Group B Streptococcus Colonization and Vaccine Acceptance Among Pregnant Women in Rio de Janeiro, Brazil
André Rio-Tinto1, Natália Silva Costa1, Isabella Pinto1, Laura Oliveira1, Sergio Fracalanzza1, Lucia Teixeira1, Penelope Marinho2, Joffre Amim Jr1, Stephen Taylor3, Stephen Thomas3 and Tatiana Pinto1
1Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio Janeiro, Rio de Janeiro-RJ, Brazil, 2Maternidade Escola, Universidade Federal do Rio Janeiro, Rio de Janeiro-RJ, Brazil, 3UK Health Security Agency, UK
Introduction: Group B Streptococcus (GBS) is a recognized leading cause of perinatal diseases and can be found in the anovaginal microbiota of pregnant women, representing the main source for vertical transmission to newborns. The development of a vaccine against GBS to prevent vertical transmission and infection is already in place; however, vaccination coverage has decreased in recent years, due to several anti-vaccination movements that have emerged globally, including Brazil.
Objectives: Our aim was to assess the acceptance to a future GBS vaccine and current recommended vaccines coverage along with GBS colonization rates among pregnant women attending a single maternity in Rio de Janeiro, Brazil, between January 2021 and December 2022.
Methods: Anovaginal samples were streaked onto chromogenic media and blood agar after a pre-enrichment step, and colonies were identified by MALDI-TOF MS. GBS serotypes were determined by latex agglutination. The participants filled out a questionnaire to obtain sociodemographic data.
Results: Overall, 701 pregnant women participated, and 60 were positive for GBS (8.6%). Serotypes V (31.7%), Ia (16.7%) and III (15%) were the most prevalent, respectively. Only 11.9% of pregnant women were familiar with GBS and its danger. However, 71.6% participants would accept being vaccinated for GBS. For women who would accept taking the GBS vaccine we established the following profile: 30-year-old single brown women with high school education who took at least three of the four currently recommended vaccines.
Conclusion: In conclusion, despite reduced rates of adhesion to some vaccines in Brazil, such as measles and polio for children and dTpa for pregnant women, our results suggest a good acceptance of GBS vaccine in the near future in the population analyzed. Nonetheless, a broader spectrum of pregnant women would be necessary to further support this data in Brazil.
Funding
This work was supported by the Bacterial Vaccines (BactiVac) Network (funding number is BVNCP4-10); and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES)—Finance code 001, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) (funding numbers are E-26/211.554/2019 and E-26/010.002141/2019).
Benzylpenicillin pharmacokinetics in pregnant women during labour
Bonniface Obura1, Catriona Waitt1,2, William Hope1, Shampa Das1 and Kate Navaratnam3,4
1Department of Pharmacology and Therapeutics, University of Liverpool, Liverpool, UK, 2Infectious Diseases Institute, Makerere University College of Health Sciences, Kampala, Uganda, 3Fetal Medicine Unit, Liverpool Women’s Hospital, Liverpool, UK, 4Harris-Wellbeing Research Centre, University of Liverpool, Liverpool, UK
Background: Group B Streptococcus (GBS) is a leading cause of severe early onset neonatal sepsis (EOS). The incidence of early-onset GBS disease is on the rise in the UK, standing at 0.57 per 1000 live births. The Royal College of Obstetricians and Gynaecologists (RCOG) recommends a risk-factor based management with intrapartum antibiotic prophylaxis using intravenous benzylpenicillin. A loading dose of 3 g is advised, followed by 1.5 g every 4 h until delivery. Benzylpenicillin exhibits time-dependent activity – the fraction of time that free drug concentration is above the minimum inhibitory concentration (%fT > MIC) of bacteria correlates well with its antibacterial activity. Physiological changes during pregnancy may alter the pharmacokinetics (PK) of intrapartum benzylpenicillin resulting in unpredictable changes in free drug concentration and %fT > MIC. We assessed the pharmacokinetics of intrapartum benzylpenicillin administered by bolus doses.
Methods: A prospective cohort study was conducted at Liverpool Women’s Hospital. Pregnant women eligible for intrapartum benzylpenicillin, according to RCOG criteria were enrolled. Baseline demographic characteristics, medical and obstetric history were recorded. Benzylpenicillin was administered as intermittent intravenous boluses, 3 g loading dose at onset of labour and 1.5 g every 4 h until delivery. 3 ml blood samples were obtained at 0, 0.25, 0.5, 1, 2 and 4 h post initial dose. Benzylpenicillin Plasma concentrations were quantified using an ultra-high pressure liquid chromatography system coupled to a triple-quadrupole mass spectrometer; lower limit of detection was 0.1 mg/L. Pharmacokinetic parameters were estimated using noncompartmental analysis.
Results: In total, 12 participants were included in the study and 46 maternal PK samples obtained. The median (range) maternal age and weight were 30.5 (19–37) years and 75 (52–132) kg respectively. The peak plasma concentration of benzylpenicillin ranged from 31 mg/L to 112 mg/L with a mean (±SD) of 75.71 ± 24.02 mg/L. Average area under the concentration-time curve (AUC0-inf) was 87.88 ± 27.41 mg/L*h. The plasma elimination half-life was 0.54 h.
Conclusion: Intrapartum benzylpenicillin concentration-time profile exhibits the typical biphasic distribution with a rapid phase followed by a slow elimination phase. Plasma clearance is comparable to previously reported results in healthy non-pregnant population.
Routine GBS testing via GBS3 trial: uptake and associated issues in a large maternity unit
Emma Pugh
Obstetrics and Gynaecology Research Department, University Hospital of Wales, Cardiff, UK
Background: GBS bacteria is common, transient and usually harmless. GBS-exposed babies may develop early-onset GBS infection, causing short and long-term morbidity and rarely mortality. Risks to neonates can be negated by testing women and administering intrapartum antibiotics to positive cases. The UK National Screening Committee recommended a randomised controlled trial to determine the clinical and cost effectiveness of routine testing. The GBS3 trial randomised 71 UK hospitals to antenatal culture or intrapartum PCR testing or routine risk-based strategy for GBS testing, to assess the impact on neonatal sepsis. Our hospital (Cardiff) was randomised to antenatal culture testing.
Methods: GBS testing became standardised practice for the duration of the GBS3 trial. Women were given information at 28 weeks and offered the swab from 35 weeks, or earlier if early birth was expected. Trained staff could provide information and send swabs. Women could self-swab and verbal consent was sufficient. Research midwives provided GBS3 training to clinical staff to provide information to women, send swabs and relay positive results to women. If positive women were offered intrapartum antibiotics, immediate augmentation with non-labouring SROM and neonatal observation.
Results: The initial expected testing rate was 80% of all eligible women, dropping to 50% as many antenatal testing sites struggled to achieve 80%. Local rates increased and remained between 40 and 50% (Figure 1), similar to other antenatal testing sites. Women were interested and positive towards GBS testing and understood the importance. Despite introduction of routine standardised testing, rates have fallen short of expectation. Various issues contributed, particularly when routine testing was first introduced.
Percentage of eligible women who had an antenatal culture GBS swab during each month of the GBS3 trial in Cardiff.
Contributing factors:
1. Disseminating information and training to high staff numbers, working different shift patterns, different locations, being unable to check emails or social media regularly.
2. Women not being offered the test, possibly due to staff shortages, staff not attending training, forgetting, no translation services, lack of time, lack of confidence, high annual leave rates (lower figure in December), staff thinking the swab was an optional additional test linked to research.
3. Women declining swabs, mainly due to planned caesarean or already testing positive in this/previous pregnancy.
4. Swabs being requested or labelled incorrectly therefore not processed in the labs correctly.
Additional issues include some women being unreceptive to the rectal swab. Women not informed of positive results or its implications. Also it was difficult to monitor which women had or hadn’t been offered the test or who had declined, possibly influenced by the lack of electronic notes and opt-out of research system at site.
Conclusion: Generally women were positive and accepting of GBS testing. However, practical issues resulted only 40-50% of women having a swab. Embedding and standardising new practice takes time and clinical improvements are needed if routine testing were to be implemented.
Group B Streptococcus colonization among pregnant women, sero-prevalence and transplacental transfer of serotype-specific IgG antibodies in Ghana and Zimbabwe
Irene Apewe Adjei1,2, Zivai Mupambireyi3, Sarah White4, Edward Matsikire3, Alex Manu4, Nisha Dhar5, Louisa Iddrisu1, Elizabeth Mathias4, Sam Newton2, Luis Cuevas4, Oscar Agyei1, Andrew Carey4, Yeetey Enuameh2, Jones Opoku-Mensah1, Matthew Mathias4, Frances Cowan3,4, Kwaku Poku Asante1 and Gaurav Kwatra5,6
1Kintampo Health Research Centre, Kintampo, Ghana, 2Kwame Nkrumah University of Science and Technology, Ghana, 3Centre for Sexual Health and HIV/AIDS Research, Harare, Zimbabwe, 4Liverpool School of Tropical Medicine, Liverpool, UK, 5University of the Witwatersrand Vaccines and Infectious Diseases Analytics, Johannesburg, South Africa, 6Laboratory for Specialized Clinical Studies, Division of Infectious Diseases Cincinnati Children’s Hospital Medical Center, USA
Background: Group B Streptococcus (GBS) disease in infants’ manifest as sepsis, pneumonia, meningitis and could also leads to neonatal encephalopathy, preterm and stillbirths. Maternal rectovaginal GBS colonization at delivery is the major risk for GBS invasive disease in newborns. This study aimed to determine the prevalence of GBS colonization, sero-prevalence and transplacental transfer of GBS serotype-specific Immunoglobulin G antibodies.
Methods: The study was a multi-country population-based cohort study carried out at the Kintampo Health Research Centre (KHRC) in Kintampo, Ghana and the Centre for Sexual Health and HIV/AIDS Research (CeSHHAR) in Harare, Zimbabwe among pregnant women. Recto-vaginal swabs and blood samples were collected from study participants after 36 weeks gestation or at the time of delivery preferably before rapture of membranes. Chest aspirates and blood were collected from stillbirths and invasive disease cases. Swabs and blood specimens were cultured using standard culture methods for GBS and serotyping was performed by the latex agglutination. Serum GBS CPS specific IgG was analysed using a multiplex Luminex platform.
Results: A total of 1,238 women were enrolled. Overall prevalence of colonization was 15.4% (95%CI 15.4%-18.2%). The prevalence was similar in Ghana (15.6%) and Zimbabwe (15.2%). Serotype III (32%), serotype V (27%) and serotype Ia (25%) were the most prevalent serotypes in both countries accounting for 84% of the serotypes. High titres of IgG antibodies were reported in Ghana for serotype II (0.24) compared Zimbabwe (p = 0.06). Of nine stillbirth cases where chest aspirates were collected, three (33.3%) cultured GBS.
Conclusion: Our study reported low prevalence of GBS colonization among Ghana and Zimbabwean pregnant women compared to other studies in both countries. Studies focusing on targeted investigation of stillbirth would be needed to ascertain GBS as cause of stillbirth in these populations. GBS hexavalent vaccine covering serotype I-V could provide protection for the 97.3% GBS serotypes identified in the study.
Distribution of CRISPR elements in Group B Streptococcus belonging to the main lineages circulating in human population for over 10 years
Leandro Correa Simoes1, Laura Maria Andrade Oliveira1, Natalia Silva Costa1, Ana Caroline Nunes Botelho1, Sergio Eduardo Longo Fracalanzza1, Lucia Martins Teixeira1 and Tatiana Castro Abreu Pinto1
1Paulo de Goes Microbiology Institute, Federal University of Rio de Janeiro, Brazil
Background & objective: Group B Streptococcus (GBS) is a recognized cause of perinatal infections, being detected in around 1 of each 4 women as colonizers of the genitourinary and/or gastrointestinal tracts. GBS population is composed by several lineages that can differ in virulence and antimicrobial resistance potential. Typing techniques can allow us to better understand the relationships established between these lineages and its prevalence. Yet, alternative typing methods can demonstrate better discriminatory potential and lead to results in less time. CRISPR elements and their associated proteins (Cas) were originally described as an adaptive immunity mechanism found in bacteria. However, its ubiquity in some species and evolutionary relationships has led it to be applied for typing purposes as well. Here, we sought to better understand the distribution and composition of CRISPR elements in a diverse GBS population belonging to the main lineages circulating in human population.
Design: Seventy-eight carriage strains (anovaginal specimens) were recovered between 2008 and 2020 from pregnant women in Rio de Janeiro, Brazil. The following lineages were identified: Sequence Type (ST) 1 (n = 17), ST17 (n = 9), ST19 (n = 12) and ST23 (n = 40).
Methods: The whole genomes of the GBS isolates previously sequenced were submitted to CRISPRCasFinder online to identify CRISPR spacers and Cas proteins.
Results: All strains harbored CRISPR1 locus (Cas-Type II-A) and it was the only found. Overall, between 3 and 28 spacers were found. In ST1 strains, between 4 and 28 spacers were found, with 12 patterns being detected; ST17 had between 4 and 10 spacers and 4 patterns. In ST19 strains, from 14 to 28 spacers and 8 patterns were found. ST23 had 3 to 28 spacers and 17 patterns were detected.
Conclusion: The finding of the CRISPR1 locus in all strains corroborates data previously described in the literature, demonstrating its ubiquity and prevalence in the vaginal GBS population, which indicates its potential for typing. A wider range of spacers and patterns can indicate greater heterogeneity within a population, which may be associated with greater occurrence of genetic exchange involving mobile genetic elements. Still, ST17 strains had the lowest diversity among all analyzed lineages and are associated with neonatal meningitis development. This finding may indicate that greater homogeneity can be associated with bigger potential to cause disease. Data indicate the potential of CRISPR elements as an alternative strain typing technique for GBS strains circulating in human population, which can contribute to GBS disease surveillance.
A 7-year review of neonatal GBS cases at East and North Hertfordshire NHS Trust: Could early detection of GBS and risk factors lead to effective prevention?
Thidar Myint1, Jude Antonieo Balraj1, Sarah Prentice2, Maxine Feldman1, Rabia Zill-E-Huma1 and Lyn Ventilacion1
1Lister Hospital, East and North Hertfordshire NHS Trust, UK, 2London School of Hygiene and Tropical Medicine, UK
Background & objective: Group B Streptococcus infection remains the leading cause of neonatal invasive bacterial infection (iGBS) with the potential to cause long-term disability. Intrapartum prophylactic antibiotic (IAP) diminishes the risk of vertical transmission from a GBS carrier mother to neonate. However, GBS screening is not routinely offered to all pregnant women in the UK. This study aims to identify potential risk factors and areas of improvement to decrease the risk of GBS infection. We participated in the routine intrapartum testing arm of the GBS3 trial from Aug 2022 to March 2024.
Methods: A retrospective analysis was conducted of neonatal GBS cases between January 2017 and January 2024 by reviewing maternal and neonatal case notes and Badgernet electronic databases.
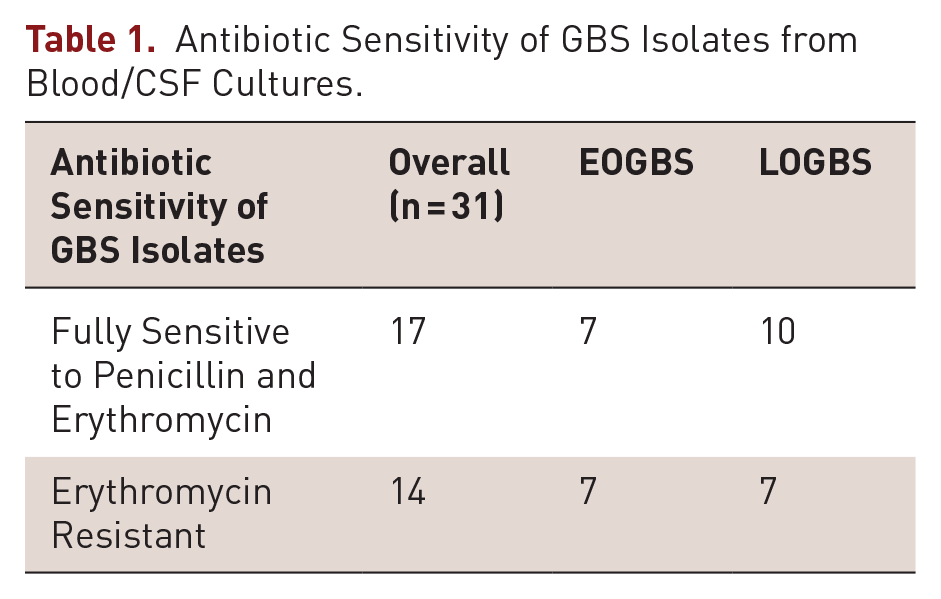
Results: 31 cases of neonatal GBS infection were identified, of which 45% (14/31) were early-onset (EOGBS) and 55% (17/31) were late-onset GBS sepsis (LOGBS) (Figure 1). GBS bacteraemia was common and all cases of GBS meningitis (16%, 5/31) were seen in the late-onset GBS sepsis cohort. 58% (18/31) of the cohort were male infants. The gestational ages of births were between 29+3 and 40+4 with 32% (10/31) of the cases being <37-week-old preterm babies. The birth weight of preterm babies (<37 weeks) ranged from 1200 to 3200 grams, while birth weight of term babies was 2628-3976 grams. 42% (13/31) of deliveries were spontaneous vaginal deliveries, while intervention was seen in 58% (18/31), which can be subdivided into instrumental deliveries 10% (3/31), elective c-sections 3% (1/31) and emergency c-sections 45% (14/31). Patients with early-onset GBS sepsis received 7–14 days of intravenous benzylpenicillin, and cases with meningitis completed a total 21 days of appropriate antibiotic therapy according to the antibiotic sensitivity from the blood/CSF cultures (Table 1).
Incidence of early onset and late onset GBS sepsis from Jan 2017 to Jan 2024.
Antibiotic Sensitivity of GBS Isolates from Blood/CSF Cultures.
Antibiotic Sensitivity of GBS Isolates
Overall (n = 31)
EOGBS
LOGBS
Fully Sensitive to Penicillin and Erythromycin
17
7
10
Erythromycin Resistant
14
7
7
In this study, we have also reviewed if there are any maternal clinical risk factors that would increase the risk of GBS sepsis among these cases. None of the mothers were known to have GBS before delivery, but only five mothers had a vaginal swab pre-delivery. 9 women had prolonged rupture of membranes (PROM), 5 of whom received broad-spectrum antibiotics for suspected chorioamnionitis or pyrexia of >38C in labour, and 3 women were found to have had histologic evidence of GBS after delivery.
Overall, positive GBS maternal results from blood culture, vaginal and placental swab were present in 25% of cases. Mothers of term neonates with early-onset GBS sepsis received intrapartum prophylactic antibiotics <4 hours pre-delivery and one >4 hours pre-delivery, as compared to preterm labour where the majority received IAP >4 hours before birth.
Conclusion: Our study findings, including our experience of the GBS3 trial, demonstrated that EOGBS at term is preventable by knowing maternal GBS status and offering IAP during labour. Prematurity remains a risk factor for early-onset GBS infection and a current focus of NHS care bundles (SBCB). Whilst the results of the GBS3 trial are awaited, we hope to raise awareness among the public and wider NHS by sharing our results.
The exploration of late-onset disease infection route of Group B Streptococcus by polymerase chain reaction (PCR)
Emiko Yoshida1, Jun Takeda1, Yojiro Maruyama2, Naoko Suga3, Shintaro Makino3 and Atsuo Itakura1
1Juntendo University, Department of Obstetrics and Gynecology, Tokyo, Japan, 2Juntendo University, Nerima Hospital Department of Obstetrics and Gynecology, Tokyo, Japan, 3Juntendo University, Urayasu Hospital Department of Obstetrics and Gynecology, Tokyo, Japan
Objectives: Group B Streptococcus (GBS) is a pathogen causing life-and-neurodevelopmental-threatening and bacterial infections in newborns. Nationwide surveillance study between 2016 and 2020 in Japan had reported an increase in the number of cases mainly driven by an increase in late-onset disease (LOD). Prevalence of maternal GBS is unstable, so Rapid diagnosis of GBS at delivery is useful as a way to prevent GBS infection. We aimed to reveal the clinical features to explore transmission route of LOD.
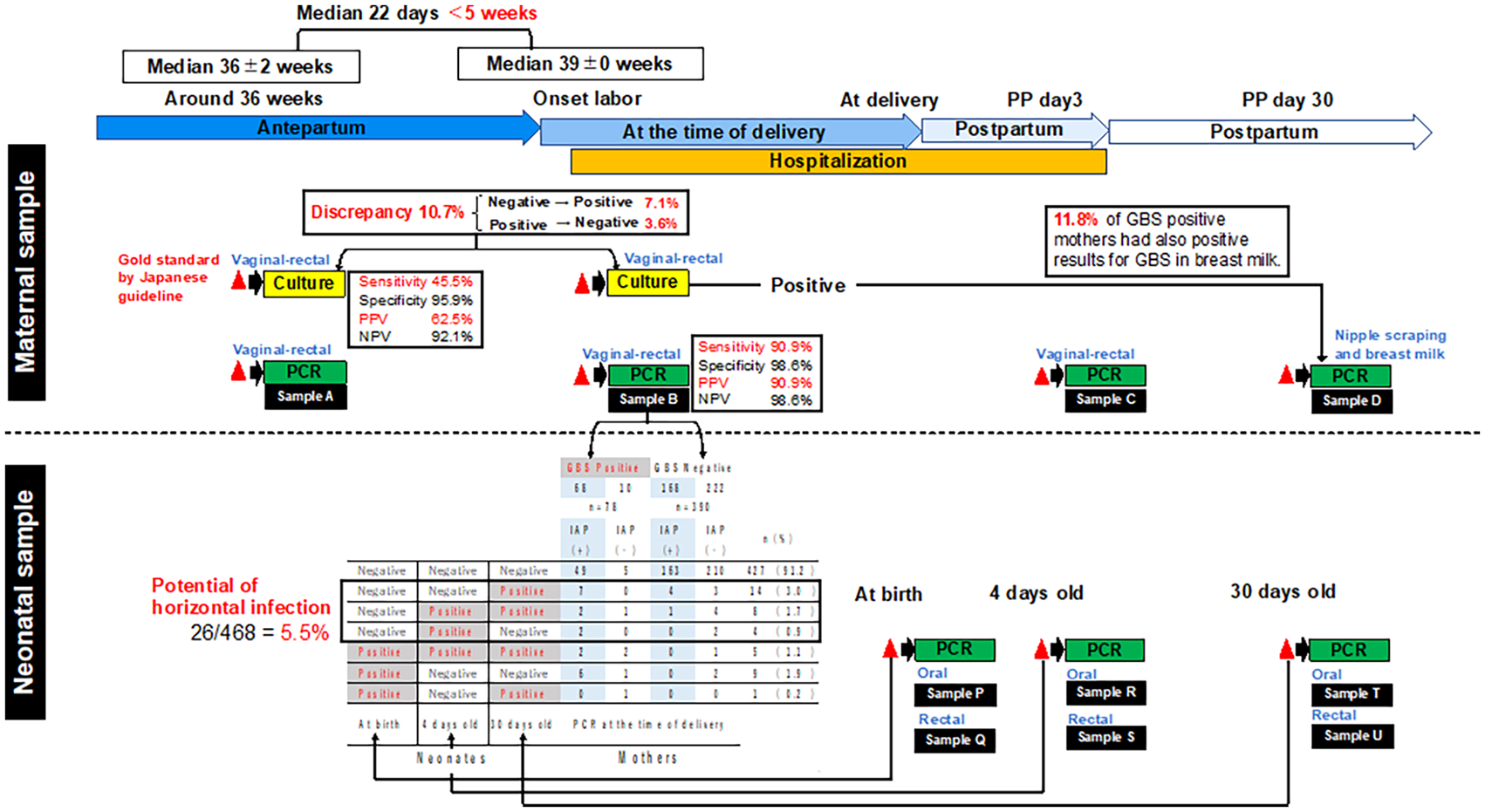
Methods: Vaginal-and-anorectal specimens were collected from 530 pregnant women at the time of antepartum, delivery or postpartum. Oral/anorectal specimens were collected from their newborns at the time of birth, day4, or day30. Each sample was tested by PCR and/or culture for GBS detection. The DNA for PCR was purified directly from the buffer that the swab specimens were suspended without enrichment cultivation.
Results: The antepartum prevalence of maternal GBS was 18.6% according to PCR, and 16.1% according to cultures. In 10.7% of cases, GBS results on culture were inconsistent with antepartum and delivery (Figure 1). The ratio of detected GBS capsular types differed between mothers and neonates, type V was the most in mothers and type Ia was the most in neonates. GBS was detected in 3.6% of neonate even from GBS negative mother.
Conclusion: As previously reported, PCR showed superior in detection to culture. GBS positive neonate with negative mother suggests horizontal infection after birth. Our method is a direct detection without an enrichment cultivation, suggesting the possibility of point of care testing on the onset of the delivery. We are developing GenPad system based on the isothermal PCR, SmartAmp, as the rapid high-sensitive fully automatic POCT system to fulfill the requirement (Figure 2).
The scheme for sampling and the relation between maternal and neonatal GBS.
The rapid high-sensitive fully automatic POCT system.
Distribution of serotypes and antibiotic resistance patterns among GBS strains recovered from anovaginal samples of pregnant women and human semen samples
Ana Clarisse Merces1, Natália Silva Costa1, Laylla Graça Barros1, Laura Maria Andrade Oliveira1, Ana Caroline Nunes Botelho1, Sérgio Eduardo Longo Fracalanzza1 and Tatiana Castro Abreu Pinto1
1Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
Background & objective:Streptococcus agalactiae (GBS) is one of the main agents of human infections, especially in pregnant women and newborns. However, little is known about the role of GBS in human semen, as strains from this source have not yet been completely characterized. Therefore, the objective of this study was to characterize and compare serotype distribution and antimicrobial resistance profile between 39 GBS strains obtained from anovaginal clinical samples of pregnant women and 38 GBS strains isolated from semen between 2017 and 2018 in Brazil.
Methods: The identification of GBS strains was carried out using conventional techniques, including the CAMP test and hippurate hydrolysis. Confirmation of identification was performed by MALDI-TOF MS. Capsular typing was determined by latex agglutination using a commercial kit, and susceptibility profiles were determined by the disk diffusion method according to CLSI.
Results: All strains were positive in the CAMP test and were able to hydrolyze hippurate. Furthermore, species-level identification was confirmed by MALDI-TOF MS. Regarding the distribution of serotypes in anovaginal strains, serotype Ia was the most common (45.5%), followed by Ib (18%), II (17.5%), V (11%), and III (8%). Regarding the susceptibility profile, resistance to tetracycline, erythromycin, clindamycin, and levofloxacin was observed in 84.2%, 13.2%, 5.3%, and 1% of the isolates, respectively. Furthermore, 5.2% of the strains showed resistance to three or more classes of antimicrobials. In semen strains, the prevalent serotype was V (45%), followed by Ia (23%), III (13%), II (10%), and IV (1%). Resistance to tetracycline, erythromycin, clindamycin, and levofloxacin was observed in 87.2%, 23.7%, 7.7%, and 5.2% of the strains, respectively. Multidrug resistance was observed in 7.6% of the strains. In Brazil, serotype Ia is commonly the most prevalent in samples from pregnant women, and serotype V is reported to be the most commonly found in infections in non-pregnant adults. This may explain why V was predominant in the semen strains. Regarding susceptibility to antimicrobials, it is worth highlighting that resistance to levofloxacin, although rare, has already been reported in Brazil at levels of 1% to 7.1%. Therefore, the resistance presented in this study for the strains is in accordance with the literature.
Conclusion: Serotype V was the most common in semen strains while serotype Ia was the most common in anovaginal strains and the second most common in semen. Semen strains, in turn, presented higher rates of antibiotic resistance.
Group B Streptococcus and Methicilin-Resistant Staphylococcus Co-colonization Among Pregnant Women in Brazil
André Rio-Tinto1, Natália Silva Costa1, Isabella Pinto1, Laura Oliveira1, Sergio Fracalanzza1, Lucia Teixeira1, Penelope Marinho2, Joffre Amim Jr1, Stephen Taylor3, Stephen Thomas3 and Tatiana Pinto1
1Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio Janeiro, Rio de Janeiro-RJ, Brazil, 2Maternidade Escola, Universidade Federal do Rio Janeiro, Rio de Janeiro-RJ, Brazil, 3UK Health Security Agency, UK
Introduction: Group B Streptococcus (GBS) is a main cause of neonatal infections, while methicillin-resistant Staphylococcus spp. (MRS) has been increasingly associated with neonatal infections. Both can colonize the anovaginal tract of pregnant women, which is the main source of vertical transmission. Clinical trials of GBS vaccines are already underway, however little is known about the potential impact of GBS vaccination in the anovaginal microbiota.
Objectives: Our aim was to evaluate the co-colonization of GBS with MRS among pregnant women attending a single maternity in Rio de Janeiro, Brazil, between January 2019 and August 2022.
Methods: Anovaginal samples were streaked onto chromogenic media and blood agar after a pre-enrichment step, and colonies were identified by MALDI-TOF MS. GBS serotypes were determined by latex agglutination. Antimicrobial susceptibility was evaluated according to CLSI. Detection of mecA gene was assessed by PCR.
Results: Overall, 1324 pregnant women were included in this study, and 8.5% (113) were positive for GBS. Serotypes Ia (34.5%), V (26.5%) and II (15%) were the most prevalent. Among the GBS positive participants, 47.8% (54) were also colonized by MRS, in which S. haemolyticus was the most prevalent species (90.7%; 49). Non-susceptibility to erythromycin was highly present in MRS strains (74.1%; 40), followed by non-susceptibility to tetracycline (24.1%; 13). Of the MRS strains, 33.3% were resistant to at least 3 different classes of antibiotics (MDR).
Conclusion: In conclusion, cases of co-colonization of GBS with MRS could indicate that the presence of drug resistant opportunistic pathogens in the anovaginal region may increase in this niche upon reduction of GBS colonization after vaccination.
Funding
This work was supported by the Bacterial Vaccines (BactiVac) Network (funding number is BVNCP4-10); and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES)—Finance code 001, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) (funding numbers are E-26/211.554/2019 and E-26/010.002141/2019).
Footnotes
Only minor formatting alterations have been made and the abstract content remains consistent with what was entered at time of submission by the author(s).