
Abstract
Backgrounds:
Existing studies on the treatment of emergency infectious diseases have primarily focused on the pathogen and the human immune system. However, human health is intricately connected to environmental factors, and this interaction becomes particularly during large-scale public health emergencies. Few studies have examined the impact of spatial differences in the microenvironment on the rehabilitation rate of patients with the Omicron variant infection.
Objective:
This study employs causal inference statistical methods and spatial analysis to investigate how the hospital microenvironment affects the rehabilitation of COVID-19 patients in a mobile cabin hospital, so as to provide a scientific basis for the spatial arrangement of patients in mobile cabin hospitals.
Design:
Observational study.
Methods:
This study used the clinical information of 6291 patients admitted in a mobile cabin hospital in Shanghai, from April 9 to May 9, 2022, during the pandemic. Exploratory spatial data analysis and fixed-effects regression analysis were conducted to understand whether the microenvironment around the patients’ beds in the cabin impacted their rehabilitation.
Results:
The results indicate that the rehabilitation condition of patients is affected by spatial differences of microenvironment. Both the mean and minimum CT values of the surrounding patients show a significant positive correlation with the rehabilitation of patients. The further the distance from the vent is, the more the rehabilitation speed of the patients is affected by the CT values of the surrounding patients.
Conclusion:
These findings offer valuable insights for bed allocation, patients’ stratification and management, and ventilation management in the mobile cabin hospitals during public health emergencies.
Keywords
Introduction
Existing studies on the treatment of emergency infectious diseases were primarily focused on the pathogen and the human immune system. However, human health is intricately connected to the environment, and this interaction becomes prominent during large-scale public health emergencies. Therefore, it is crucial to study the hidden factors affecting the patients’ recovery and the dynamic interaction mechanisms between humans and the environment during such events. Air-transmissible pathogenic viruses pose a severe threat to public health and have already caused various pandemics worldwide such as Spanish influenza in 1918, Asian influenza in 1957, Severe acute respiratory syndrome coronavirus (SARS) in 2003, H1N1 influenza in 2009, and Middle East respiratory syndrome (MERS) in 2015.1–6 Airborne pathogens can spread widely and rapidly. Since the outbreak of the COVID-19 epidemic in December 2019, countries have faced the challenge of a significant increase in infection caused by the local outbreak of the epidemic. The sudden surge of patients has led to a shortage of beds in traditional hospitals, which has further intensified the COVID-19 threat. 7 Therefore, it is necessary to enforce strict quarantine measures to stop the spread of the COVID-19 epidemic. 8 To meet the sudden increase in medical demand and the requirements of isolation treatment, many makeshift hospitals have been constructed, which have played an essential role in treating patients infected with the novel coronavirus. China’s “Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia” (Ninth Trial Edition) has specifically pointed out that a centralized isolation management should be implemented for mild cases. 9
The World Health Organization recommends “cohort nursing” for large-scale outbreaks of infectious diseases such as influenza. 10 Cohort nursing involves grouping patients with the same infection and symptoms to confirm pathogens and provide medical care in isolated areas. 11 In cohort nursing, patients are generally placed in wards that have been already constructed. Mobile cabin hospitals are usually set up in large public facilities such as indoor stadiums, conference centers, or exhibition centers. When there are many patients and the available beds are insufficient, mobile cabin hospitals can be utilized as an alternative strategy for cohort nursing to control the rapid transmission of a disease. Mobile cabin hospitals were launched as a new public health project in Wuhan, China, in February 2020 in response to the COVID-19 epidemic. They have shown significant advantages in preventing and controlling highly infectious diseases and reducing the infection rate.12,13 The primary function of a mobile cabin hospital is to alleviate the challenge of the mass concentration of patients and the shortage of wards in the short term. Thus, such hospitals have become important facilities for providing medical treatment to COVID-19 patients, offering effective monitoring of asymptomatic or mildly infected patients, as well as the timely identification and treatment of those severely affected, ensuring better diagnosis and care. Unlike conventional isolated patient rooms, the patients in a mobile cabin hospital are located in large indoor spaces that maximize the healthcare efficiency of the medical staff. However, this open environment increases the risk of cross-infection among patients.
In the past few years, many studies have reported on the architectural features of mobile cabin hospitals and their effectiveness in controlling outbreaks.14–16 A few studies have also explored how the distribution and planning of hospitals relate to the control of epidemics from a spatial perspective. 17 However, limited attention has been given to the indoor spatial layout of mobile cabin hospitals. In addition, there is a deficit of research that combines the rehabilitation speed of patients with spatial planning. Previous studies have proposed the use of the circulation rate of hospital beds as an indicator to measure the hospital’s ability to operate safely and effectively. 18 However, when dealing with a pandemic with limited resources such as the number of beds and medical staff, the acceleration of nucleic acid negative conversion rate is essential to increase the circulation rate of beds in a mobile cabin hospital for admitting more patients within a short period. Several studies have confirmed that indoor air quality plays an important role in reducing the viral load. 19 The decrease in viral load benefits the acceleration of patients’ nucleic acid negative conversion rate. 20 Therefore, improving the circulation rate of hospital beds and microenvironment in mobile cabin hospitals will be of great significance during a pandemic.
This study employs statistical and spatial analyses to investigate how the hospital microenvironment affects the rehabilitation of patients in a mobile cabin hospital. We propose two hypotheses. First, the rehabilitation speed of patients is influenced by the microenvironment and exhibits spatial variation. Second, the severity of illness in surrounding patients has a significant effect on the rehabilitation of other patients. If these two hypotheses are confirmed, the results may provide valuable insights for the spatial planning of patients and hospital beds, improve the rehabilitation efficiency of patients in mobile cabin hospitals, as well as reduce the social and economic burden of isolation.
Methods
Study population
The study was an observational study and included clinical information of 6291 patients from the first floor of No. 4 cabin at a mobile cabin hospital set at the National Exhibition and Convention Center, Shanghai, from April 9 to May 9, 2022. As Shanghai’s largest mobile cabin hospital, the National Exhibition and Convention Center was designated to treat mild cases during the Omicron outbreak. In cases where a patient’s condition worsened, they were immediately transferred to another designated hospital for further treatment. Sample size is calculated in Supplemental Materials. Positive nucleic acid results were diagnosed according to the diagnosis and treatment protocol for COVID-19 (Trial version 9). 9 All patients were diagnosed based on CT-values (both ORF1ab and N genes). The CT values of nucleic acid detection were measured daily in a mobile cabin hospital. Patients who were not transferred to other hospitals were discharged after two negative nucleic acids. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Descriptive analysis
The information about 6291 patients, including their age, gender, and other attributes, was obtained and analyzed. The number of days of CT values to convert to negative and individual characteristics were analyzed using cross-tabulation to test for any significant differences between the groups.
Spatial analysis
The spatial distribution of hospital beds and the location of doors, doctors’ office, and nursing centers in the mobile cabin hospital were visualized using the ArcGIS software (Esri, 2020) (Figure 2). The medical records of the patients were attached to the respective beds. The door shown in Figure 2 is the only door that was continuously open in the cabin; the rest of the doors and windows were closed. The ventilation system was installed next to the door, which was the main channel of fresh-air inflow into the cabin. The distance from each bed to the door was calculated using the point distance tool of the ArcGIS software, which was used as a variable to test the effect of distance from ventilation on patient rehabilitation. The distance from the bed to the door in the cabin is a continuous variable. In this study, it was divided into three groups for fixed-effects regression analysis based on the lower and upper quartiles, namely 0–60 m as short distance, 61–120 m as medium distance, and over 121 m as long distance.
Considering the changes in the CT value with time, the change rate of the CT values of the O and N genes was used as a variable to measure the rehabilitation speed of patients turning negative. Hot spot analysis was carried out on the change rates of the O and N genes of all patients on April 15 to identify any spatial agglomeration of high and low values and to visualize the distribution of clusters with high and low values of the variables by ArcGIS. The Global Moran Index (see Supplemental Material) was used to determine the correlation of age, gender, number of vaccine injections, and chronic diseases in spatial distribution by Geoda software. The patients’ age, gender, number of vaccinations, and chronic diseases were analyzed by the Global Moran Index to check for any correlation with the spatial distribution of patients.
Fixed-effects regression analysis: The CT values of the O and N genes change with time. Regular regression analysis cannot effectively control for the change in time and individual characteristics. Therefore, the two-way fixed effects (individual fixed effects and time fixed effects) method was used to study the influence of the mean and minimum CT values of surrounding patients in the cabin on the CT value of a patient. Specifically, the individual fixed effects were used to control for the time-invariant individual factors that do not change during patients’ hospitalization, such as age, gender, physical immunity, and other individual factors, while the day fixed effects were used to control for the influencing factors of all patients in the cabin (shared effect), such as the consistent management measures and the same environmental factors for each patient in the cabin. The following model was used to estimate the CT value Y of individual i at time t by ordinary least square:

where
Results
Descriptive analysis
This study included clinical information of 6291 patients from the first floor of No. 4 cabin at a mobile cabin hospital set at the National Exhibition and Convention Center, Shanghai, from April 9 to May 9, 2022. The data showed that COVID-19 patients were hospitalized for an average period of 8 days; the last 3 days comprised the observation period. Therefore, the 5-day period was taken as the panel for data analysis. As the first group of patients admitted to the mobile cabin hospital began to be discharged after April 15, the peak period of hospitalization in mobile cabin hospitals, that is, from April 22 to April 28, was selected for the analysis to include as many inpatients as possible in three panels. The panel data of April 22–26, April 23–27, and April 24–28 were utilized for sliding window analysis to analyze and verify the results (Figure 1). It shows the daily change in the number of patients staying in and leaving the mobile cabin hospital. The blue line refers to the total number of patients on that day, and the red line refers to the number of patients increased or decreased on that day.

Daily change in the number of inpatients in a mobile cabin hospital.
The average rehabilitation period varies significantly based on the age group, vaccine number of patients, and whether they have chronic diseases. The rehabilitation of patients aged 60 years and older took an average of 5.932 days, while that of unvaccinated patients took an average of 5.637 days. These values are greater than those of other age groups and vaccinated patients. In addition, the average number of days for rehabilitation is 5.3 for patients without chronic diseases and 5.793 for patients with chronic diseases. The average number of days for rehabilitation does not show significant gender differences in this study (see Supplemental Material Table 2).
Exploratory spatial data analysis
A spatial autocorrelation analysis of the change rate of CT values for the O and N genes was conducted. The results showed that the Global Moran Index values of the change rate of the O and N genes were 0.1154 and 0.1147, respectively, which imply that the change rates of these two genes showed a certain spatial autocorrelation among the inpatients on April 15. The results of the change rate of the CT values of the O gene are listed in Figure 2 (see the results for the N gene in Supplemental Material Figure 1). Hot spot analysis is used to display the regions with high and low values. Red represents high values or hot spots, while blue represents low values or cold spots. Patients with a faster rehabilitation rate (red beds; Figure 2) are spatially aggregated beside the channel to the only vent of the cabin. To verify hypothesis 1, a spatial autocorrelation analysis and a fixed effects analysis were conducted. The results of the spatial autocorrelation analysis showed that the values of Moran’s I for age, vaccine injections, and chronic diseases are all <0.1, implying a random distribution of patients based on the three attributes. The value of Moran’s I for gender is 0.316, which implies that male or female inpatients are spatially clustered. However, the cross-tabulation analysis results showed that the gender has no significant difference in the number of rehabilitation days. Therefore, the individual attributes do not have a significant impact on the spatial agglomeration of the change rate in the CT values of inpatients.
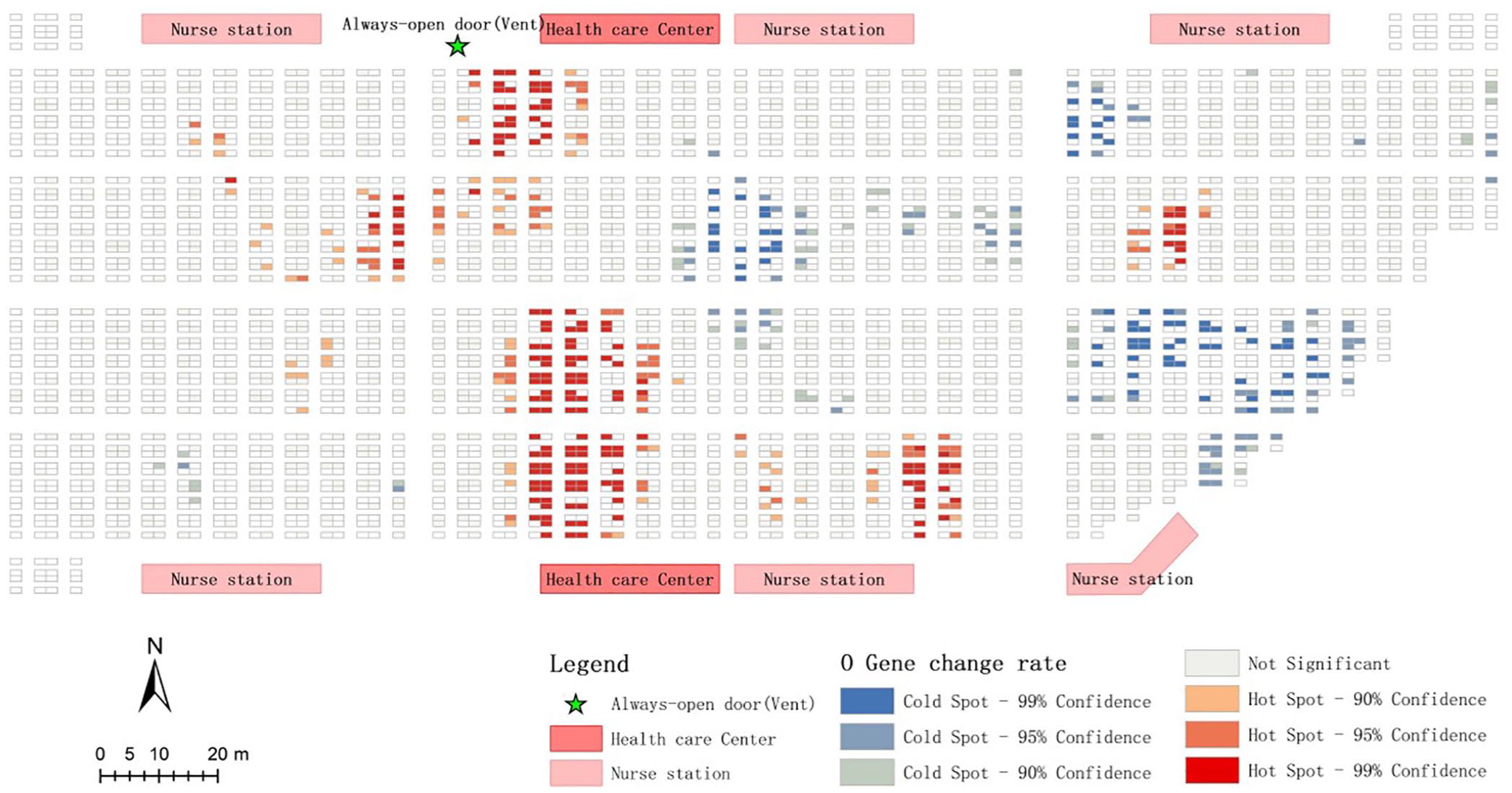
Hot spot map of the change rate of CT values of the O gene of inpatients on April 15. A hot spot represents a high-value cluster, and a cold spot represents a low-value cluster.
Fixed-effects regression analysis
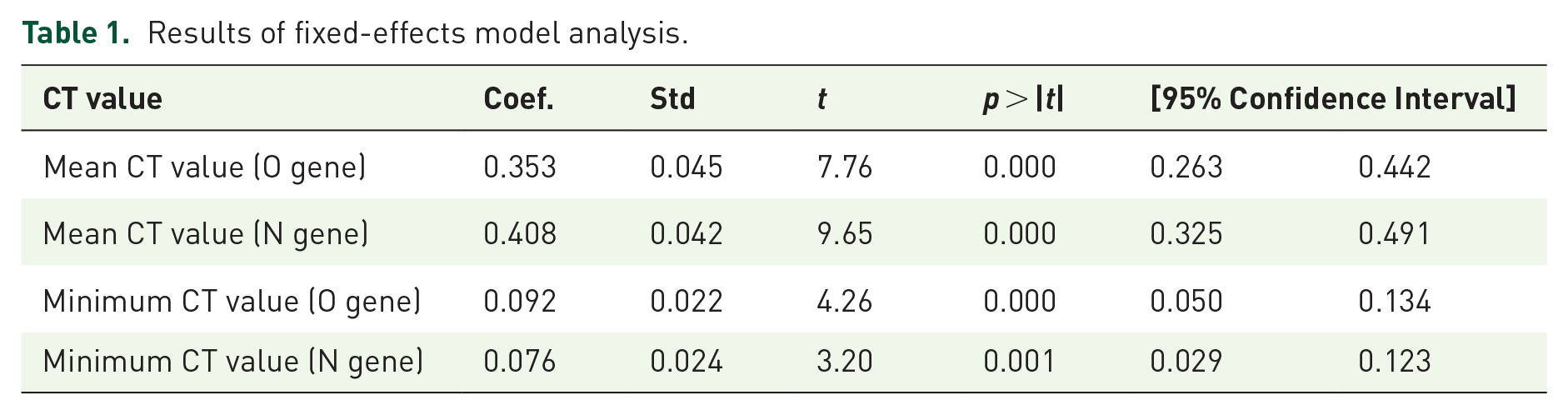
The results of fixed-effects regression analysis showed a significant positive correlation between the mean CT value of the surrounding patients in the cabin and the CT value of a patient (Table 1). When the mean CT value of the surrounding patients is high, the CT value of the patient increases and the viral load decreases, and vice versa. The minimum CT value of the surrounding patients has a significant positive correlation with the CT value of the patient. When the minimum CT value of the surrounding patients is small, it implies that the condition of the patient has become more serious and his/her CT value has become smaller. Similar results were obtained when the N gene was analyzed as the dependent variable.
Results of fixed-effects model analysis.
The interactive fixed effects were analyzed to test whether the distance from the vent impacts the rehabilitation of patients. The O and N genes were analyzed, and the same pattern was obtained (Table 2 and Supplemental Material Table 3). In Table 2, for the O gene, when the distance between the patient’s location and the vent was 0–60, 61–120, and over 120 m, the coefficient for the influence of the CT value of surrounding patients was 0.499, 0.538, and 0.543, respectively.
Interactive CT value cross-fixed-effects model analysis results (O gene).
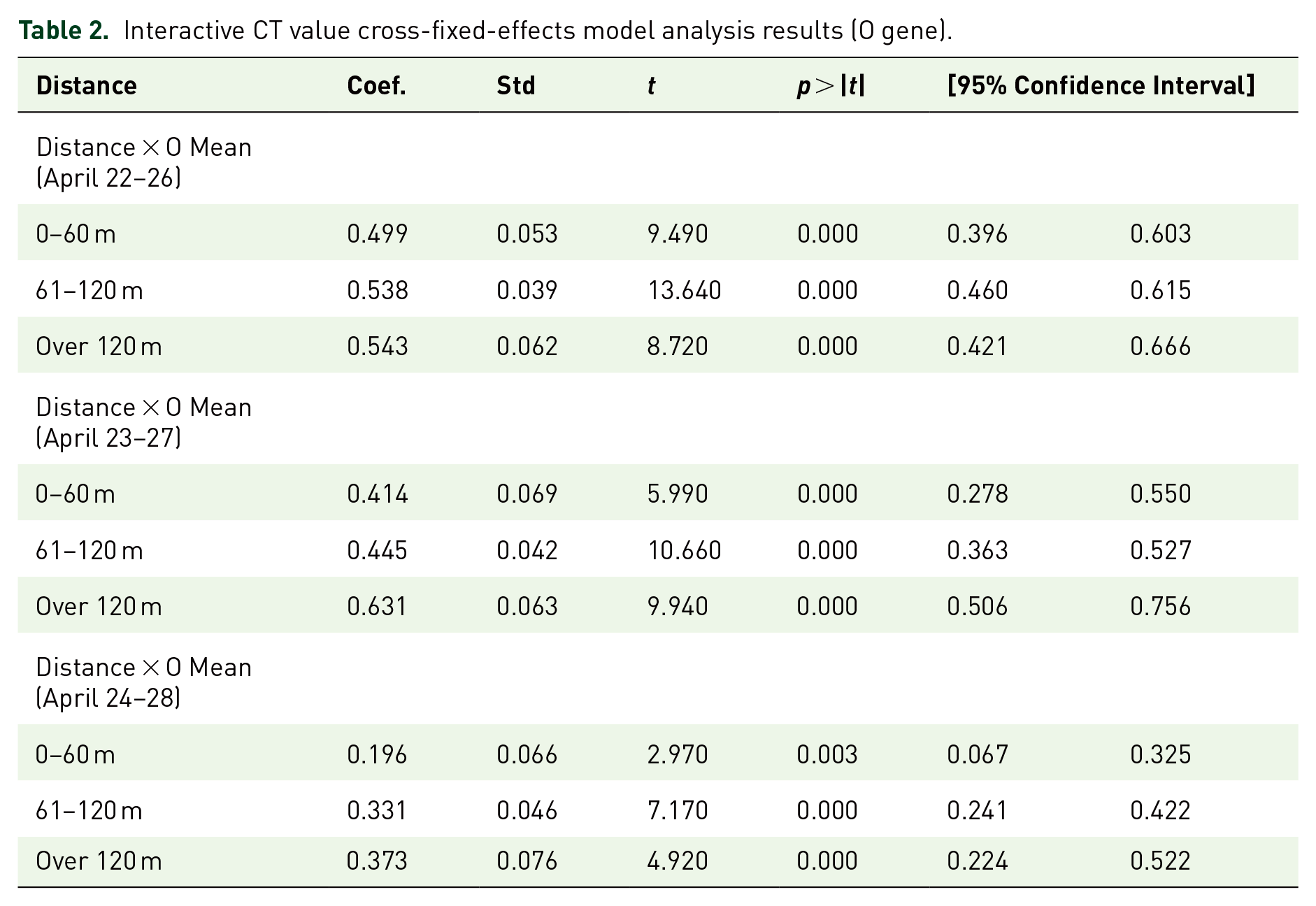
The results showed a spatial difference in the degree to which the CT values of patients are affected by those of the surrounding patients. When patients are closer to the ventilation system, their CT values are less affected by the surrounding patients, and vice versa. Figure 3 shows that the slope increases with an increase in distance between hospital beds and the vent, that is, as the distance from the vent increases, the influence of the mean CT values of the surrounding patients on the CT values of the patients also increases.

Margin plot diagram of interactive fixed effects. The blue line represents the impact of changes in CT values around patients on patients 0–60 m away from the vent. The red line represents the impact of changes in CT values around the patient when the distance from the vent is 61–120 m. The green line represents the extent to which changes in CT values around the patient affect the patient when the distance from the vent exceeds 120 m.
Discussion
This study utilizes patient data from a mobile cabin hospital set up at the National Exhibition and Convention Center in Shanghai to analyze whether the microenvironment around a patient bed has an impact on the rehabilitation of the surrounding patients. To the best of our knowledge, no prior study has analyzed the correlation between the rate of change in CT values of COVID-19 patients and the allocation of hospital beds. The findings of this study will provide evidence for improving the spatial planning of patient allocation and the optimization of the cabin microenvironment.
The results confirm the spatial heterogeneity and autocorrelation of patient rehabilitation in the microenvironment when the patients are randomly distributed in terms of age, number of vaccines, and whether have chronic diseases.21,22 The spatial exploratory analysis found that the change rate of the CT values of patients shows spatial agglomeration and a spatial proximity relationship exists between the areas with a higher change rate for CT values and cabin vents. Hence, hypothesis 1 is verified. The results of the fixed-effects analysis show that there is a significant positive correlation between the CT value of the patient and the mean CT values, as well as the minimum CT value of the surrounding patients. Hence, hypothesis 2 is verified. When further considering the impact of the microenvironment on patient rehabilitation, it was observed that the farther away a patient is from the vent, the greater is the influence of the mean CT values of the surrounding patients on the patient’s CT value. Hence, hypothesis 1 is verified again.
Previous studies have shown that at the macro level, there is a significant spatial association in the early stages of the COVID-19 epidemic, highlighting the critical role of spatial analysis in studying the spread of infectious diseases. 23 A previous study conducted a spatial autocorrelation analysis and showed that in China, the SARS-CoV-2 infection was spatially dependent and mainly spread from Hubei Province in Central China to the surrounding areas. 24 A study from Brazil used spatial and temporal trend analyses to demonstrate spatial autocorrelation in metropolitan areas. It also identified the spatiotemporal clusters of 11 COVID-19 cases. 25
A study conducted spatial analysis and showed that at the micro level, the confirmed cases of COVID-19 are related to the distribution of intensive care beds specifically for the disease. This helps in determining the priority areas of care for containing and controlling the disease. 26 The spatial autocorrelation analysis of gender, age, number of vaccination shots, and chronic diseases is conducted to verify whether the spatial agglomeration is a result of individual attributes. The results show that the patients were randomly distributed in space, which indicates that the spatial agglomeration of the change rate of the CT values of COVID-19 patients is not caused by individual factors.
Previous studies have emphasized the critical role of fresh air in removing exhaled virus-carrying air. 27 Ventilation can effectively avoid the recycling of polluted air, keep the indoor aerosol concentration as low as possible, and reduce the viral load concentration in the air. Ventilation improvements can help control airborne infections. A major way to reduce an individual’s infected susceptibility in a confined space is to increase the air-dilution rate. 28 Several studies have investigated the relationship between ventilation rates in laboratory-like offices and the health and performance of the occupants. The findings show that increasing the supply of fresh air to any indoor space is an effective strategy for reducing airborne transmission, 29 which has similar or even better control effects than isolation and vaccination. 30 A study also showed that increasing the fresh-air supply rate in trains can significantly reduce the risk of airborne transmission of COVID-19. 31 Hence, the rehabilitation rate of patients in mobile cabin hospitals varies with ventilation conditions. Appropriate fresh-air ventilation and outdoor air exchange rates help mitigate the spread of the virus.32,33
Hence, the spatial allocation of patients should take their CT values into account. In addition, the surrounding environment is particularly important for the rehabilitation of patients. Among all age groups, the rehabilitation time period is the longest for old and young patients, and therefore, these two groups of patients need care resources the most. Special zones should be planned for old and young patients to provide them with better care and to alleviate the challenge of shortages in medical staff. At present, the existing plan places both old- and young-patient zones farthest away from the vent at the corner of the cabin. However, this study has shown that the patients’ CT values are more affected by the mean and minimum CT values of the surrounding patients when the distance from the vent increases. In contrast, the CT value of patients in the area closer to the vent is least affected by the mean and minimum CT values of the surrounding patients. Hence, old and young patients should be allocated beds closer to the vent and the distance between their beds should be increased to effectively reduce the negative cross-impact and improve their rehabilitation. It is also of great significance to improve the monitoring of the cabin environment and carry out regular disinfections of the cabin, especially at the dead corners with poor ventilation. Based on our research findings, we propose the following recommendations for optimizing the ventilation system in cabin hospitals: Optimization of Vent Location and Quantity: Ventilation vents should be strategically positioned within the cabin hospital to ensure adequate fresh air circulation for each bed. The use of airflow simulation models can help determine the optimal placement and number of vents; Implementation of Air Filtration and Purification Systems: It is recommended to install high-efficiency air filtration and purification systems in the cabin hospital to reduce the spread of pathogens in the air and improve air quality; Establishment of a Real-Time Monitoring System: A real-time monitoring system should be established to provide continuous feedback on the effectiveness of ventilation. This system should allow for dynamic adjustments to meet the varying needs of different patients.
This study has some limitations as well. First, no monitoring data were obtained for factors such as temperature, humidity, and aerosol in the cabin. Instead, the distance from the bed to the vent and the door was taken as an independent variable to measure the microenvironment. We plan to introduce temperature and humidity measurements in subsequent studies to more fully analyze the impact of environmental factors on the results. Aerosol concentrations are monitored using specialized instruments to assess their potential impact on the microenvironment and study results. We will investigate the effect of improving the measurement of the rehabilitation rate in a future study. Second, failure to include laboratory tests and to adequately explore the contribution of management/treatment measures to patient outcomes. To address this issue, future studies should incorporate information such as laboratory tests and analyze the management and treatment measures patients receive to more accurately assess their impact on prognosis.
Conclusion
To summarize, the results from the clinical data of 6291 patients in this study indicate that the microenvironment of mobile cabin hospitals has a significant impact on the rehabilitation condition of patients and spatial differences exist. The mean and minimum CT values of the surrounding patients have a significant positive correlation with the rehabilitation of patients. The further the distance from the vent is, the more the rehabilitation speed of the patients is affected by the CT values of the surrounding patients.
Based on the results obtained, the following recommendations are provided for the construction of mobile cabin hospitals. First, the ventilation system should be enhanced and the number of vents appropriately increased to reduce viral load and facilitate patient rehabilitation. Second, patients’ CT values should be considered when allocating patients to optimize bed distribution, reduce cross-infection, accelerate bed turnover, and improve the utilization efficiency of mobile cabin hospitals. Third, a dedicated zone for elderly and young patients should be established near the vents and entrances, with increased spacing between beds to further reduce infection risks.
We believe that this spatial epidemiological study of COVID-19 will assist in the planning of mobile cabin hospitals, particularly in the allocation of zones for elderly and young patients, and provide scientific evidence for policy-making. Additionally, it will serve as a reference for the construction of mobile cabin hospitals for managing other respiratory infectious diseases in the future.
Supplemental Material
sj-doc-2-tai-10.1177_20499361241293668 – Supplemental material for The hidden factor in COVID-19 rehabilitation: how does the microenvironment in mobile cabin hospitals impact patient recovery? An observational study
Supplemental material, sj-doc-2-tai-10.1177_20499361241293668 for The hidden factor in COVID-19 rehabilitation: how does the microenvironment in mobile cabin hospitals impact patient recovery? An observational study by Yang Cheng, Ru Wen, Yuxiao Wang, Xinxin Sun, Shan Jiang, Zhiqiang Chen, Qiwei Yu, Liang Tan, Liqiang Zhang, Zhuolin Tao, Peng Xu, Dongdong Chen, Hong Yu, Zuqiang Su, Kang Chen, Yunsheng Liu and Chen Liu in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-1-tai-10.1177_20499361241293668 – Supplemental material for The hidden factor in COVID-19 rehabilitation: how does the microenvironment in mobile cabin hospitals impact patient recovery? An observational study
Supplemental material, sj-docx-1-tai-10.1177_20499361241293668 for The hidden factor in COVID-19 rehabilitation: how does the microenvironment in mobile cabin hospitals impact patient recovery? An observational study by Yang Cheng, Ru Wen, Yuxiao Wang, Xinxin Sun, Shan Jiang, Zhiqiang Chen, Qiwei Yu, Liang Tan, Liqiang Zhang, Zhuolin Tao, Peng Xu, Dongdong Chen, Hong Yu, Zuqiang Su, Kang Chen, Yunsheng Liu and Chen Liu in Therapeutic Advances in Infectious Disease