
Abstract
Background:
The COVID-19 pandemic constitutes a global health threat and poses a major burden on the African continent. We assessed the real-world burden of COVID-19 infection in African Union (AU) member states to determine the distributional patterns of epidemiological measures during the first 1 year of the pandemic.
Methods:
This retrospective cross-sectional study utilized COVID-19 data from publicly available data repositories of the African Center for Disease Control and Prevention and Our World in Data for the period February 2020 to January 2021. AU member states were classified into low, medium, and high burdens based on COVID-19 morbidity. We conducted descriptive and inferential analyses of COVID-19-reported cases, deaths, recoveries, active cases, COVID-19 tests, and epidemiological measures that included morbidity and mortality rates, case fatality rate (CFR), and case ratios.
Results:
A total of 3.21 million cases were reported during the 1-year period, with 2.6 million recoveries, 536,784 cases remaining active, and 77,486 deaths. Most countries (49.1%, n = 26) in AU experienced a low burden of COVID-19 infection compared to 28.3% (n = 15) with medium burden and 22.6% (n = 12) with high burden. AU nations with a high burden of the disease were mainly in the northern and southern regions. South Africa recorded the highest number of cases (1.31 million), followed by Morocco with 457,625 and Tunisia with 175,065 cases. Correspondently, death tolls for these countries were 36,467, 7888, and 5528 deaths, respectively. Of the total COVID-19 tests performed (83.8 million) during the first 1 year, 62.43% were from high-burden countries. The least testing occurred in the medium-burden (18.42%) countries. The overall CFR of AU was 2.21%. A morbidity rate of 327.52/105 population and mortality rate of 5.96/105 population were recorded during the first 1-year period with significant variations (p < 0.0001) across burden levels. Continental morbidity and mortality rates of 17,359/105 and 315.933/105 populations were recorded with significant correlation (r = 0.863, p < 0.0001) between them and variations across selected epidemiological measures by COVID-19 burden levels.
Conclusion:
Understanding the true burden of the disease in AU countries is important for establishing the impact of the pandemic in the African continent and for intervention planning, preparedness, and deployment of resources during COVID-19 surges and future pandemics.
Keywords
Introduction
Since the outbreak of the COVID-19 pandemic in Wuhan, China in December 2019, it has remained a threat to public health worldwide, including in African countries.1–3 Due to the close ties of African countries with China and other affected countries, there was anticipation of the importation of the virus to the continent of approximately 1.3 billion people. 4 Eventually, the first COVID-19 case in Africa was reported in Egypt on 14 February 2020,5,6 which makes Africa the last continent to be hit by COVID-19. 7 Subsequently, Algeria and Nigeria reported their first cases on 25 February 2020, and 27 February 2020, 8 followed later by most other African countries, including South Africa, Ghana, Morocco, and Cameroon, that detected their first cases in March 2020. 8 As with the rest of the world, initial cases were imported from other regions, followed by local transmission. 9
Africa, despite being the last continent to be hit by the pandemic, was described as the most vulnerable to a public health and economic catastrophe.5,10–12 These projections were based on the continent’s weak healthcare systems and a large immunocompromised population owing to the high prevalence of malnutrition, anemia, malaria, HIV/AIDs, tuberculosis, and poor economic discipline, social lifestyle, fragile infrastructure, inadequate availability of trained personnel, insufficient funding, inefficient data transmission as well as reduced access to medical supplies and equipment in the continent.5,11,12 Experts also anticipated that under these circumstances, the pandemic in Africa could be challenging to control and that the consequences could be dismal. 11
With the lessons on the pandemic learned from other continents and from the previous outbreaks, African countries acted urgently on specific gaps and put in place stricter measures of detection, prevention, and control.4,5,8 Many governments in Africa enacted early response measures to the pandemic that included complete and partial lockdowns, travel restrictions, the closing of schools, bans on large gatherings, isolation and quarantine policies, increased testing capacity, and strict infection control measures.8,10 The African Center for Disease Control and Prevention (African CDC), working with the World Health Organization (WHO), seized this window of opportunity to rapidly mobilize a continent-wide response. The African Task Force for Coronavirus (AFCOR) was established by the African CDC to work with the African Union Commission (AUC) and the WHO to manage the treatment of COVID-19 patients as well as proposed interventions.1,8,9 AFCOR worked diligently to deliver on six work streams, namely laboratory diagnosis and subtyping; surveillance, including screening at points of entry and cross-border activities; infection prevention and control in healthcare facilities; clinical management of severe COVID-19; risk communication; and supply chain management and stockpiles.8,9 These public health and social measures helped to control and slow down the spread of COVID-19 in the African continent while affording extra time to prepare.
Despite the initial worst-case scenarios epidemic model prediction of the COVID-19 pandemic in the African continent,2,13 there was a general sense of optimism – in part driven by the low numbers of COVID cases – that Africa could have been spared the worst effects of the pandemic.13,14 This was short-lived as the devastating consequences of the COVID-19 pandemic on the African continent in terms of direct case burden, morbidity, mortality, and marked socioeconomic disruption later became evident.1,13,15–17 As of June 2020, 10 out of 54 countries were driving the rise in numbers, accounting for nearly 80% of all the cases, with more than 70% of the deaths taking place in only five countries: Algeria, Egypt, Nigeria, South Africa, and Sudan. 18 By the 3rd of September 2020, the continent had more than 12 million symptomatic cases and 30,000 deaths, with a 24% case fatality, representing 5% of global infections. 6 During this period, vaccines were still in the development phase, and COVID-19 variants had not been detected yet.
Several research studies have attempted to assess the dynamics of the COVID-19 pandemic in the African continent and to understand the true burden of the disease since the first case was reported in Egypt on 14 February 2020.1–3,5–10,13,15,16,19–24 However, most have been restricted in scope to country or subregion because of scarce primary information or do not reflect country-specific adaptive factors.10,15,16,22,24 None have attempted to evaluate the burden of the disease across African countries during the first 1 year of the pandemic. Understanding the impact of the pandemic across African countries could help build on specific gaps experienced in the first 1 year and provide a more practical road map for future pandemic preparedness and response efforts. On the above premise, our current study attempts to assess the burden of COVID-19 infection in African Union (AU) member countries and to highlight the distributional patterns of the epidemiological measures of the disease across countries and regions during the first 1 year of the pandemic.
Methods
Study population
Africa is the second largest and second most populous continent on earth. With an estimated population in 2021 of 1.39 billion people and a population density of 45.30 persons per km 2 , it accounts for about 16% of the world’s human population. 25 The population growth rate in most African countries is in the range of 2.0−2.55% per year.25,26 In addition, within the African population, it is estimated that a high proportion of people are under the age of 15 years, while another 19% are between the ages of 15 and 24. 27
Data source
The COVID-19 data used for this study were sourced from publicly available data repositories of the African CDC 21 and Our World in Data 28 from February 2020 to January 2021. Data obtained from the African CDC were accumulated daily from reports received from the Official Regional Collaborating Centre and 53 AU Member States within the five major geographic regions, namely Northern, Central, Western, Eastern, and Southern regions. 21 The variables identified in the dataset included the name of the country, population, geographic region, confirmed reported cases (RC) of COVID-19 infection, active cases (AC), recoveries (R), and deaths. COVID-19 test data were not available in the African CDC data repository and, therefore, were augmented with test data obtained from the Our World in Data repository for the same period. 28
Epidemiological measures
Based on the data obtained, the following epidemiological measures were assessed namely morbidity and mortality rates (MMRs), case fatality rate (CFR), and case ratios. 29 Morbidity and mortality rates were defined as measures of the frequency of occurrence of positive COVID-19 cases and deaths from COVID-19 infection, respectively, in a defined population during a specified interval. 30 CFR was defined as the proportion of death among those infected with COVID-19 within the specified period, and the resulting ratio was then multiplied by 100 to yield a percentage. CFR measures the severity of the COVID-19 disease in each country or region. Furthermore, the ratios of R and AC against the number of RC were determined by dividing the R and AC by RC. Because of the absence of data for estimating the traditional measures such as years of life lost and years of life lived with disability, 31 the burden of COVID-19 infection in our study was estimated based on the morbidity data following the first wave of the pandemic in Africa as follows: countries with COVID-19 morbidity rate of less than 100 per 105 population were classified as ‘low’, those with a morbidity rate of 100–349 per 105 population were classified as ‘medium’, while countries with a morbidity rate of 350+ per 105 population were designated as having ‘high’ burden of the COVID-19 infection. This measure was crucial to understanding the early dynamics of the COVID-19 pandemic and evaluating the impact and trajectory following the first wave. This classification formed the foundation for subsequent assessments of the epidemiological measures and the public health impact of the COVID-19 infection in the AU member states.
Statistical analysis
Preliminary data analysis involved descriptive analysis of the epidemiological measures. Subsequently, we performed an analysis of variance to determine whether there were differences in epidemiological measures of COVID-19 infection by the low, medium, and high burden of COVID-19 infection. Where significant differences existed within the factors, post hoc tests were conducted using Tukey’s Honestly Significant Difference procedure to compare the epidemiological measure means. To examine the pairwise relationships among the epidemiological measures, we conducted Pearson correlation analyses within the disease burden groups. All parameters of interest could not be considered together in the correlation analysis due to collinearity and, thus, were analyzed separately. 32 In addition, graphical representations were used to assess the distributional patterns of the epidemiological measures of interest across AU member nations by the burden of COVID-19 infection. All statistical tests conducted were two-tailed, and a probability value of ⩽0.05 was used as the minimum threshold for declaring statistical significance. Data management, statistical analysis, and visualizations were conducted using SAS JMP Statistical Discovery™ Software version 16.2 (SAS Institute, Cary, NC, USA). This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.33,34
Results
Burden of COVID-19 infection in AU
Figure 1 depicts the burden of COVID-19 infection in AU countries during the first 12 months of the pandemic. The majority of the countries in AU (49.1%, n = 26) were considered to have a low burden of COVID-19 infection compared to 28.3% (n = 15) of AU member countries with a medium burden and 22.6% (n = 12) with a high burden of the disease. Geographically, AU nations with a high burden of COVID-19 infection were mainly in the northern (n = 4; Tunisia, Morocco, Mauritania, and Libya) and southern (n = 4; South Africa, Namibia, Eswatini, and Botswana) regions. By contrast, most countries with a low burden of the disease were in the western (n = 9) and eastern (n = 9) regions of the continent (Figure 2). Countries, where the burden of the disease was reported to be medium, were identified in all the regions, with most in the western region (n = 4) and the least in the central (n = 2) and northern (n = 2) regions.
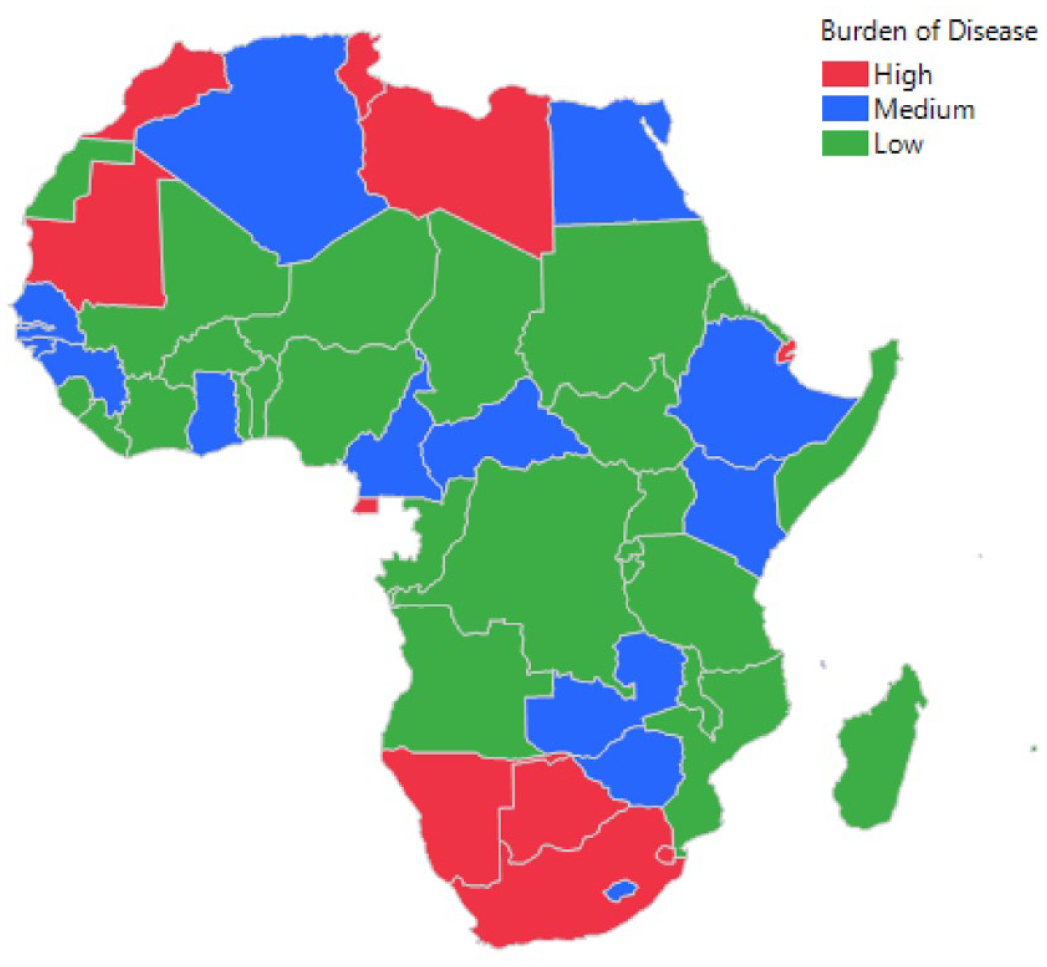
Map of Africa showing the burden of COVID-19 pandemic in AU member nations, 2020–2021.

Reported, recoveries, and active cases of COVID-19 in AU member countries by the burden of COVID-19 infection.
Epidemiological measures by the burden of COVID-19 infection
Reported cases, recoveries, and active cases
The epidemiological measures of COVID-19 infection in AU by the burden of the disease are presented in Table 1. A total of 3.2 million cases were reported to the African CDC between February 2020 and January 2021, with about 2.6 million recoveries, 536,784 cases remaining active, and 77,486 deaths recorded during the period. Significant variations (p < 0.05) existed in the burden of COVID-19 infection in the AU, with mean RC, R, and AC being higher among high-burden nations, followed by those with a moderate and low burden of the disease. South Africa recorded the highest number of cases (1.31 million), followed by Morocco with 457,625 and Tunisia with 175,065. Similar trends were noted for R and AC in these countries. By contrast, the highest number of RC in the low-burden group was from Nigeria (107,345), followed by Uganda (38,085) and Sudan (25,730). Figure 2 shows the distribution of RC, R, and AC in AU member countries by the burden of the COVID-19 infection. A summary of epidemiological measures of the COVID-19 pandemic in AU member countries is displayed in Supplemental Table 1.
Epidemiological measures of COVID-19 infection in AU by the burden of COVID-19 infection.

Burden of COVID-19 infection: low, n = 26 countries; moderate, n = 15 countries; high, n = 12 countries. Within the burden of COVID-19 infection, means with different superscripts (a, b, c) are statistically different (p < 0.05).
Billion; Pop: Population.
As a percentage of the total COVID-19 tests conducted in AU during the period under review.
Significance level: *p < 0.05; ****p < 0.0001.
AC, active cases; AU, African Union; CFR, case fatality rate; R, recoveries; RC, reported cases.
COVID-19 tests
A total of 83.8 million COVID-19 tests were performed in the AU States during the first 1 year of the COVID-19 pandemic (Table 1). Of this number, the high-burden countries had the most COVID-19 tests (62.43%, n = 52.3 million), compared to low- (19%, n = 16 million) and medium- (18.42%, n = 15.4 million) burden countries (p < 0.0001). There were significant (p < 0.0001) differences in COVID-19 tests by the burden of the disease, being 7.208, 9.009, and 43.314 per 1000 people for low-, medium-, and high-burden countries, respectively. More COVID-19 tests were conducted in the southern (48.9%, n = 41.0 million) and northern (21.9%, 18.4 million) regions of the continent. The least tests representing 13.5% and 15.7%, were performed in the western and eastern regions of the continent, respectively (Supplemental Table 2).
COVID-19-related deaths
As expected, there were more deaths in the high-burden countries compared to those from the medium- and low-burden groups (Table 1). Despite the high numerical variations, we recorded no statistically significant differences across the burden levels for the number of COVID-19-related deaths (p = 0.0685). However, during the period under review, the highest death toll was noted in the high-burden countries, with South Africa leading with 36,467 deaths, followed by Morocco with 7888 and Tunisia with 5528 deaths. The number of COVID-19-related deaths in the population of AU member countries by the burden level of the COVID-19 pandemic is depicted in Figure 3.
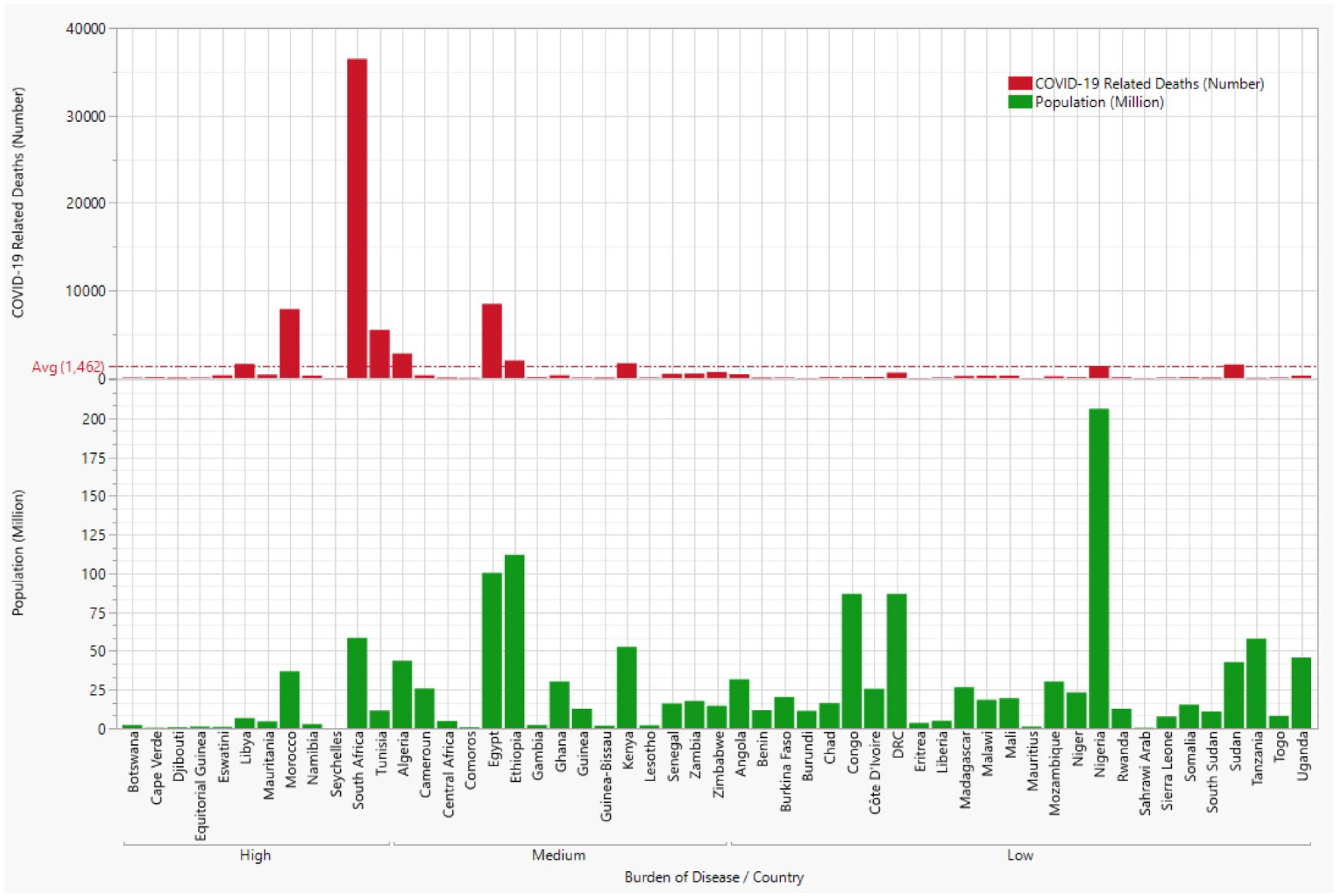
A number of COVID-19-related deaths overlaid the population of AU member countries by the burden of the COVID-19 pandemic.
R/RC and AC/RC ratios
The overall mean ratios of R/RC and AC/RC were 0.767 and 0.211 (Table 1). The R/RC ratio ranged from 0.740 in medium-burden to 0.838 in high COVID-19-burden countries, while the AC/RC ratio ranged from 0.145 in high-burden to 0.239 in medium-burden countries. However, there were no statistically significant (p > 0.05) differences in the ratios by the disease burden. Figure 4 shows the distribution of the R/RC and AC/RC ratios across AU member nations by COVID-19 burden.

Ratios of active cases (A/C) and recoveries (R), and reported cases (RC) of COVID-19 in AU member countries by the burden of COVID-19 infection.
Morbidity and mortality rates
The overall COVID-19 morbidity rate for the continent during the period under review was 17,359 per 100,000 population (pop) (mean = 327.52/100,000 population) (Table 1). Morbidity rates varied significantly (p < 0.0001) and were higher in the high-burden countries (1146.16/105 population) compared to the low-burden countries (43.38/105 population) (Table 1). Mortality rates followed the same pattern, with an overall rate of 315.933/105 pop (mean = 5.96/105 population) recorded for AU. The mean mortality rate in high-burden AU member nations (mean = 20.12/105 population) was about 23, and six times (p < 0.0001) more than those of low (0.872/105 population) and medium (3.45/105 population) COVID-19-burden nations. Within high-burden countries, South Africa recorded the highest mortality rate of 62.27/105 population, followed by Tunisia with 47.29/105 population and Eswatini with 29.88/105 population. Mortality rates for countries with a medium burden of COVID-19 infection generally ranged from 1.12/105 population in Ghana to 6.45/105 population in Algeria. The distribution of the mean MMRs for each AU member nation by the burden of the disease is presented in Figure 5.

Morbidity and mortality rates of COVID-19 in AU member countries by the burden of COVID-19 infection.
Case fatality rate
The overall reported CFR for the AU was 2.21% with no significant difference (p > 0.3195) noted across the disease burden levels (Table 1). However, low-burden countries, on average, tended to have a higher CFR (2.57%), while the lowest average CFR of 1.63% was reported in high-burden AU countries. For instance, the highest CFR of 11.76% was reported for Sahrawi Arab, followed by Sudan at 6.13% (both low-burden countries), and Egypt with a CFR of 5.48% (medium-burden country). By contrast, CFR of 2.78% and 3.16% were recorded for South Africa and Tunisia, both in the high-burden groups. Figure 6 shows the distribution of CFRs in AU member countries by the burden of COVID-19 infection.
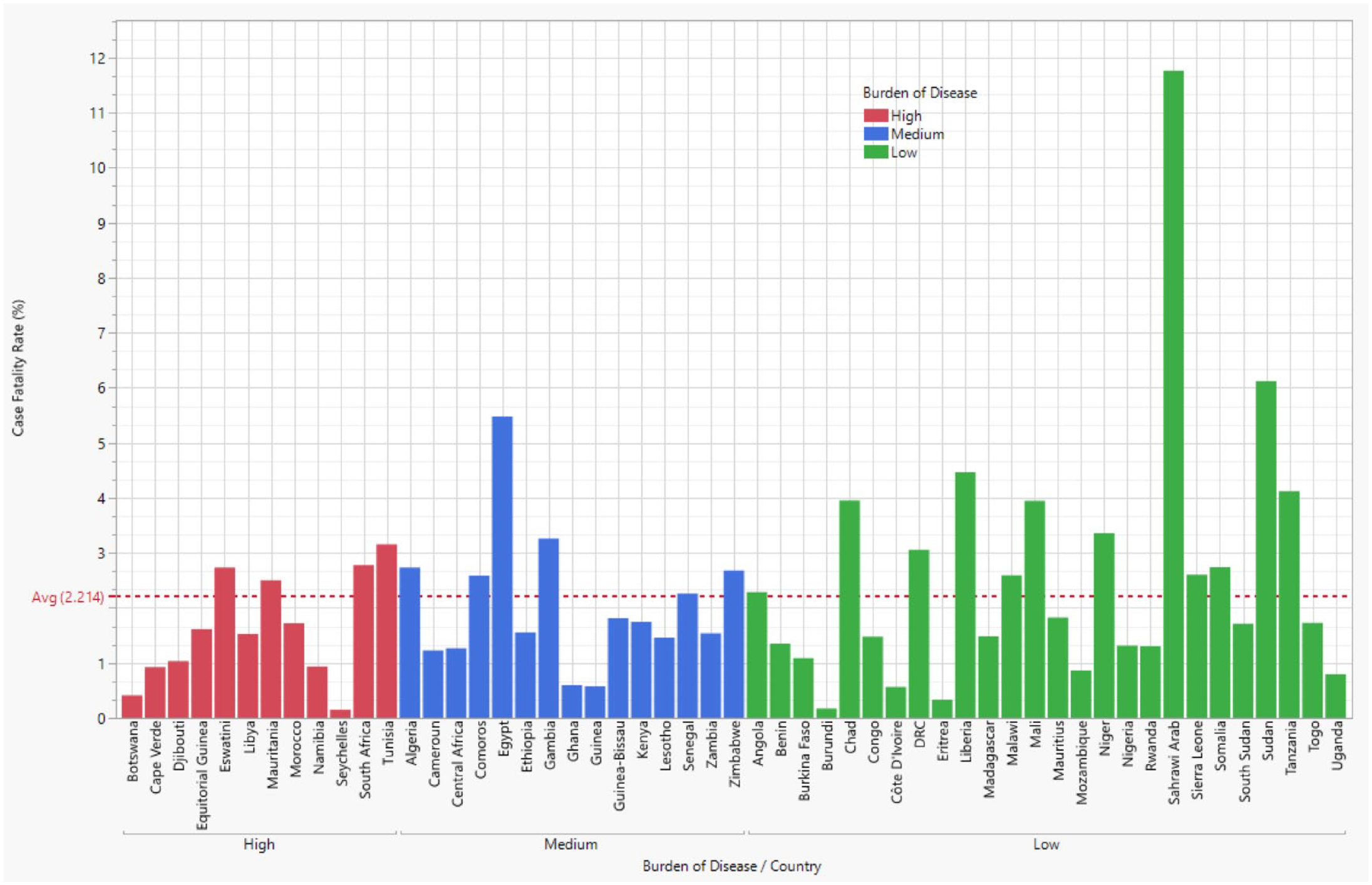
Case fatality rates of COVID-19 in AU member countries by the burden of COVID-19 infection.
Correlation among selected epidemiological measures
The correlation analysis among selected epidemiological measures in the AU by the burden of COVID-19 infection is presented in Table 2. MMRs in the AU were significantly (r = 0.863, p < 0.0001) correlated. We also noted a significant relationship between CFR and morbidity rate (r = −0.417, p = 0.0339) and CFR and mortality rates (r = 0.397, p = 0.0446) in the low-burden African countries. Of all measures assessed, only the mortality rate was significant and highly correlated (p < 0.0001) with the CFR (r = 0.915) among countries classified under medium COVID-19 burden. However, in the high-burden countries, MMRs were significantly correlated (r = 0.752, p = 0.0048), and likewise, mortality and CFRs (r = 0.757, p < 0.0044). Similarly, the population of the high-burden countries was also significantly correlated with the mortality rates reported during the first 12 months of the COVID-19 pandemic being 0.719 (p = 0.0084). However, further relational analysis carried out indicates that although expectedly RC, recoveries, and deaths were highly significantly (p < 0.0001) correlated with each other (r = 0.93–1.0), they were not significantly associated with the African countries’ populations (p > 0.05) (results not shown).
Correlation among selected epidemiological measures of COVID-19 infection in AU by the burden of COVID-19 infection.

Burden of COVID-19 infection: low, n = 26 countries; moderate, n = 15 countries; high, n = 12 countries.
Significance level: *p < 0.05; **p < 0.01; ****p < 0.0001.
AU, African Union; Pop, population; r, correlation coefficient.
Discussion
Since the SARS-CoV-2 was declared a pandemic on 11 March 2020, by WHO, 19 the public health and social impact of the disease have evolved to be enormous. The burden of the disease has been felt globally by every continent, country, population, people, and demographics, either directly or indirectly.2,11,15,16,20 Findings from our study indicate that almost half (49.1%) of the AU member countries experienced a low burden of the disease, while 22.6% were designated as high-burden countries. Geographically, AU nations with a high burden of COVID-19 infection were mainly in the northern (Tunisia, Morocco, Mauritania, and Libya) and southern (South Africa, Namibia, Eswatini, and Botswana) regions. A total of 3.2 million cases were reported in the continent, with about 2.6 million recoveries, 536,784 active cases, and 77,486 deaths during the 1-year period. The Americas, Europe, and Asia have greater burdens of COVID-19-confirmed cases and higher mortality rates than the African continent.2,21
During the period under review, the highest death toll was noted in the high-burden countries, with South Africa leading with 36,467 deaths, followed by Morocco with 7888 and Tunisia with 5528 deaths. The countries with high COVID-19 burden had the most COVID-19 tests compared to those classified as having low and medium burdens. The southern and western regions reported the most and least COVID-19 tests. Similar trends were previously noted by Awoyemi et al. 22 The testing rate in the African continent of 1.3 billion inhabitants is among the lowest in the world22,24,35 and has been implicated in the low infection rates and case fatalities.4,13,14 More tests (more than 17 million tests each) were, however, conducted in South Africa and Morocco during the first 1 year of the COVID-19 pandemic (SM1) compared to other countries. In some African countries, there were insufficient or no data available on the number of tests completed. This may indicate that little effort and few resources were directed toward COVID-19 testing, surveillance, and data management,2,7,8,10 during the first 1 year of the pandemic. For instance, the WHO estimates that the number of people infected with COVID-19 from the onset of the pandemic to November 2021 would be 61.2 million, against the reported 8.7 million cases. 23
The underlying cause for the significant epidemiological heterogeneity of COVID-19 infection and the relatively lower infection rates in the different African countries remains unknown. 35 Several explanations have been advanced for lower COVID-19 infection rate, which includes, among others, the timing of the introduction of the SARS-CoV-2 virus, different preparedness and response measures, experience with previous epidemics and pandemics, differences in the capacity of the health systems for testing and contact tracing, demographic factors, low seeding rate due to the low volume of travel to Africa, climate and environmental factors, host genetics, and social factors that determine adherence to public policies.2,5,13,22–24,35–39 Also, the stigma associated with COVID-19 is so great that infected people are reluctant to come forward for health care and are unwilling to disclose the names of others with whom they have been in close contact, 6 thereby hampering contact tracing. Epidemiological studies have indicated a lower incidence of COVID-19 in malaria-endemic areas in Africa.37,38
The MMRs varied significantly across countries, burden levels, and regions but were generally lower than those reported in other countries and continents.39,40 Various hypotheses have been advanced to explain the relatively low morbidity and mortality of SARS-CoV-2 in Africa,2,5,13,22–24,35–39 including differences in testing in the countries. 41 Current data suggest that COVID-19 affects older people severely, with higher mortality than the younger population, which showed only milder symptoms. 42 The median age in Africa is less than 20 years, which makes the continent the youngest in the world and seems to be an advantage when compared to other COVID-19-affected regions.8,42 For instance, only 4% of Africa’s population is older than 65, which is low as compared to 37% in Eastern and South-Eastern Asia and 29% in Europe and North America. 43 Young people are often known to be asymptomatic or have mild symptoms that can be missed by targeted surveillance and testing, 40 and thus, may contribute to overall lower MMRs in the African continent.
The overall first 1-year CFR for the AU was 2.21% with 3.2 million confirmed cases and 77,486 deaths. This value is comparable to the CFR of 2.4% reported in the continent in September 2020, 6 and in Asia,43,44 and lower than the CFRs for the Americas and Europe. 39 WHO reported that the global CFR for COVID-19 of 2.0% in November 2021 is much lower than that of the Ebola virus (various outbreaks, 25−90%), but COVID-19 has caused more deaths than all the Ebola Virus outbreaks combined.23,44 With more testing, more people with milder cases may be identified, which would help to lower the CFR. 42
The COVID-19 morbidity rate in AU was positive and significantly correlated with the mortality rate, and this finding corroborates with that obtained by Awoyemi et al. for 21 African Countries, 22 and Kodera et al. in Japan. 45 Our study further noted a strong positive relationship between CFR and mortality rates at all the COVID-19 burden levels. On the other hand, the mortality rate was the only significantly correlated measure (r = 0.719, p < 0.0084) with the population in the high-burden countries. This suggests that with population data, the number of cases and deaths in the high-burden area of the continent can be estimated, allowing for medical resource needs planning, thereby avoiding the potential spread of the disease. Although expectedly, RC, recoveries, and deaths were highly significantly (p < 0.0001) correlated with each other. Correlation coefficients of similar magnitude were obtained in an exploratory cross-sectional analysis of 21 African Countries. 22 However, these parameters were not significantly (p > 0.05) associated with the AU member states populations. This may reflect the limited resources, poor COVID-19 surveillance, and testing capacity’s inability to keep up with the continent’s population. These findings could be useful for intervention planning for potential COVID-19 surges or future pandemics.
Public health implications
COVID-19 brought with it an unprecedented health crisis, the response to which requires learning from past epidemic and pandemic experiences and generating new evidence to guide containment efforts.9,23,24,36 Although the African continent was not spared of the disease, the comparatively low number of confirmed cases and deaths noted in our current study and previous studies,39,40 contrasted the previously documented gloomy models and predictions during the early part of the pandemic. Njenga et al. argue that the low number of cases in Africa may not be an artifact of poor surveillance and low testing because an escalating number of COVID-19 cases would be easily detected through reports of pneumonia clusters, 39 but this has not been the case despite the high transmissibility of the virus demonstrated in Asia, Europe, and North America.24,35–37,39,43,46
There is no doubt that the late arrival of the outbreak offered the continent a window of opportunity for African countries to plan and prepare for the pandemic. The WHO Regional Office for Africa, in partnership with African governments and other stakeholders, immediately developed COVID-19 preparedness and response plans prior to reporting the first case, having learned lessons from the rest of the world on the critical nature of early containment measures. 23 Also, the lessons from past epidemics and pandemic experiences of African countries served as the source of guidance for the strategic implementation and promotion of public health intervention strategy, COVID-19 case management, infection prevention, and control.23,47,48 During the first 1 year of the COVID-19 pandemic, the first wave in Africa peaked between June and August 2020 and was driven by the community spread of the imported cases.21,23 The second wave peak occurred between December 2020 and February 2021 and was driven by the re-opening of airports in many African countries, which also coincided with the December holidays, where there was increased travel from urban to rural areas. 23 This likely contributed to the faster spread of the Delta variant in the third wave experienced in June/August 2021 in Africa. 46
Although the COVID-19 vaccine was still in development and the variants had not been detected yet as of the period covered by our current study, it is, however, worth mentioning the impact of the roll-out on combating the disease in Africa. About 49 African countries have so far rolled out COVID-19 vaccines, with more than 28 million doses already administered with an average continental coverage of 2.5%, an amount which is below the global average (20 versus 227 doses per 1000 people). 35 The use of available vaccines (⩾2 booster doses) will enhance antibody development and reduce the severity of the disease and the risk of death among all age groups.23,24 Amid the scramble for vaccines and the inequitable distribution between rich and poor countries, the Africa CDC continues to coordinate and mobilize resources to increase vaccine supply, address the challenges of vaccine hesitancy, and advocate for increased local production of COVID-19 and other vaccines.23,35 However, 52.3% of the continent’s population is estimated to have some SARS-CoV-2 immunity, given the low vaccination coverage of 14·7% as of 31 December 2021. 24 It must be reiterated that COVID is a global emergency that requires a global response and that no one can be safe until everyone is safe. 49 While care of critically ill COVID-19 patients has improved, African countries need to further strengthen their capacities to cope with a potential surge in cases sparked by a new lethal and transmissible variant. 43 This underscores the critical need to accelerate the provision of vaccine doses to vulnerable populations in developing countries. 50
Understanding the geographic regions with the highest disease burden will allow the African CDC, and indeed each country’s health ministries and establishments, to appropriately identify gaps, allocate medical resources, and adequately prepare for any potential COVID-19 surge or future pandemics. There is no doubt that the decreasing trends in the COVID-19 burden in 2022 are reducing the pressure on African countries’ public health resources and, thus, have allowed previously disrupted routine health services such as HIV and TB care and management, immunization, and other disease outbreaks surveillance to resume. Finally, the response to the COVID-19 pandemic across African countries has helped to reinforce key public health emergency response measures, including diagnosis and testing, critical care, and infection prevention and control. 43 Also, most countries in Africa require urgent assistance in upgrading the quality of their vital statistics systems to facilitate public health decisions and actions, not only for the COVID-19 pandemic but for future global health concerns. 50 It is believed that these improvements will continue to help each country monitor and control not only the COVID-19 pandemic but any other emerging infectious disease.
Study limitations and strengths
Our study findings are subject to several limitations. Data were collected from multiple sources, and data for countries were updated at the African CDC as they received them. Therefore, the number of RC and deaths from each country varied widely depending on the strength of each country’s surveillance system, data management, and reporting infrastructures, poorly resourced diagnostic laboratories, and lack of COVID-19 testing capacity. These limitations may have led to the underestimation of the actual number of cases and deaths. There was no standardized definition of a COVID-19-associated death across African countries, especially during the initial period of the pandemic. Thus, accuracy was hampered by delays in reporting deaths, and the lack of information on causes of deaths making it difficult to track ‘hot spots’ and leading to undercounting of COVID-19-related deaths. The WHO estimates that two-thirds of all deaths are unrecorded, with all low-income and most middle-income countries either collecting low-quality data or not recording deaths at all. 51 It is also possible that underreporting may not be the culprit for the low cases and death rates. 39 In general, the large variability in confirmed cases and deaths reported may directly affect the accuracy of our epidemiological measures leading to nonsignificant results in some cases, despite huge numerical differences noted. 52 Consequently, caution should be exercised in the interpretation of the outcomes and consideration given to the clinical relevance and implication of the findings, whether the results are statistically significant or not. 52 Finally, our data source did not capture the sociodemographic characteristics of affected persons making it impossible to assess the impact of social determinants of health indicators on the MMRs.
Despite the above limitations, the strengths of our study lie in the comprehensive cataloging of the COVID-19 morbidity and mortality data in the African continent during the first 1 year of the pandemic. Quantifying the health impacts of COVID-19 can help to determine the pandemic’s scale in African countries and inform resource deployment at the early stages of similar pandemics. During later phases, the data can also be used for predictive planning, risk mitigation, and other efforts to improve preparedness and strengthen public health systems to perform better during future pandemics. 53
Conclusion
Our findings indicated that although the African continent was the last to be hit by the COVID-19 pandemic, the disease quickly spreads to all countries within the first 1 year. The swift and appropriate response with sufficient capacity by African countries, despite their limited resources, helped to slow down the disease spread. However, the reported cases, recoveries, active cases, deaths, and other epidemiological measures evaluated were highly heterogeneous across African countries. Regardless of the worst-case scenario predictions for the African continent, our numbers showed that COVID-19 infections and deaths were much lower compared to those in the Americas, Europe, and Asia. It is also possible that the overall burden of COVID-19 infections in the African continent may be underestimated.
The comparatively high MMRs of COVID-19 in the Northern and Southern regions indicated that countries in those regions were worse hit by the pandemic. The current low testing capacity in the Central, Western, and Eastern regions in Africa, coupled with the poor reporting and vital statistics systems, do not provide strong evidence for the assessment of the true burden of COVID-19 in the regions. We recommend conducting well-designed seroprevalence studies in the continent to determine the true burden of COVID-19 and to understand both the sociocultural and immune response dynamics of SARS-CoV-2 infection under the heterogeneous African settings and contexts.
Supplemental Material
sj-docx-1-tai-10.1177_20499361231202116 – Supplemental material for Population-based assessment of the burden of COVID-19 infection in African countries: a first-year report card and public health implications
Supplemental material, sj-docx-1-tai-10.1177_20499361231202116 for Population-based assessment of the burden of COVID-19 infection in African countries: a first-year report card and public health implications by Osaro Mgbere, Ogbonna Collins Nwabuko, Olajumoke A. Olateju, Omolola E. Adepoju, Winston Liaw, Charles Darkoh and Ekere James Essien in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
We thank the various countries’ ministries of health and the Africa CDC for making available the data on COVID-19-confirmed cases, recoveries, active cases, and deaths. Our world in Data is also acknowledged for availing us of the COVID-19 test data used for this study. The findings and conclusions reached in this article are solely the responsibility of the listed authors and do not by any means represent the official position on the COVID-19 pandemic in Africa by the Africa Centers for Disease Control and Prevention or the African Union or Our World in Data or the institutions for which the authors are affiliated. All authors read and approved the final version of the manuscript, and consent to the article publication.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.