clinic staff were invited to access the survey link, where they received detailed information about the study’s purpose, voluntary nature, data confidentiality, and incentives prior to providing informed consent. Participants then completed an electronic eligibility screening and consent form. Those who met the inclusion criteria and provided consent proceeded to complete the survey, which was administered in English.
Healthcare workers were eligible if they (1) worked at one of three study sites for at least 1 year and (2) provided service or care to PWH or PWUD at high risk for HIV acquisition. We defined “healthcare worker” as anyone with face-to-face contact with patients, including front desk/reception staff, social workers or case managers, research coordinators, dieticians, and medical workers such as nurses, physicians, and physician assistants.
Over 130 healthcare workers were eligible for participation (including physicians, nurses, medical assistants, social workers, behavioral health staff, and front-desk personnel). However, due to the anonymous nature of survey distribution and to protect confidentiality, we did not track or record the number of individuals who received the invitation but declined to participate. We aimed to recruit 125 healthcare workers for this survey based on the number of eligible healthcare workers at participating HIV care clinic sites. Healthcare workers received a $25 incentive after completing the survey, which remained open from April through October 2022. The University of Pittsburgh Institutional Review Board approved this study via expedited review.
The three participating HIV clinics varied in size, structure, and patient populations. The Positive Health Clinic at Allegheny Health Network in Pittsburgh, PA, serves over 950 PLWH annually, with approximately 40% reporting current illicit substance use or current or past injection drug use. The University of Pittsburgh Medical Center (UPMC) HIV/AIDS Program also in Pittsburgh, serves over 1700 patients, with approximately 20% reporting substance use disorder, current illicit substance use, or current or past injection drug use. The University of Alabama at Birmingham (UAB) 1917 Clinic in Birmingham, AL, serves over 3500 PLWH, with approximately 33% reporting current or lifetime illicit substance use, and approximately 10% reporting current or lifetime injection drug use. These clinics operate in distinct policy and service environments: the Pittsburgh clinics are embedded in a harm reduction-supportive ecosystem with established linkages to syringe service programs and MOUD healthcare workers, while the Birmingham clinic operates in a more restrictive environment where syringe service programs remain illegal.
In this study, we defined “drugs” to include illicit substances and prescription medications used in ways other than prescribed. We excluded alcohol and cannabis, as these substances—while cannabis remains criminalized at the federal level—are often perceived as less stigmatized compared to prescription drugs that are misused or substances more uniformly criminalized and penalized.56,57
Measures
Acceptance of harm reduction was measured using the Harm Reduction Acceptability Scale (HRAS). 58 There are 25 statements within the scale whereby participants express their agreement or disagreement regarding harm reduction strategies, substance use, and PWUD. The HRAS was scored based on guidance from the original author, who granted permission for its use and instructed us to reverse all items such that 1 = strongly disagree and 5 = strongly agree. In this reversed format, higher scores reflect greater acceptance and support for harm reduction principles. This scoring approach ensures internal consistency and interpretability aligned with the author’s intended use. One item was removed from this study (an alcohol-related item that was not pertinent to our research question). The HRAS does not have any cut-off scores. Potential mean scores on the scale range from 1 to 5, with higher scores indicating greater harm reduction acceptance while lower scores indicate lower acceptance of harm reduction. In the original validation study, the Cronbach’s alpha of HRAS was found to be 0.83 59 ; in ours, it was 0.92.
Healthcare workers’ attitudes toward providing care to PWUD were measured using the Drug and Drug Problems Perceptions Questionnaire (DDPPQ). 60 The DDPPQ was used to assess healthcare workers’ therapeutic attitudes toward PWUD. While the DDPPQ does not directly measure stigma in the form of prejudice or discrimination, its subscales—role adequacy, role legitimacy, motivation, self-esteem, and job satisfaction—reflect attitudinal dimensions that influence healthcare workers’ willingness and readiness to deliver care to PWUD. Consistent with literature that frames stigma as a broader construct encompassing structural barriers, healthcare worker disengagement, and clinical discomfort,7,31,61 we conceptualized negative therapeutic attitudes measured by the DDPPQ as proxies for enacted or structural stigma within healthcare settings. The 20-item questionnaire measures five sub-dimensions of negative attitudes toward PWUD: Role adequacy refers to a healthcare worker’s confidence in having the essential knowledge and skills to effectively work with PWUD (seven statements); Role support involves the belief that colleagues and supervisors provide assistance and guidance in the healthcare worker’s work with PWUD (three statements); Job satisfaction reflects a healthcare worker’s perceived level of fulfillment and contentment in their work with PWUD (four statements); Role-related self-esteem refers to a healthcare worker’s self-assessment of their ability to work competently with PWUD and confidence in their capacity to impact clients and achieve successful outcomes positively (four statements); and Role legitimacy pertains to the extent to which healthcare workers believe that it is their responsibility to work with PWUD (two statements). Responses were recorded using a 7-point Likert scale (1 = Strongly agree to 7 = Strongly disagree). The DDPPQ questionnaire and the subscales do not have any cut-off scores. Potential mean scores from the overall questionnaire ranged from 1 to 7, with low scores indicating positive attitudes, whereas high scores indicating negative attitudes toward working with PWUD. In our study, the Cronbach’s alpha for the DPPQ was 0.88, similar to 0.87 in the original validation study. 60
While the DDPPQ was originally developed and validated for clinical healthcare workers (Watson et al., 2007), such as physicians and nurses, subsequent research has extended its use to a broader range of service healthcare workers. For example, Albery et al. (2003) applied the DDPPQ to measure therapeutic attitudes among non-clinical healthcare workers, including probation officers working with PWUD. 62 In our study, we included both clinical and non-clinical healthcare-affiliated staff whose roles involve interaction with patients in contexts where attitudes toward substance use are likely to influence care and service delivery. Although this represents an extension beyond the original clinical validation sample, the DDPPQ’s core constructs—such as role adequacy, role legitimacy, and motivation—are conceptually relevant to the responsibilities of these staff members.
Because some of the healthcare worker sites had small numbers of healthcare worker types, we captured age as a categorical variable to support the protection of healthcare worker confidentiality. We collapsed the original 10 categories into 4 for this analysis to ensure equal distribution across categories. Sociodemographic characteristics captured in this study included healthcare worker age (four categories: 24–35, 36–47, 48–59, and ⩾60 years old), gender (three categories: cisgender man, cisgender woman, and gender minority), sexual orientation (two categories: heterosexual/straight and sexual minority), and race/ethnicity (seven categories: White Non-Hispanic (NH), Native American NH, Native Hawaiian NH, Asian NH, Black NH, Hispanic/Latinx, and Mixed race). Information related to participants’ professional and occupational characteristics included the location where they worked (two categories: Birmingham, AL and Pittsburgh, PA), job title (four categories: medical service healthcare workers (e.g., physician, nurse, dietician), social service providers (e.g., social worker, counselor, peer worker], pharmacists, and administrative staff (e.g., front desk employee, program coordinator)), years of experience providing services to PWH (four categories: ⩽5, 6–10, 11–20, and > 20 years) and years of experience providing services to PWUD (four categories: ⩽5, 6–10, 11–20, and > 20 years). Other independent variables included personal experience with illegal drugs (yes/no), personal experience with friends or family members using illegal drugs (yes/no), and living with HIV (yes/no).
Analysis
Data entry and statistical analyses were conducted using Stata version 17. 63 Descriptive statistical analyses were used to describe the demographics of the sample population as frequency and proportion within categories (%). Linear regression models were used to examine associations between the HRAS, the Drug and DDPPQ, and respondents’ sociodemographic and work-related characteristics, while controlling for location of employment (Birmingham, AL vs Pittsburgh, PA). For the bivariate analyses, each independent variable was entered into a separate linear regression model with either HRAS or DDPPQ as the outcome, adjusted for clinic location. All models were estimated individually and not simultaneously to allow clearer interpretation of each variable’s independent association with the outcomes. Variables with p-values of <0.2 in these associations were included in the final multivariable model. 64 In addition, variables for job title, race/ethnicity, and location of employment (Birmingham, AL, and Pittsburgh, PA) were included in the final analysis regardless of the p-value. These variables were incorporated into the final model to ensure a comprehensive analysis of factors potentially influencing the acceptance of harm reduction.
Then, a final multivariable linear regression analysis was performed to assess predictors of harm reduction acceptability, including perceptions of drug use/drug users (DPPDQ), sociodemographic characteristics, and work-related characteristics. This model aimed to assess factors associated with harm reduction acceptability among healthcare workers. We hypothesized that negative attitudes toward PWUD would be associated with lower acceptance of harm reduction. In the final multivariable model, predictor variables were considered statistically significant at p-values of <0.05. Unstandardized regression coefficients (b) represent the estimated change in harm reduction acceptance for each one-unit change in the predictor variable. A positive b indicates a direct association (higher predictor values associated with higher outcome values), while a negative b indicates an inverse association. The magnitude of b reflects the strength of the association. Linear regression assumptions were assessed, confirming that the data met these criteria.
Results
A total of 145 healthcare workers across our three study sites completed the survey. We removed data from 17 participants due to incomplete information, and one respondent completed the survey twice, so only data from the first completed survey was included. As a result, data from 128 participants were included in the final analysis. Because recruitment messages were not sent by our study team but were generated by each site, we cannot calculate a response rate. However, from information shared by our study partners, we estimate less than 200 individuals met the eligibility criteria for our survey, suggesting a high response rate.
Table 1 presents the healthcare workers’ sociodemographic and work-related characteristics. The study encompassed a diverse range of healthcare workers, with the largest proportion (43.4%) being medical care workers. About half (48.9%) worked in Birmingham, AL. Regarding age distribution, individuals aged 36–47 constituted 35.1% of participants. Nearly three-quarters of participants identified as cisgender women and heterosexual/straight (70.3% and 74.4%, respectively). Over half (52.4%) identified as White. Just over one-third (35.8%) had <5 years of experience working with PWH, and 29.6% had <5 years of experience working with PWUD. A relatively small proportion (16.5%) reported personal experience with illegal drugs. However, more than 60% of participants indicated having friends or family members using illegal drugs.
Healthcare sociodemographic and worker characteristics in three HIV clinics in Birmingham, AL, and Pittsburgh, PA (N = 145), April to October 2022.

Table 2 presents the DDPPQ and HRAS scores. The DDPPQ scores suggested positive attitudes toward working with PWUD, with a mean score of 2.17 (SD = 0.69). The scores in the sample ranged from 1 to 3.8, within a theoretical range of 1 to 7, with low scores indicating positive attitudes. Similarly, the level of harm reduction acceptance among healthcare workers, measured by the HRAS, was reported favorably. The mean score of HRAS was 3.80 (SD = 0.56). The HRAS scores in the sample ranged from 2.4 to 4.8, within a theoretical range of 1 to 5, with higher scores indicating greater harm reduction acceptance.
Descriptive statistics of the DDPPQ and HRAS, three HIV care clinics in Birmingham, AL, and Pittsburgh, PA (N = 128), April to October 2022.
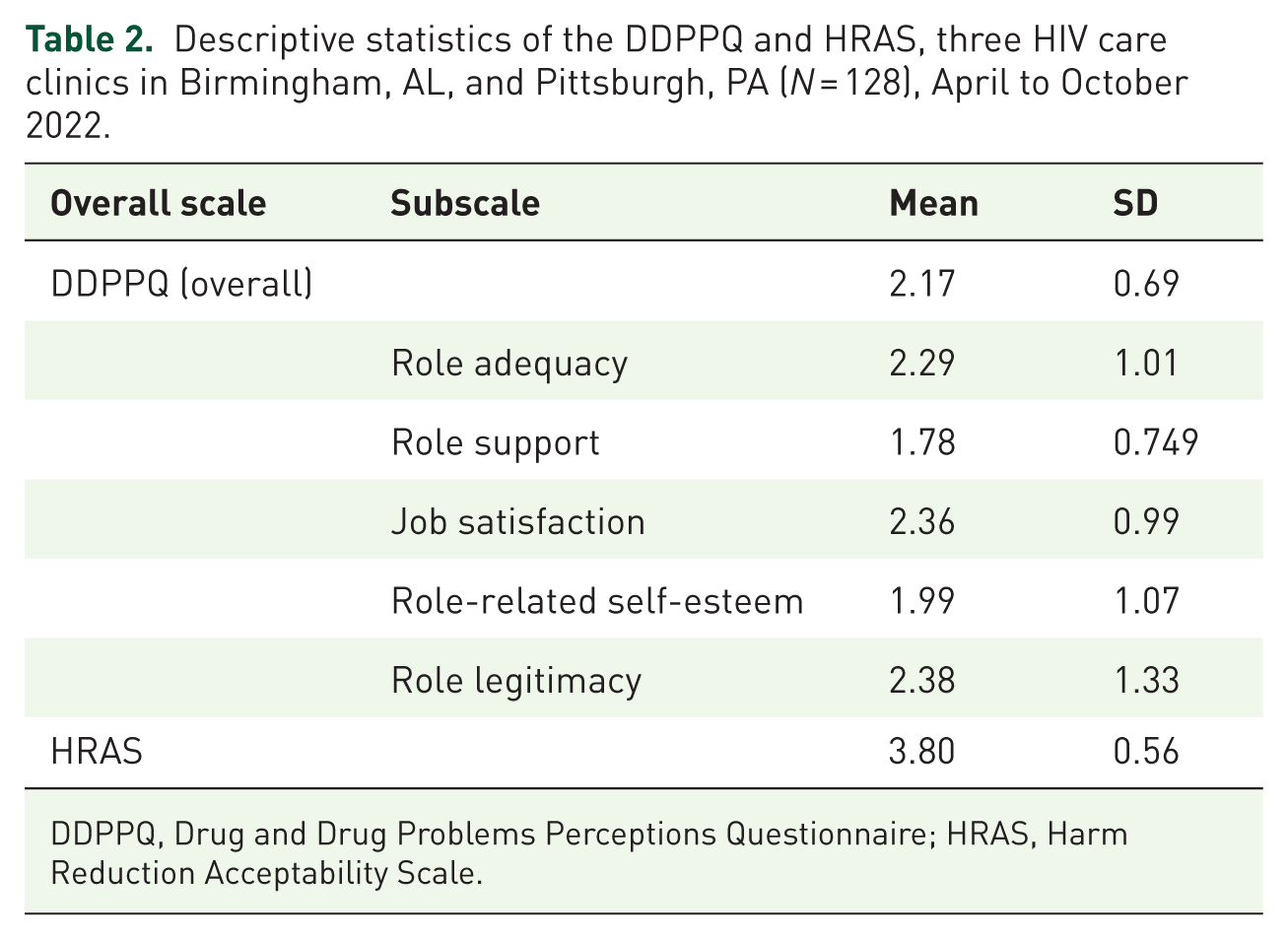
DDPPQ, Drug and Drug Problems Perceptions Questionnaire; HRAS, Harm Reduction Acceptability Scale.
Table 3 displays the outcome of location-adjusted independent associations between healthcare workers’ sociodemographic/work-related characteristics and acceptance of harm reduction. In this model, age, race/ethnicity, duration of providing services to people with HIV, personal experience with substance use, and experience with substance use among the healthcare worker’s friends or family members statistically significantly predicted harm reduction acceptance. Gender, sexual orientation, job title, duration of providing services to PWUD, and living with HIV were not statistically significant in predicting harm reduction acceptance. Specifically, healthcare workers who self-identified as Black or African American had significantly lower acceptance of harm reduction compared to those who identified as White (b = −0.43; p = 0.001). Similarly, healthcare workers aged 48–59 had significantly lower harm reduction acceptance than younger healthcare workers aged 24–35 (b = −0.28; p = 0.04). Harm reduction acceptance was higher among healthcare workers with 6–10 years of experience working with HIV compared to those with < 5 years of experience (b = 0.31; p = 0.01). Personal experience with substance use also played a role in harm reduction acceptance. Healthcare workers with no personal experience with substance use had lower harm reduction acceptance compared to those with personal experience with substance use (b = −0.27; p = 0.02). Additionally, healthcare workers who did not report substance use history within their friends or family members had lower harm reduction acceptance compared to those with such experience (b = −0.29; p = 0.005). Only statistically significant variables were included in the final multivariable linear regression model.
Bivariate associations between sociodemographic and worker characteristics and HRAS N = 128).

Each row represents a separate bivariate linear regression model assessing the association between a single independent variable and HRAS, adjusted for location of employment (Birmingham, AL vs Pittsburgh, PA). Models were not estimated simultaneously.
Reference categories.
Statistically significant p-value (<0.2) for the overall variable to move into the final model.
Statistically significant p-value (<0.05) at the individual level.
b, Unstandardized beta in linear regression; HRAS, Harm Reduction Acceptability Scale.
Table 4 displays the location-adjusted association between healthcare workers’ sociodemographic/work-related characteristics and healthcare workers’ negative attitudes toward PWUD. In this model, gender and duration of providing services to PWUD statistically significantly predicted healthcare workers’ attitudes toward PWUD. Healthcare workers who self-identified as gender minority had significantly higher negative attitudes toward PWUD compared to those who identified as cisgender men (b = 1.53; p = 0.002). In contrast, negative attitudes toward PWUD were less prevalent among healthcare workers with more years of experience. Specifically, healthcare workers with 6–10 years of experience working with PWUD (b = −0.38; p = 0.02) and those with 11–20 years of experience (b = −0.36; p = 0.02) had more positive attitudes compared to those with less than 5 years of experience. Age, personal experience with substance use, sexual orientation, race/ethnicity, job title, duration of providing services to people with HIV, experience of drug misuse among participants’ friends, or family members, and living with HIV were not statistically significant in predicting healthcare workers’ attitudes toward PWUD. Only the significant variables were included in the final multivariable linear regression model.
Bivariate associations between sociodemographic and worker characteristics and negative attitudes toward PWUD (DDPPQ), adjusted for clinic location (N = 128).
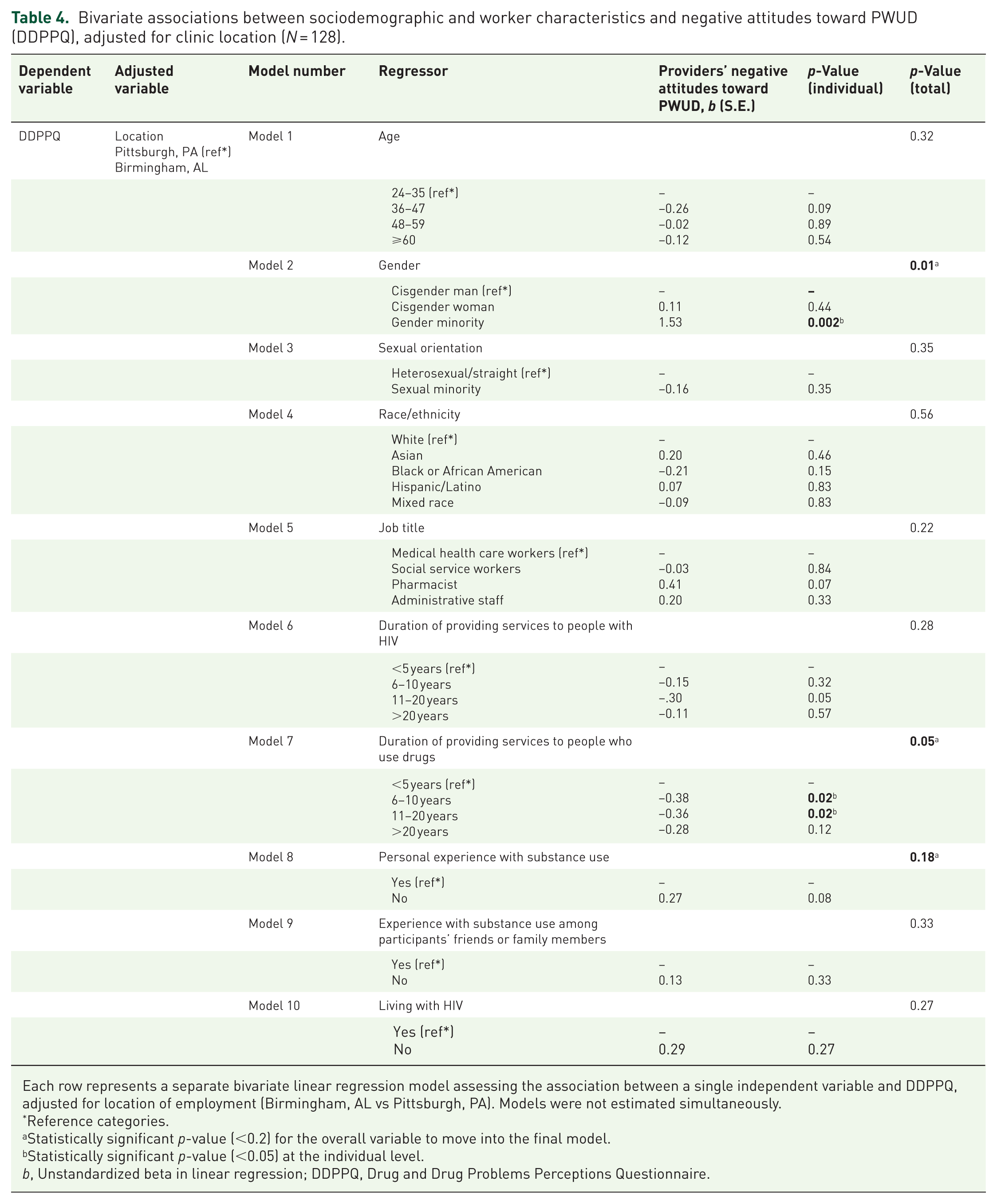
Each row represents a separate bivariate linear regression model assessing the association between a single independent variable and DDPPQ, adjusted for location of employment (Birmingham, AL vs Pittsburgh, PA). Models were not estimated simultaneously.
Reference categories.
Statistically significant p-value (<0.2) for the overall variable to move into the final model.
Statistically significant p-value (<0.05) at the individual level.
b, Unstandardized beta in linear regression; DDPPQ, Drug and Drug Problems Perceptions Questionnaire.
Table 5 presents the final multivariable linear regression model, controlling for the location of employment, job title, and race/ethnicity. The final model demonstrated a moderate to substantial fit, with an R 2 value of 0.56, indicating that more than half of the variability in the scores of the HRAS was accounted for by the independent variables, encompassing both the DDPPQ overall questionnaire and the healthcare worker’s sociodemographic and work-related characteristics. Results showed that DDPPQ scores were negatively correlated with HRAS (b = −0.28; p = 0.001), illustrating that more negative attitudes toward serving PWUD were associated with lower harm reduction acceptance. Healthcare workers who self-identified as Black or African American had significantly lower harm reduction acceptance compared with those who identified as White (b = −0.45; p = 0.001). Harm reduction acceptance was lower among healthcare workers in Birmingham, AL, compared with those in Pittsburgh, PA (b = -0.34; p = 0.001). Acceptance of harm reduction was higher among healthcare workers with 6–10 years and > 20 years of experience working with PWH (b = 0.45; p = 0.003) and (b = 0.62; p = 0.02), respectively, compared with ⩽ 5 years of experience. Age, gender, job title, duration of providing services to PWUD, or personal or friends or family members’ experience with substance use were not statistically significantly associated with harm reduction acceptance scores.
Multivariable linear regression model: Association between Harm Reduction Acceptance (HRAS) and negative attitudes toward PWUD (DDPPQ), adjusted for key covariates (N = 128).

Statistically significant p-value (<0.05).
b, unstandardized Beta coefficient in linear regression.
DDPPQ, Drug and Drug Problems Perceptions Questionnaire; HRAS, Harm Reduction Acceptability Scale.
Discussion
In our study, we found that negative attitudes toward PWUD were associated with lower acceptance of harm reduction, suggesting that healthcare workers harboring more negative attitudes toward PWUD are less inclined to support or engage in harm reduction practices. This primary finding aligns with studies demonstrating that substance use stigma and lack of acceptance among healthcare workers pose significant barriers to effectively implementing harm reduction in clinical settings.65–68 These findings also echo patients’ perspectives in qualitative and quantitative studies, highlighting how experiencing stigma in various healthcare settings detrimentally affects their access to harm-reduction services.1,11,20,68–70
We found that healthcare workers who more experienced in caring for PWH were more likely to be accepting of harm reduction. Specifically, healthcare workers with 6–10 years and over 20 years of experience caring for PWH demonstrated higher harm reduction acceptability compared with ⩽5 years of experience. The reasons for these differences are not known, but it is possible that healthcare workers with more years of experience engage deeply with patients in a way that humanizes them or that healthcare workers who inherently respect and care for PWH stay in the field longer than those with less favorable attitudes. It is also possible that there is a historical cohort effect influencing differences by years of service providing HIV care. While further research is needed to understand these nuances, findings may set the stage for healthcare worker-level interventions to improve HIV care outcomes for those who use drugs.
Although overall healthcare worker attitudes toward PWUD were generally positive, our findings highlight specific demographic and contextual factors—such as location, race, and years of experience—that continue to shape variability in harm reduction acceptability, underscoring the importance of tailored strategies to sustain and strengthen supportive attitudes across all healthcare worker groups. Compared with Pittsburgh, PA-based healthcare workers, respondents from Birmingham, AL, had lower harm reduction acceptance. This finding may be due to the conservative policy context in Birmingham, which limits access to structural harm reduction (e.g. SSPs are not legalized) 71 and where few healthcare workers prescribe buprenorphine, 72 in comparison to the political context in Pittsburgh, PA, where syringe service programs have operated legally since 2008. 73 Understanding the impact of these regional disparities on healthcare workers’ attitudes can be crucial for tailoring interventions and training programs to improve harm reduction care. In addition, healthcare workers in our study who identified as Black or African American had lower harm reduction acceptance as compared to their White counterparts. This finding is consistent with prior research demonstrating that some Black communities distrust harm reduction approaches given the country’s racist drug criminalization history, which has caused significant harm and trauma to the Black population. As a result, these individuals may hold concerns that tolerating any drug use will have the effect of further stigmatizing and oppressing Black PWUD. 74 However, more research is needed in this area to ensure perspectives of Black communities can be gathered and meaningfully applied to intervention development in a way that amplifies their voices and experiences.
Unique aspects of our study include that we assessed both clinical and non-clinical healthcare workers, and that we explored variables associated with acceptance of harm reduction in HIV clinical settings, which is important given low rates of retention in care and viral suppression among PWH who use drugs. Additional work is also needed to understand how experience in providing care for PWH affects healthcare workers’ attitudes toward PWUD and harm reduction acceptance.
Given these results, it may be beneficial to design an intervention to improve harm reduction acceptance among HIV healthcare workers that is tailored to their individual and work-related characteristics and that considers cultural and policy contexts. Although our analysis did not explore whether regional disparities and healthcare workers’ characteristics act as mediators or moderators in explaining associations with harm reduction acceptance, it is clear that future studies are needed to elucidate the role of political contexts, regional disparities, and healthcare workers’ characteristics in delivering harm reduction services for PWUD. Moreover, specific types of harm reduction strategies and stigmatizing attitudes experienced by subgroups of PWUD in healthcare settings may change over time with political and cultural shifts among healthcare workers. Monitoring these changes will be pivotal in designing harm reduction strategies that are context-sensitive and capable of addressing the challenges faced by PWUD.
Limitations
This study also has limitations that may restrict the generalizability of its findings. First, the sample was drawn exclusively from three HIV clinics located in two urban areas in the U.S. South and Northeast. As such, the attitudes and experiences of healthcare workers in other regions, particularly rural areas or jurisdictions with different harm reduction policies, may differ. Second, while our sample included both clinical and non-clinical staff, the relatively small overall sample size—especially the limited number of participants within specific staff categories, gender minorities, and racially/ethnically diverse subgroups—may have reduced our statistical power to detect group differences and limited our ability to explore intersectional effects or conduct robust subgroup analyses. Third, the use of a web-based, self-administered survey may have introduced self-selection bias, as healthcare workers with more favorable views of harm reduction may have been more inclined to participate. Fourth, because survey participation was anonymous and voluntary, we could not track non-respondents, limiting our ability to assess selection bias and potentially affecting the generalizability of our findings. Fifth, due to the cross-sectional design of this study, causality cannot be inferred. The observed associations may be bidirectional—for example, healthcare workers’ negative attitudes toward PWUD might reduce their motivation to implement harm reduction strategies, while limited acceptance of harm reduction could, in turn, reinforce or worsen negative attitudes toward PWUD. These dynamics may create a self-reinforcing cycle that negatively impacts clinical care. Additionally, unmeasured confounding variables—such as healthcare workers’ political beliefs, exposure to harm reduction training, or religious values—may also influence these associations. Longitudinal research is needed to better understand the directionality and underlying mechanisms of these relationships. Sixth, we did not assess the amount or frequency of direct patient interaction across healthcare worker roles, nor did we distinguish between prescribing and non-prescribing clinical staff. Given the heterogeneity in responsibilities and patient contact across job titles, future research should account for these differences to better understand how role-specific dynamics influence harm reduction attitudes.
Seventh, although the DDPPQ was originally validated for use with clinical staff, our study extended its application to include non-clinical staff involved in patient care. While the core constructs of the scale (e.g., role adequacy, motivation) are conceptually relevant to these roles, the instrument has not been formally validated in non-clinical populations. This limits the generalizability of findings and highlights the need for future research to adapt and validate attitudinal measures for non-clinical personnel working in healthcare settings. Eighth, it is also important to note that while our analysis suggested that healthcare workers who self-identified as gender minority had significantly higher negative attitudes toward PWUD, this finding was based on a very small subgroup (n = 2). As such, this result should be interpreted with extreme caution and cannot be generalized to gender minority healthcare workers as a whole. Future studies with larger and more diverse samples are needed to better understand the experiences and perspectives of gender minority providers. Finally, a potential limitation is the difference in scoring direction between the two primary attitudinal measures. The HRAS was reverse-coded based on direct guidance from the scale’s author to ensure that higher scores reflect greater support for harm reduction. In contrast, the DDPPQ was retained in its original scoring format, where lower scores indicate more favorable attitudes. While both approaches were justified, the differing directions may require careful interpretation when comparing findings across measures.
Conclusion
Our study explored the attitudes of multiple types of healthcare workers in HIV healthcare settings across two U.S. states with distinct policy environments. While we observed variation in harm reduction acceptance by location, these differences may reflect not only broader regional policy contexts but also institutional characteristics unique to each clinic. Given the limited number of sites—particularly the inclusion of only one clinic in Alabama—caution should be exercised in generalizing these findings to entire regions. The connection between healthcare workers’ years of experience with PWH, their sociodemographic and work-related characteristics, and their increased acceptance of harm reduction over time suggests the need for a nuanced approach to strengthening harm reduction in healthcare. Our findings underscore the importance of addressing attitudinal barriers—such as healthcare worker discomfort—which are closely tied to stigma and may hinder the delivery of equitable, person-centered care. Future work should build on this foundation to advance structural and relational harm reduction strategies that reduce stigma, improve outcomes, and promote health equity for PWUD.
To enhance acceptance of harm reduction among healthcare workers, multilevel interventions that combine education, stigma reduction, and system-level support are recommended. Training programs that incorporate lived experiences of PWUD and emphasize harm reduction as a public health strategy have been shown to improve healthcare worker attitudes and willingness to implement harm reduction approaches.11,75 Structural level – including public and organizational policies – including leadership endorsement, integration into clinical workflows, and clarity on legal and policy protections – can further legitimize harm reduction practices in clinical settings. 76 Moreover, culturally responsive approaches that acknowledge healthcare workers’ needs for integrating harm reduction into medical care, including fostering a stigma-free, welcoming environment; embracing flexible, low-threshold access; promoting healthcare worker learning; and building collaborative care teams and referral networks to support patient engagement and continuity of care. Success was defined by patient-centered outcomes such as trust, participation, and incremental health improvements rather than abstinence. 77 Taken together, these strategies may foster more widespread acceptance and implementation of harm reduction in HIV care.