
Abstract
Background:
Influenza is a significant public health challenge, characterized by severe disease progression and considerable societal burden. Patients at high risk of influenza-related complications require special attention in routine clinical practice.
Objectives:
This study aimed to compare the effects of antiviral treatments for influenza on the incidence of bacterial complications, adverse events, and disease duration in high-risk outpatients.
Design:
Multicenter, non-interventional, observational cohort study.
Methods:
The study was conducted during the 2023–2024 influenza epidemic season and included 1867 high-risk outpatients treated with oseltamivir, umifenovir, kagocel, or imidazolyl ethanamide pentanedioic acid.
Results:
Bacterial complications occurred in 18.87% (n = 335) of high-risk patients, with 17.41% (n = 309) requiring antibacterial therapy. The hospitalization rate was 1.24% (n = 22), and the average disease duration was 8 days. The incidence of bacterial complications varied among treatment groups: oseltamivir (18.96%, n = 102), umifenovir (12.17%%, n = 51), kagocel (22.00%%, n = 110), and imidazolyl ethanamide pentanedioic acid (22.64%%, n = 72). Adverse events were reported in 4.76% (n = 84) of patients, most commonly gastrointestinal disorders (91.67%, n = 77), followed by allergic reactions (8.33%, n = 7). The incidence of adverse events was significantly higher in the oseltamivir group compared to other treatments.
Conclusion:
The etiotropic agents oseltamivir and umifenovir demonstrated comparable efficacy in managing influenza in high-risk patients, as reflected by their impact on bacterial complication rates and disease duration. Both drugs may be recommended for the treatment of high-risk influenza patients.
Plain language summary
Some individuals are at a higher risk of developing serious complications from influenza. The global scientific community is increasingly concerned about the limited effectiveness of vaccines and the growing resistance to antiviral medications. These challenges highlight the importance of finding new ways to prevent and treat influenza, as well as evaluating the effectiveness of existing antiviral drugs.
This study included approximately 2000 high-risk outpatients in Russia who were treated with one of four antiviral medications: oseltamivir, umifenovir, kagocel, or imidazolyl ethanamide pentanedioic acid. Among these patients, 19% developed bacterial complications, and 17% required antibiotics. The rate of bacterial complications varied between treatments, with oseltamivir having the highest rate and umifenovir the lowest.
Adverse effects were reported in about 5% of patients, most commonly gastrointestinal issues, while allergic reactions were less frequent. Side effects were more common in the oseltamivir group compared to the other treatments.
In conclusion, oseltamivir and umifenovir were found to be similarly effective in reducing influenza complications. These findings suggest that both drugs are suitable treatment options for patients at high risk of complications.
Keywords
Introduction
Influenza is one of the most common acute respiratory viral infections (ARVI), which causes significant damage to public health and the economy and is often characterized by a severe course of disease. Wide circulation and high variability of influenza viruses provide sustainable risks of seasonal epidemics and pandemics. Thus, the 1918 influenza pandemic, according to the available information, caused at least 50 million human deaths. According to the World Health Organization (WHO), about a billion influenza cases are recorded annually worldwide: 3–5 million cases of severe disease and 290,000–650,000 deaths.1–4
Influenza complications determine disease severity and outcomes. The risk factors for influenza complications are age (under 2 years and over 65 years), chronic somatic comorbidities, and pregnancy. Patients with metabolic and nutritional disorders (including obesity), circulatory and respiratory diseases have a high risk of influenza complications. 5 Severe influenza course and the high probability of unfavorable outcomes can be due to primary influenza pneumonia or secondary bacterial pneumonia, as well as due to deterioration of the patient’s condition caused by exacerbation of chronic comorbidities. Timely start of antiviral treatment, particularly in patients at risk, allows prevention of a severe course of the disease and complications, as well as reducing the number of hospitalizations.
Diagnostic and therapeutic approaches to influenza in the Russian Federation are principally regulated by clinical guidelines. 6 The high variability of the influenza virus, the possibility of developing resistance to antiviral medications, and insufficient efficacy of influenza vaccination determine the urgency of finding new preventive and therapeutic options, as well as of assessing the efficacy of existing antiviral medications. 7 Direct-acting antiviral agents are commonly used in routine clinical practice in the Russian Federation, such as oseltamivir,8–16 umifenovir (Arbidol is the original drug product),17–21 as well as indirect-acting antiviral agents, such as kagocel22–33 and pentanedioic acid imidazolyl ethanamide (Ingavirin is a trade name).34–38
The study objective was a comparative evaluation of antiviral treatment impact on the incidence of bacterial complications of influenza, adverse events, and duration of the disease in outpatients with a high risk of complications.
Materials and methods
Study design
To achieve the research objectives, a multicenter observational study was conducted between October 2023 and April 2024 at the site of 11 outpatient clinics of Saint-Petersburg and the Leningrad region, Russia. The study included male and female patients over 18 years old, with mild or moderate influenza, who presented for medical care over the first 36 h after the onset of the first symptoms of the disease and provided voluntary informed patient consent. The investigators enrolled all patients, meeting inclusion criteria, who presented for medical attention during the study period, without exclusions for any reason (severity of the disease, historical data, etc.).
All the patients enrolled in the study had a high risk of complications due to the presence of at least one of the following conditions:
age over 60 years;
respiratory diseases (bronchial asthma, chronic bronchitis, bronchiectasis, etc.);
cardiovascular diseases (essential hypertension stage II–III, cardiac rhythm disorders, ischemic heart disease (IHD), etc.);
obesity (body mass index (BMI) > 30);
type I or II diabetes mellitus;
kidney diseases (chronic renal failure, chronic pyelonephritis, glomerulonephritis).
All the patients enrolled in the study were receiving one of the following medications (INN): oseltamivir, umifenovir, kagocel, or pentanedioic acid imidazolyl ethanamide. The dosage and duration of therapy with antiviral agents were prescribed by the attending physician according to the instructions for use. Aside from antiviral agents, a patient was prescribed supportive and other necessary therapy if needed: nonsteroidal anti-inflammatory drugs, decongestants, and saline solutions for nasal congestion; expectorants in case of cough, as well as vitamins and general tonics. In this study, the patients were maintaining concomitant treatment for their chronic diseases.
Patients with signs of bacterial infection and a need for antibiotics at the first visit were not enrolled in the study. In addition, patients who required hospitalization or started self-treatment with antiviral or antibacterial agents were also not enrolled. Throughout the study, patients were prohibited from vaccination, administration of blood products, and other medicinal products containing proteins, including diagnostic allergens.
The maximal study duration was 15 days. The visit #1 was conducted on the day of the initial presentation and included signing the informed patient consent to participate in the study, collection of the patient’s complaints, history, demographic data, and vaccination history, physical examination, assessment of vital signs, collection of a nasopharyngeal/oropharyngeal swab to diagnose influenza using polymerase chain reaction (PCR diagnostics) or a rapid test for influenza. If laboratory diagnostics of influenza were unavailable in accordance with the clinical guidelines, the diagnosis “Influenza, virus not identified” (ICD code J11) could be made based on the clinical presentation and medical history, and the antiviral treatment was prescribed, as well as supportive treatment if needed. At the visit #2 (Days 5–8) and visit #3 (Days 9–15), the patient’s compliance was assessed additionally, information about adverse events during treatment was collected, and the treatment was adjusted as necessary. To assess the safety of treatment during visits #2 and #3, the doctor recorded information in the primary documentation about the occurrence of complaints from the gastrointestinal tract, allergic reactions, other manifestations associated with side effects of treatment, or their absence. If recovered by the visit #2, the patient completed study participation. If there were signs of bacterial complications, the treatment was prescribed in accordance with conventional clinical practice. If indicated, the patients were hospitalized.
To minimize and eliminate subjectivity, the present study was conducted in 11 clinical centers. When assessing the links between the treatment regimen and the development of bacterial complications of influenza, as well as the development of adverse events as a confounder, the multivariate analysis included an indicator of patient adherence to treatment. In addition, in the comparative analysis of the studied therapy groups, such important clinical and demographic indicators as the patient’s age and BMI, the presence of a history of influenza vaccination, an ICD diagnosis (J10 or J11), the severity of the disease (mild or moderate), the number of risk factors for complications, and the number of flu symptoms were taken into account as covariates.
In case of failure to attend a scheduled visit, the patient was contacted by phone to collect information about complaints, antiviral drug regimen, supportive treatment, occurrence of adverse events, dates of hospitalization, and recovery. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (STROBE checklist is available as Supplemental Material). 39
Data analysis
The analysis of the data collected was carried out using the R Software Environment (version 4.3.2). Mode or median was used as measure of central tendency to describe parameters measured in nominal and ordinal scales, and median for parameters in interval and ratio scales. First/low (LQ) and third/high (HQ) quartile values were calculated as measures of data variability. The group nominal and ordinal parameters are presented as incidence in the absolute values and percentages, and the group quantitative parameters are presented as a median with the interquartile range. The distribution normality for parameters measured in the interval scale and the ratio scale was assessed using the Shapiro–Wilk W test, and the homogeneity of their variances was assessed using the Bartlett test. To assess the group differences in nominal characteristics, contingency tables were created, and the Pearson (chi-squared) test or the two-sided Fisher’s exact test with Holm’s correction for multiple comparisons was applied (“pairwise_prop_test” and “pairwise_fisher_test” functions from the “rstatix” package). The nonparametric Kruskal–Wallis rank test was used to assess the differences between the samples for parameters measured on ordinal and interval scales, as well as in the ratio scale. Multiple pairwise group comparisons were performed using Dunn’s test with Bonferroni correction (“kwAllPairsDunnTest” function from the “PMCMRplus” package). To visualize the results of pairwise group comparisons on graphs and tables, a conventional symbolic notation was used, which assumes marking different groups with different Latin letters. Thus, if significant differences were identified in two groups for the parameter studied, then there will be no common Latin letters in the symbolic marking of these groups. No imputation of missing values was used in this study. Single values identified as outliers were not excluded from the analysis and were not subject to any changes. The significance level was set at α ⩽ 0.05 (5%), the power of the statistical test—at 0.95 (95%).
Multiple logistic regression was used for a comparative assessment of the antiviral treatment effect on the outcomes studied, taking into account the simultaneous influence of several factors (the “glm” algorithm with a binomial distribution function). The logistic regression model allows for the estimation of the adjusted odds ratios (ORs) and their confidence intervals (CIs), as well as the degree of reliability of the difference between these values from 1. Predicates of the presence or absence of the clinical event studied were used as a binary dependent variable, for example, the development of a bacterial influenza complication (yes/no) over a certain observation period. Information about the patient’s belonging to a particular therapeutic group was used as an independent variable combined with other parameters that could also affect the clinical outcome studied. No imputation of missing values was used, and all observations with missing values in at least one of the parameters were excluded from the analysis. The coefficients of multiple logistic regression were converted into adjusted ORs with the calculation of 95% CI using the exponent function. To test the logistic regression models, a visual analysis of the remainder distributions was performed.
Study population
The study’s statistical power was calculated using the Chi-square goodness-of-fit test. Given the total sample size of 2000 patients and the observed event rates in the four treatment groups, the power of the test was found to be 89%. A total of 2005 influenza patients with a high risk of developing complications were enrolled in the study. In 138 patients, a deviation from the study protocol was revealed: the enrollment of a patient with the first presentation to a physician dated later than 36 h after onset of the first symptoms of the disease. Data on these patients were excluded from the main analysis. The final study sample size was 1867 patients, 39.64% males and 60.36% females (n = 1127). The median age of the patients was 64.42 years (56.34–70.69 years), and the mean BMI was 26.88 kg/m2 (23.67–30.37 kg/m2). The enrolment process during the season 2023–2024 corresponded to the influenza incidence rate in Russia and is shown in Figure 1.
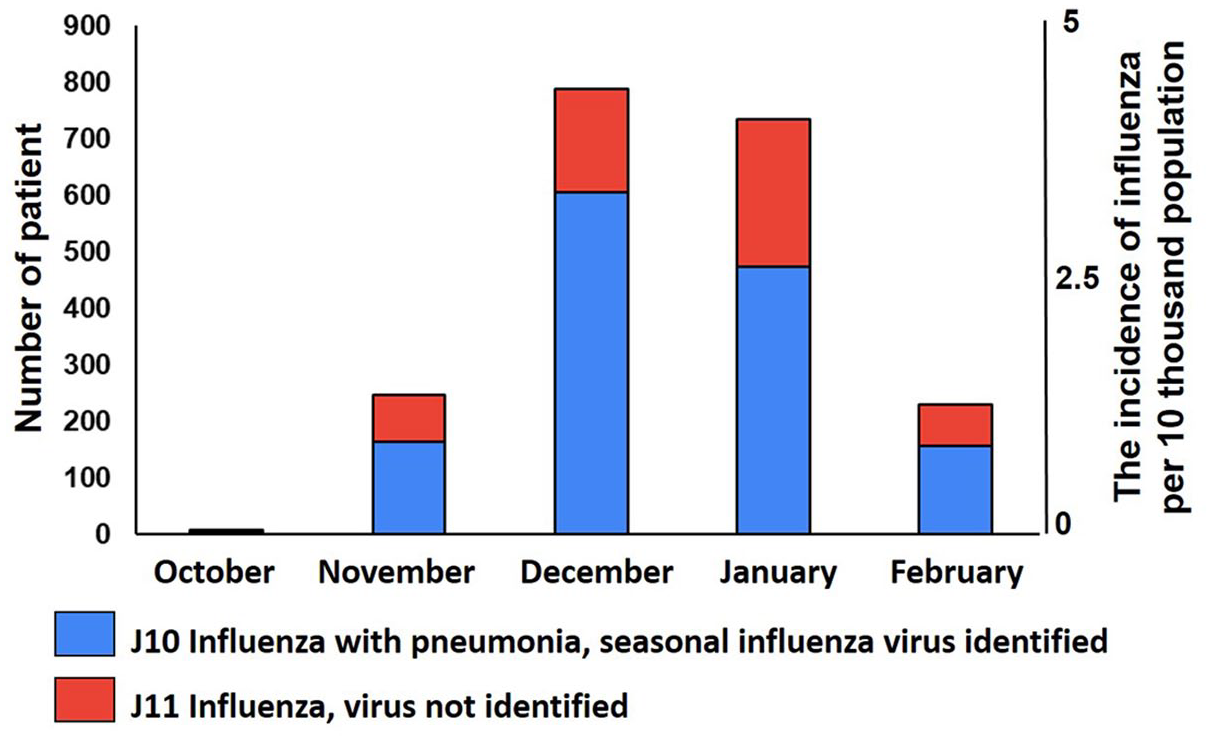
The incidence of influenza in the Russian Federation in the epidemic season 2023–2024, per 10 thousand population (red line), and the flowchart of patients’ enrollment in the study.
The most common clinical manifestations of influenza at the initial presentation were general weakness (81.15%, n = 1515), body temperature elevation above 38°C (73.76%, n = 1377), headache (73.22%, n = 1367), muscles and joints pains (71.40%, n = 1333), and dry cough (61.76%, n = 1153). Symptoms such as sore throat (54.63%, n = 1020) and nasal congestion (53.88%, n = 1006) were less common. Only 19.50% (n = 364) and 2.95% (n = 55) of patients complained of shortness of breath and nausea and/or vomiting, respectively.
All patients were divided into four groups according to the medicinal product prescribed at visit 1. Group 1 patients received oseltamivir (29.99%, n = 560), group 2 patients—umifenovir (22.98%, n = 429), group 3 patients—kagocel (28.39%, n = 530), and group 4 patients—pentanedioic acid imidazolyl ethanamide (18.64%, n = 348). Figure 2 shows a study flow diagram. Table 1 provides summary information on the distribution of nominal biomedical parameters in the patient groups studied.

Study flow diagram.
Main demographic and clinical characteristics of patient groups (count/%).

Pearson (chi-squared) test.
Two-sided Fisher’s exact test.
A comparative analysis of the distribution of nominal parameters showed that the patient groups studied were comparable in gender, history of influenza vaccination, and were not comparable in terms of the ICD code, disease severity, and two risk factors for the complicated course of the disease.
The proportion of patients diagnosed with “J10 Influenza due to identified seasonal influenza virus” in group 2 was 62.00% and was significantly less than in group 1 (75.18%, p < 0.001) and in group 3 (71.13%, p = 0.017). At the same time, a mild course of influenza before treatment was observed significantly more often among the patients who were prescribed umifenovir (87.18%), than in the group 1 (67.32%, p < 0.001), the group 3 (70.75%, p < 0.001), and the group 4 (75.29%, p < 0.001). The proportion of patients over the age of 60 years in group 4 was 55.75%, which was significantly less than among the patients in group 1 (74.46%, p < 0.001), group 2 (71.79%, p < 0.001), and group 3 (70.38%, p < 0.001). Furthermore, cardiovascular diseases were less common among the patients who were prescribed kagocel (73.96%), than in group 1 (81.79%, p = 0.002) and group 2 (84.15%, p < 0.001).
A comparative analysis of quantitative variables showed that the patient groups differ in age, weight, and BMI, as well as in the average number of risk factors for complicated influenza course, the number of concomitant diseases, and various influenza symptoms registered at the visit 1. The mean age of patients who were prescribed pentanedioic acid imidazolyl ethanamide was 61.97 years (52.13–69.14 years) and was less than in the groups of patients who received oseltamivir (65.40 years (60.38–71.39 years), p < 0.001), umifenovir (65.14 years (57.36–71.09 years), p = 0.008), and kagocel (64.43 years (56.73–70.31 years), p = 0.030). In turn, the patients in the group 2 had lower BMI (26.23 kg/m2 (23.15–30.08 kg/m2)), than the patients who received oseltamivir (27.11 kg/m2 (24.52–30.42 kg/m2), p = 0.029) and pentanedioic acid imidazolyl ethanamide (27.02 kg/m2 (23.34–31.42 kg/m2), p = 0.030).
The mean number of risk factors for the complicated influenza course per patient was lower in the groups of patients treated with kagocel and pentanedioic acid imidazolyl ethanamide than in group 2 (p < 0.001 and p = 0,001, respectively). In addition, the patients receiving kagocel had a lower number of concomitant diseases than the patients in group 1, group 2, and group 4 (p = 0.002, p < 0.001, and p = 0.029, respectively). The mean number of different influenza symptoms per patient was lower in the group of patients receiving umifenovir than in group 1 (p < 0.001) and group 3 (p < 0.001). At the same time, significant differences in this parameter were observed between patients receiving kagocel and pentanedioic acid imidazolyl ethanamide (p = 0.010).
Results
Monitoring patients’ compliance with treatment
The analysis of patients’ compliance with treatment showed that most patients took the drug prescribed in accordance with the doctor’s instructions (84.47%, n = 1577). In 7.23% of cases (n = 135), it was found that patients violated the treatment regimen and withdrew the medication earlier than the specified period. In 6.70% of cases (n = 125), irregular administration of the medication or taking a lower dose of the medication was recorded. Complete refusal to take the medication prescribed was observed only in 1.61% (n = 30) of cases. A decrease in treatment compliance was recorded more often among patients receiving kagocel than among patients in group 1 (p = 0.012) and group 2 (p = 0.001).
Comparative assessment of the incidence of bacterial complications, adverse events, antibiotic treatment, and hospitalization
Statistical differences between the treatment groups were revealed for the following events: bacterial complications (in particular, from the ENT organs), bronchitis with productive cough, and pneumonia, as well as the prescribing antibacterial treatment (Table 2). Bacterial complications were observed in 18.87% (n = 335) of the patients examined. The most common nosology among all bacterial complications was bronchitis with productive cough (10.03%, n = 174). Bacterial complications from the ENT organs were observed in 7.09% of patients (n = 123). Bacterial pneumonia was observed much less often in the patients examined (2.38%, n = 42).
Comparative characteristics of the patient groups according to the incidence of bacterial complications, adverse events, prescribing antibacterial treatment, and hospitalization (count/%).

Pearson (chi-squared) test.
Two-sided Fisher’s exact test, pairwise comparisons of the groups are presented in symbolic notation.
Prescribing antibacterial treatment due to bacterial complications was required in 17.41% of the patients examined (n = 309). Exacerbation of concomitant diseases was observed in 2.14% of patients only (n = 37). A total of 1.24% of patients (n = 22) were hospitalized, of which 18 patients were hospitalized due to bacterial complications, two patients—with complications of concomitant diseases, and two patients—with severe influenza. There were no significant differences in the incidence of hospitalization between the treatment groups studied.
Adverse events were observed in 4.76% of patients (n = 84), of which complaints were due to symptoms of gastrointestinal tract disorder in the absolute majority of cases (91.67%, n = 77) and only in 8.33% of cases (n = 7) complaints were due to allergic reactions. Table 2 shows the incidence of the main types of adverse events in different patient groups. It was found that gastrointestinal complaints were significantly more common among patients receiving oseltamivir (8.21%) than among the patients in group 2 (2.56%, p < 0.001), group 3 (2.08%, p < 0.001), and group 4 (2.59%, p = 0.003). There were no other statistically significant differences between the groups.
Table 3 shows the characteristics of risk groups according to the incidence of bacterial complications and prescribing antibacterial treatment. Significant differences for all parameters studied were found between two patient groups, depending on the presence or absence of diabetes mellitus or obesity. Among patients with lung diseases, bronchitis with productive cough was observed much more often than among patients with influenza without a history of pulmonary diseases (16.82% vs 8.45%, p < 0.001).
Frequency of bacterial complications and antibiotic treatment in patients of different risk groups for severe/complicated influenza (count/%).

Pearson (chi-squared) test.
Two-sided Fisher’s exact test.
A multivariate analysis was performed to comparatively assess the effect of antiviral treatment on disease outcomes, considering additional risk factors. It was found that bacterial complications were more associated with influenza severity and treatment compliance (Figure 3). Thus, among patients with a moderate course of the disease, the chance of bacterial complications was 6.77 times higher (95% CI: 5.00–9.21, p < 0.001) than among patients with a mild course. In turn, non-compliance with the treatment regimen prescribed was also accompanied by a 2.65-fold increase in the chance of bacterial complications (95% CI: 1.90–3.68, p < 0.001).

Multivariate analysis of the relationship of demographic and clinical parameters with bacterial complications in patients with influenza.
Considering additional risk factors, the chances of bacterial complications from ENT organs and bronchitis with productive cough did not differ in the patient groups studied. Meanwhile, the chance of developing bacterial pneumonia among patients in group 4 was 3.26 times higher (95% CI: 1.44–7.72, p = 0.005) than among patients receiving oseltamivir. In turn, in group 2, there was a tendency to decrease the chance of developing bacterial pneumonia; however, this relationship was not statistically significant (p = 0.193).
The need for antibiotic therapy due to bacterial complications was largely associated with the disease severity and treatment compliance. Among patients with a moderate course of the disease, the chance of bacterial complications was 6.90 times higher (95% CI: 5.06–9.48, p < 0.001) than among patients with a mild course. A decrease in the patient’s treatment compliance was accompanied by an increase in the chance of prescribing antibacterial therapy by 2.15 times (95% CI: 1.53–3.01, p < 0.001). The chances of prescribing antibacterial therapy among patients in group 2 and group 3, adjusted for additional risk factors, did not differ significantly from the chances in group 1. Meanwhile, the chance of prescribing antibacterial therapy was 1.76 times higher (95% CI: 1.17–2.65, p = 0.006) in the group of patients receiving imidazolyl ethanamide pentanedioic acid than in the group of patients receiving oseltamivir.
The chance of adverse events among patients with a laboratory-confirmed diagnosis of influenza was 3.50 times higher (95% CI: 1.73–8.10, p = 0.001) than among the patients with a clinically established diagnosis (Figure 4). In addition, a 3.93-fold increase in the chance of adverse events (95% CI: 2.29–6.66, p < 0.001) was observed in the patients who did not follow the prescribed treatment regimen. Multivariate analysis confirmed statistically significant differences between the studied groups of patients in the incidence of adverse events. The chance of adverse events in the group of patients receiving oseltamivir was 2.44 times greater (95% CI: 1.28–5.00, p = 0.009) than in group 2, 4.76 times greater (95% CI: 2.44–10.00, p < 0.001) than in group 3 and 3.45 times greater (95% CI: 1.67–7.69, p = 0.002) than in group 4.

Multivariate analysis of the relationship of demographic and clinical parameters with adverse events in patients with influenza.
Comparative assessment of the disease duration
Analysis of the dynamics of the course of the disease at visits 2 and 3 showed that information about the date of complete clinical recovery was absent in 15.16% (n = 283) of patients. Among them, in 62.19% of cases (n = 176), the patient remained clinically ill at the time of the last study visit (visit 3), in 37.81% of cases (n = 107), contact with the patient was lost after visit 2, at which clinical manifestations of influenza persisted. There were no significant differences between the patient groups regarding the disease duration. The median duration of the disease was 8.00 days (6.00–9.00 days).
Discussion
Clinical guidelines for the treatment of influenza in adults include the possibility of using a number of antiviral drugs registered in the Russian Federation. Among the medications recommended for use in patients with influenza in outpatient practice, three drug products are most used: umifenovir (up to 25%–40% of the total number of prescriptions), imidazolyl ethanamide pentanedioic acid (up to 15%), kagocel (up to 15%), as well as oseltamivir as the “gold standard” of antiviral therapy. Assessing the impact of choosing an antiviral drug on the incidence of complications in patients at risk is an important task to improve the quality of outpatient medical care.
The treatment effectiveness for mild and moderate forms of influenza was assessed by the rate of complications in patients from risk groups. In patients receiving etiotropic therapy with umifenovir and oseltamivir, the incidence of bacterial pneumonia was the lowest in comparison with other studied medications. The highest incidence of complications was shown when using imidazolyl ethanamide pentanedioic acid, whose mechanism of action is associated with the activation of innate immunity factors, in particular by increasing the expression of the first type interferon receptor IFNAR. 17
The results obtained confirm WHO guidelines on the use of direct-acting antiviral agents to control the incidence of influenza. The use of host-response immune modulators is limited by the reactivity of the immune system, that is, the ability to activate interferon synthesis and the time to achieve effective concentrations in the blood. Thus, for the interferon inducer kagocel, the time to reach maximum concentrations of IFN in the blood is 48 h. 17 In turn, the duration of action for medications with a direct mechanism of action is determined by the achievement of maximum concentrations of the drug itself in the blood or its active metabolites, so for oseltamivir and umifenovir, the time of onset of action can be determined as 1–1.5 h and 2–3 h, respectively. 17 These differences in the mechanism and speed of action may explain the results obtained.
All the results of the multivariate data analysis described in the text of the article and the obtained significant effect sizes seem to the authors to be clinically significant and allow certain conclusions to be drawn regarding the characteristics of the course and treatment of influenza caused by modern seasonal strains in individuals from high-risk groups.
The second aspect investigated in the study is safety. The development of adverse events, primarily from the gastrointestinal tract, when using oseltamivir, is observed significantly more often than when prescribing other drugs. Thus, the optimal choice in the treatment for outpatient influenza patients at risk of complications is prescribing direct antiviral drugs (oseltamivir or umifenovir) in the first 36 h after the onset of the first symptoms of the disease. The results of our study allow us to recommend the use of these drugs for the treatment of outpatient influenza patients at risk of complications, regardless of the severity of the disease.
Evaluation of the cost-effectiveness of treatment was not the aim of this work; however, the obtained results indicate the advisability of conducting additional studies on comparative clinical and economic evaluation of various antiviral therapy regimens in patients with a high risk of severe/complicated influenza.
The main limitations of this study are the features of its design: an observational, non-interventional study without randomization, blinding, and control. Meanwhile, the current study included more than 2000 patients who were monitored by qualified research doctors at 11 clinical centers. The stages of observation and the criteria for evaluating the primary and secondary points of the study were clearly defined. To exclude confounding errors and influence on the results of important clinical indicators, for which stratification of therapy groups was not carried out, methods of multidimensional data analysis were used to evaluate the studied effects. This study was conducted in the context of real clinical practice and, in accordance with current clinical guidelines, all patients with influenza from risk groups were to receive antiviral therapy. In this regard, it was not possible to study the possible effects of different treatment regimens in comparison with the control or placebo. Undoubtedly, if the control group were included in the studies, one would have expected to receive a much larger number of adverse disease outcomes, which would have allowed a more accurate assessment of the differences in the effects of the treatment regimens under study.
All of the above allow, from our point of view, to consider the results obtained as reliable and reproducible in real clinical practice on the territory of the Russian Federation. In addition, the results obtained can be extrapolated to some neighboring countries, which apply similar standards for the diagnosis and treatment of influenza. Oseltamivir is used to treat influenza in many countries around the world, which allows us to extrapolate the relevant research results to a much larger target audience than patients living only in Russia. Umifenovir is also registered and available for use in some countries, such as China. In turn, Kagocel and imidazole ethanamide pentandioic acid, in addition to Russia, are available for clinical use in some countries, such as Belarus, Kazakhstan.
Conclusion
This study aimed to compare the effects of antiviral treatments for influenza on the incidence of bacterial complications. The results obtained confirm the relevance of direct-acting antiviral agents, namely oseltamivir and umifenovir, in managing influenza in high-risk patients, as reflected by their impact on bacterial complication rates and disease duration. These two agents may be recommended for the treatment of high-risk influenza patients.
Supplemental Material
sj-docx-1-tai-10.1177_20499361251347726 – Supplemental material for Antiviral therapy for influenza in high-risk outpatients: a multicenter observational study of routine clinical practice in Russia
Supplemental material, sj-docx-1-tai-10.1177_20499361251347726 for Antiviral therapy for influenza in high-risk outpatients: a multicenter observational study of routine clinical practice in Russia by Ivan Tokin, Dmitry Lioznov, Artem Poromov, Tatyana Zubkova, Valerii Tsvetkov, Olesya Nikitina, Olga Pobegalova, Natalia Pshenichnaya, Viktor Renev and Anastasiya Podgornaya in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.